Paronychia: Comprehensive Surgical Management, Anatomy & Indications
Key Takeaway
Surgical drainage of paronychia is indicated for pus presence, failure of conservative management, subungual abscess, runaround infection, suspected osteomyelitis, or in immunocompromised patients. Understanding the perionychium's anatomy is crucial for accurate localization and optimal intervention, preventing complications and ensuring effective recovery from this prevalent hand infection.
Introduction and Epidemiology
Hand infections represent a significant source of patient morbidity, leading to substantial functional deficits and economic burden due to lost time from work. While advancements in medical care and antibiotic therapy have historically reduced the incidence of major hand infections, the re-emergence of serious infections, particularly in vulnerable populations including those with intravenous drug use, diabetes mellitus, and immunocompromising conditions, continues to challenge the field of hand surgery.
Paronychia is the most prevalent hand infection, comprising approximately 35% of all hand infections encountered in both emergency departments and specialized hand clinics. It is an inflammatory condition involving the nail fold, typically presenting as an acute or chronic infection of the perionychium. Acute paronychia is most commonly caused by bacterial inoculation, predominantly Staphylococcus aureus (with a rising prevalence of Methicillin-resistant Staphylococcus aureus or MRSA), often following minor trauma, nail biting (onychophagia), hangnail manipulation, aggressive manicuring, or occupational micro-trauma. Other relevant pathogens include Streptococcus pyogenes, and in cases involving oral flora exposure, mixed anaerobic and Gram-negative organisms such as Eikenella corrodens.
Chronic paronychia, conversely, is typically multifactorial and represents an eczematous or inflammatory dermatitis rather than a simple bacterial abscess. It involves a combination of environmental irritants, prolonged moisture exposure, repeated micro-trauma, and often secondary fungal colonization, predominantly Candida species. Occupational hazards strongly correlate with chronic paronychia, frequently affecting dishwashers, bartenders, healthcare workers, and agricultural personnel.
The principles governing the surgical treatment of paronychia are consistent with the broader management of hand infections: accurate localization of the infection, identification of the causative organism or pathology, and optimal timing of surgical intervention. Failure to adhere to these principles can lead to prolonged recovery, severe local complications such as felon extension or osteomyelitis, and permanent functional or aesthetic deficits of the nail unit.
Surgical Anatomy and Biomechanics
A thorough understanding of the perionychium and nail unit anatomy is paramount for effective diagnosis and surgical management of paronychia, minimizing iatrogenic injury to the delicate structures responsible for nail generation and fingertip sensation.
Components of the Nail Unit
The nail unit comprises several distinct anatomical structures that function synergistically:
* Nail Plate: The hard, keratinized structure that provides dorsal protection to the underlying distal phalanx and nail bed. It acts as a counter-force for the volar pulp during tactile pinch.
* Nail Bed: The highly vascular soft tissue beneath the nail plate, consisting of two distinct functional zones:
* Germinal Matrix: Located proximally beneath the eponychium, extending proximally to the insertion of the terminal extensor tendon. It is responsible for producing approximately 90% of the nail plate volume. Iatrogenic injury to the germinal matrix during incision and drainage will lead to permanent nail dystrophy, ridging, or split nail deformity.
* Sterile Matrix: Extends distally from the lunula (the visible distal extent of the germinal matrix) to the hyponychium. It is responsible for the firm adhesion of the nail plate to the underlying phalanx and contributes to the remaining 10% of the nail's thickness.
* Eponychium: The skin fold covering the proximal nail matrix, terminating distally in the cuticle (eponychial fold). Infection tracking under this fold from one lateral paronychium to the contralateral side is clinically designated as a runaround infection or eponychial abscess.
* Paronychium: The lateral nail folds, which are the specialized skin folds overlying the lateral borders of the nail plate. This is the primary anatomical site of acute paronychial abscess formation.
* Hyponychium: The specialized area of skin beneath the free distal edge of the nail plate. It provides a protective keratinous seal against proximal bacterial migration under the nail plate.
* Perionychium: The collective anatomical term encompassing all the soft tissues immediately surrounding the nail plate, including the eponychium, paronychium, and hyponychium.
Osteology and Fascial Compartments
The underlying distal phalanx provides rigid skeletal support. The base of the distal phalanx and the distal interphalangeal (DIP) joint are in close anatomical proximity to the proximal germinal matrix. Neglected proximal paronychial infections can directly extend into the DIP joint space, resulting in septic arthritis, or into the periosteum, causing osteomyelitis.
The volar pulp of the fingertip contains a dense fibrofatty septal network. These fibrous septa extend from the volar periosteum of the distal phalanx to the dermis, compartmentalizing the pulp to provide stability during pinch grip. While this compartmentalization aids in biomechanical rigidity, it also traps infections (felons), hindering their spontaneous drainage and leading to rapid increases in compartmental pressure, microvascular compromise, and subsequent soft tissue necrosis.
Neurovascular Supply
The digital arteries run along the lateral aspects of the digits, arborizing into a complex vascular plexus within the distal pulp and nail bed. The arterial supply to the nail fold forms a distinct proximal arcade. The dorsal branches of the proper digital nerves branch off at the level of the middle phalanx to provide critical sensation to the dorsal skin, including the eponychial and paronychial regions. Meticulous surgical technique, utilizing blunt dissection where appropriate, is essential to avoid transection of these superficial terminal nerve branches, which can result in painful neuromas.
Biomechanical Considerations
The intricate relationship between the nail plate, its surrounding soft tissues, and the underlying distal phalanx is crucial for both protection and fine tactile discrimination. The nail plate provides a rigid dorsal buttress that allows the volar pulp skin to deform around objects during pinch, maximizing sensory feedback via Pacinian and Meissner corpuscles. Swelling and fluctuance within the confined spaces of the perionychium rapidly increase local tissue pressure. This pressure compromises microcirculation, causing the severe, throbbing pain characteristic of acute paronychia, and impairs the biomechanical dexterity of the affected digit.
Indications and Contraindications
The decision to proceed with operative intervention versus conservative management relies on a careful clinical assessment differentiating between early cellulitis and frank abscess formation, as well as distinguishing acute bacterial infection from chronic inflammatory changes.
| Clinical Presentation | Operative Indications | Non Operative Indications |
|---|---|---|
| Acute Paronychia | Frank fluctuance or visible purulence under the eponychium/paronychium | Early erythema and swelling without fluctuance (< 24 to 48 hours duration) |
| Eponychial Runaround | Purulence extending across the proximal nail fold | Mild proximal fold erythema responsive to warm soaks and antibiotics |
| Subungual Abscess | Purulence tracking beneath the nail plate causing nail plate elevation | N/A (Subungual purulence requires decompression) |
| Chronic Paronychia | Refractory cases failing prolonged conservative management (requires marsupialization) | Initial presentation; management with topical steroids, antifungals, and avoidance of moisture/irritants |
| Complicated Infection | Suspected felon extension, osteomyelitis, or septic arthritis of the DIP joint | N/A (Requires emergent surgical exploration and debridement) |
Relative Contraindications to Surgery
True contraindications to the drainage of a paronychial abscess are exceptionally rare, as source control is the definitive treatment for confined purulence. However, relative contraindications and factors requiring preoperative optimization include:
* Severe Peripheral Vascular Disease: Digits with profound ischemia require careful consideration regarding the use of tourniquets and the extent of debridement to avoid precipitating digital gangrene.
* Uncorrected Coagulopathy: Severe bleeding diatheses should be medically optimized, though the superficial nature of paronychia drainage often allows for local hemostatic control.
* Absence of Fluctuance: Incising an area of pure cellulitis without a localized fluid collection provides no clinical benefit, increases the risk of iatrogenic injury, and introduces a portal for secondary nosocomial infection.
Pre Operative Planning and Patient Positioning
Clinical Evaluation and Diagnostics
Preoperative planning begins with a meticulous physical examination. The surgeon must assess for fluctuance, the extent of erythema, and signs of proximal spread (lymphangitis). The digit must be palpated circumferentially to rule out concurrent felon (volar pulp fluctuance or extreme tenderness).
Standard two-view radiographs (anteroposterior and lateral) of the affected digit are highly recommended prior to surgical intervention. Radiographs serve to rule out underlying osteomyelitis of the distal phalanx, identify radiopaque foreign bodies, and assess the integrity of the DIP joint.
Anesthesia
Adequate anesthesia is critical for a painless procedure and allows for thorough exploration and debridement. A digital block is the standard of care.
* Technique: A traditional ring block or a single volar subcutaneous injection at the base of the digit (transthecal block) can be utilized.
* Agents: 1% or 2% Lidocaine without epinephrine is historically preferred, often mixed with 0.5% Bupivacaine for prolonged postoperative analgesia. While modern evidence demonstrates the safety of epinephrine in digital blocks for healthy patients, it is generally avoided in patients with a history of digital ischemia, Raynaud's phenomenon, or severe peripheral vascular disease to prevent vasospastic complications.
Patient Positioning and Equipment
- Positioning: The patient is positioned supine with the affected upper extremity extended on a radiolucent hand table.
- Tourniquet: A bloodless field is essential for identifying the germinal matrix and avoiding iatrogenic injury. This is achieved using a sterile digital tourniquet (e.g., a commercial digital tourniquet or a Penrose drain clamped at the base of the digit). Care must be taken not to exceed 20-30 minutes of digital tourniquet time, and the surgeon must remember to remove it prior to dressing application.
- Instrumentation: A basic minor procedure tray is required, including a No. 11 or No. 15 scalpel blade, fine iris scissors, a Freer elevator or small periosteal elevator, straight hemostats, fine tissue forceps (Adson or micro-forceps), and aerobic/anaerobic culture swabs.
Detailed Surgical Approach and Technique
The surgical technique must be tailored to the specific anatomical location and chronicity of the paronychial infection. The overarching goal is complete decompression of the abscess cavity while meticulously preserving the germinal matrix and the integrity of the nail bed.
Acute Paronychia Simple Decompression
For an acute, localized abscess of the lateral paronychium without subungual extension:
1. Preparation: Following adequate digital block and application of the digital tourniquet, the digit is prepped and draped in a standard sterile surgical fashion.
2. Incision: The blade of a No. 11 scalpel is placed flat against the lateral aspect of the nail plate. The blade is advanced parallel to the nail plate into the lateral nail fold (paronychium).
3. Elevation: The blade or a Freer elevator is used to gently elevate the paronychial fold away from the nail plate. This maneuver typically enters the abscess cavity, resulting in the immediate egress of purulent material.
4. Avoidance of Matrix Injury: It is critical that the sharp edge of the blade is directed away from the nail bed and germinal matrix. No deep incisions should be made into the sterile matrix.
5. Debridement and Culture: A swab is taken for aerobic and anaerobic cultures. The cavity is gently explored with a blunt probe or Freer elevator to break up any loculations.
6. Irrigation: The cavity is copiously irrigated with sterile normal saline.
7. Packing: A small wick of plain gauze or iodoform gauze is loosely placed into the cavity to hold the paronychial fold open, preventing premature epithelialization and re-accumulation of purulence.
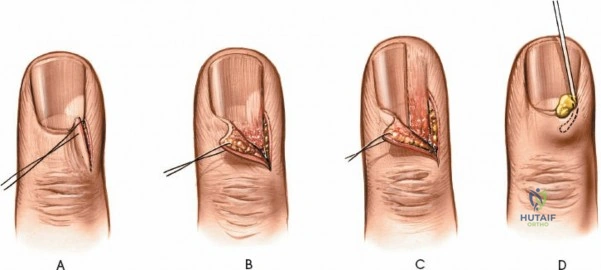
Eponychial Runaround Abscess Management
When the infection extends proximally across the entire eponychium:
1. Bilateral Incisions: Bilateral longitudinal incisions are made at the junction of the proximal eponychial fold and the lateral paronychial folds.
2. Eponychial Elevation: The entire proximal eponychial fold is gently elevated proximally using a Freer elevator. This exposes the proximal aspect of the nail plate and the underlying abscess cavity.
3. Decompression: Purulence is evacuated, and cultures are obtained.
4. Wound Management: The eponychial fold is packed open with a non-adherent dressing or a small piece of gauze tucked beneath the fold to facilitate continuous drainage.
Subungual Abscess Decompression
If purulence has tracked beneath the nail plate, causing elevation or floating of the nail:
1. Nail Plate Resection: The portion of the nail plate overlying the abscess must be removed to achieve adequate source control.
2. Partial vs. Total Removal: Using fine iris scissors or a Freer elevator, the affected lateral one-third of the nail plate is bluntly separated from the underlying sterile and germinal matrix. The scissors are then used to longitudinally split the nail plate, and the involved segment is extracted with a hemostat. If the subungual abscess involves the majority of the nail bed, a complete nail plate avulsion is indicated.
3. Matrix Protection: Extreme care must be taken during nail avulsion to avoid tearing the delicate sterile matrix.
4. Dressing: Following irrigation, a non-adherent dressing (e.g., Xeroform or Adaptic) is placed directly over the exposed nail bed to prevent desiccation and adherence of secondary dressings.
Chronic Paronychia Surgical Excision
Chronic paronychia that is refractory to prolonged conservative management (topical steroids, antifungals, avoidance of wet environments) requires surgical excision of the fibrotic, chronically inflamed eponychial tissue, a procedure known as marsupialization.
1. Incision Design: A crescent-shaped incision is designed over the dorsal aspect of the proximal nail fold (eponychium). The maximum width of the crescent is typically 3 to 5 millimeters, centered over the area of maximal induration.
2. Excision: The incision is carried down through the epidermis and dermis. The crescent of fibrotic tissue is excised en bloc.
3. Depth of Dissection: The dissection must remain superficial to the germinal matrix. The goal is to remove the chronically infected and fibrotic roof of the nail fold while leaving the floor (the germinal matrix) completely intact.
4. Nail Plate Management: If the nail plate is severely dystrophic, it may be removed concurrently.
5. Healing: The resulting defect is not closed primarily. It is allowed to heal by secondary intention. This process effectively exteriorizes the chronic infection space, preventing further accumulation of debris and moisture.
Complications and Management
Surgical intervention for paronychia, while generally straightforward, carries the risk of several complications, primarily related to iatrogenic injury or inadequate source control.
| Complication | Estimated Incidence | Etiology | Salvage Strategy and Management |
|---|---|---|---|
| Nail Dystrophy / Split Nail | 5% - 10% | Iatrogenic sharp injury to the germinal matrix during incision; severe preoperative matrix necrosis | Scar excision of the germinal matrix and primary repair; split-thickness sterile matrix grafting for large defects |
| Recurrent Infection | 10% - 15% | Inadequate initial drainage; premature closure of the incision site; retained foreign body | Repeat incision and drainage; wider exposure; prolonged packing; targeted systemic antimicrobial therapy based on culture data |
| Felon Extension | < 5% | Volar tracking of the abscess through the lateral interosseous septa into the digital pulp | Emergent longitudinal volar or mid-lateral incision and drainage of the pulp space; division of fibrous septa |
| Osteomyelitis of Distal Phalanx | Rare (< 2%) | Neglected chronic infection; direct extension into the periosteum | Surgical debridement of necrotic bone; prolonged course of culture-directed intravenous or oral antibiotics |
| Septic Arthritis of DIP Joint | Rare (< 1%) | Proximal extension of a neglected paronychia into the joint capsule | Emergent arthrotomy, joint lavage, and possible temporary joint spanning external fixation if highly unstable |
| Digital Neuroma | < 1% | Iatrogenic transection of the dorsal branch of the proper digital nerve during lateral incision | Conservative management with desensitization; surgical exploration and neuroma excision with burying of the nerve stump into bone or muscle if refractory |
Management of Specific Complications
Nail Deformity: The most common functional and aesthetic complication is a longitudinal split or ridging of the nail plate. This occurs when a scar forms within the germinal matrix, preventing the uniform production of keratin. Management requires a delayed surgical approach (minimum 6 months post-infection) to elevate the nail plate, excise the longitudinal scar in the matrix, and repair the matrix with fine absorbable sutures (e.g., 7-0 chromic gut) under loupe magnification.
Progression to Felon: If a paronychia is inadequately drained, the pressure can force purulence volarly into the pulp space. Clinical examination will reveal a tense, exquisitely tender volar pulp. This requires immediate surgical decompression via a mid-lateral or volar longitudinal approach, ensuring the fibrous septa are adequately divided to decompress the entire pulp space.
Post Operative Rehabilitation Protocols
The immediate postoperative goal is to maintain continuous drainage and prevent premature sealing of the wound edges.
Immediate Postoperative Care (Days 0-3)
- Dressings: The initial bulky dressing and packing should remain in place for 24 to 48 hours.
- Elevation: Strict elevation of the affected hand above the level of the heart is mandatory to minimize edema, reduce throbbing pain, and facilitate venous and lymphatic drainage.
- Antibiotics: While simple I&D of a localized paronychia often does not require systemic antibiotics, patients with surrounding cellulitis, systemic symptoms, or immunocompromise should be prescribed a short course (5-7 days) of oral antibiotics. Empiric therapy should cover MRSA and MSSA (e.g., Trimethoprim-Sulfamethoxazole, Clindamycin, or Doxycycline) pending culture results.
Subacute Care and Rehabilitation (Days 3-14)
- Warm Soaks: Once the initial packing is removed, the patient must initiate warm water or dilute chlorhexidine/povidone-iodine soaks. These should be performed for 15 minutes, 3 to 4 times daily. Soaking promotes local vasodilation, facilitates the mechanical debridement of exudate, and prevents the incision edges from sealing.
- Wound Healing: Following each soak, a light, non-adherent dressing (e.g., a simple adhesive bandage) is applied. The wound is allowed to heal by secondary intention.
- Range of Motion: Active and active-assisted range of motion exercises of the DIP, PIP, and MCP joints should commence immediately to prevent joint stiffness and tendon adhesions. The patient should be instructed to achieve full composite flexion and extension multiple times a day.
Long-Term Follow-up
Patients are typically reviewed in the clinic at 1 week to ensure resolution of the infection and at 4 to 6 weeks to assess nail growth. Patients must be educated that a fully avulsed nail plate takes approximately 4 to 6 months to regenerate completely, and the new nail may exhibit temporary transverse ridging (Beau's lines) reflecting the systemic stress of the acute infection.
Summary of Key Literature and Guidelines
The surgical management of paronychia is heavily guided by established anatomical principles and evolving microbiological data.
- Microbiology and Antibiotic Stewardship: Recent guidelines from the Infectious Diseases Society of America (IDSA) emphasize the high prevalence of community-acquired MRSA in skin and soft tissue infections, including hand infections. Empiric antibiotic therapy, when indicated, must include MRSA coverage until culture sensitivities dictate otherwise. However, multiple prospective studies have demonstrated that for simple, localized paronychia without extensive cellulitis, surgical incision and drainage alone, without the addition of systemic antibiotics, yields equivalent cure rates and reduces the risk of antibiotic resistance.
- Surgical Technique Efficacy: The classic literature by Keyser and Eaton established the standard techniques for paronychia drainage, emphasizing the avoidance of the germinal matrix. The efficacy of the marsupialization technique for chronic paronychia was popularized by Bednar and Lane, demonstrating high success rates and low recurrence when the fibrotic eponychial roof is adequately excised.
- Anesthesia Safety: Historically, the use of epinephrine in digital blocks was taught as an absolute contraindication due to the fear of digital necrosis. However, extensive comprehensive reviews and large cohort studies (e.g., Lalonde et al.) have definitively proven the safety of lidocaine with epinephrine in the digits of healthy patients, demonstrating improved hemostasis and prolonged anesthesia without increased risk of ischemic complications. This paradigm shift allows for better visualization during the meticulous dissection required around the nail matrix.
- Timing of Intervention: Literature consistently supports early surgical decompression once fluctuance is identified. Delayed intervention directly correlates with a logarithmic increase in the risk of deep space spread, felon formation, and osteomyelitis, reinforcing the surgical maxim that a localized abscess in the hand demands prompt evacuation.
