Postoperative Care and Web Space Reconstruction in Hand Surgery
Key Takeaway
Optimal postoperative care in hand surgery is paramount for restoring function and mitigating edema. This comprehensive guide details evidence-based protocols for dressing application, limb elevation, and rehabilitation. Furthermore, it provides step-by-step surgical techniques for addressing web space contractures using four-flap Z-plasties and dorsal flaps, ensuring orthopaedic surgeons and residents achieve superior clinical outcomes.
Comprehensive Introduction and Patho-Epidemiology
The ultimate success of any surgical intervention within the intricate anatomical confines of the hand is inextricably linked to the quality, precision, and rigor of the postoperative care regimen. In orthopedic and plastic hand surgery, the operation itself represents merely the initial phase of a continuum of care. The postoperative phase must be meticulously managed to ensure that traumatized tissues are allowed to heal optimally while the highly complex, interconnected biomechanical functions of the affected extremity are restored as rapidly as physiologically possible. This phase begins the moment the final suture is placed in the operating room, heavily relying on the immediate application of a biomechanically sound surgical dressing, and extends through months of structured, highly specialized rehabilitation. Failure to appreciate the criticality of this phase frequently results in catastrophic functional outcomes, rendering even the most technically brilliant surgical reconstruction functionally useless.
The pathophysiology of postoperative hand dysfunction is primarily driven by the body's natural inflammatory response, which, if left unchecked, initiates a devastating cascade of edema, fibroblastic proliferation, and subsequent joint contracture. Due to the dependent positioning of the upper extremity and the naturally high ratio of synovial and tendinous structures to subcutaneous fat, the hand is uniquely susceptible to the rapid accumulation of protein-rich lymphatic exudate. When this exudate stagnates, it acts as a biological glue. Fibroblasts migrate into this proteinaceous matrix, laying down disorganized collagen cross-links that adhere gliding planes—such as flexor tendons within their sheaths, or the delicate extensor mechanism over the phalanges—to the surrounding static structures. This pathophysiological process underscores the absolute necessity of aggressive edema management and early, controlled mobilization to maintain the gliding capacity of these tissues.
Within the spectrum of hand surgery, the management of web space contractures represents a particularly challenging intersection of precise surgical reconstruction and demanding postoperative care. The epidemiology of web space contractures is diverse, encompassing sequelae from thermal and chemical burns, severe crush injuries, chronic infections, neglected compartment syndromes, and congenital anomalies such as syndactyly. Iatrogenic causes, often resulting from poorly planned incisions that cross the web space perpendicularly rather than utilizing Brunner-type zig-zag or mid-axial approaches, also constitute a significant portion of these deformities. Regardless of the etiology, the functional impairment is profound.
The first web space is arguably the most critical functional unit of the hand, dictating the spatial positioning of the thumb required for opposition, key pinch, and power grasp. A contracture here severely debilitates overall hand function, effectively reducing the functional capacity of the hand by up to 50%. Similarly, linear contractures of the lesser web spaces (second, third, and fourth) restrict the independent, divergent spread of the fingers and frequently induce rotational deformities during digital flexion. Addressing these contractures requires not only precise local flap reconstruction to restore the three-dimensional geometry of the commissure but also an unrelenting postoperative protocol to prevent the recurrence of the fibrotic cascade.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy and biomechanics of the hand is the foundation upon which all postoperative care and reconstructive procedures are built. The biomechanics of the surgical dressing, often dismissed as a mundane task, is in fact the first critical step in postoperative rehabilitation. A poorly applied dressing can lead to ischemia, maceration, irreversible joint stiffness, and complex regional pain syndrome (CRPS). The routine dressing must be applied systematically, respecting the underlying anatomy. The primary contact layer utilizes a closely woven, nonadherent gauze, such as Xeroform (bismuth tribromophenate) or Adaptic (cellulose acetate). Granulation tissue cannot penetrate this tightly woven architecture, thereby preventing traumatic adherence during subsequent dressing changes while allowing serosanguinous exudate to pass through to the secondary layers, mitigating maceration of the fragile epidermis.
The secondary, conformational layer is where the biomechanical positioning of the hand is established. The hand must be immobilized in the "intrinsic plus" or "safe" position. This involves positioning the metacarpophalangeal (MCP) joints in 70° to 90° of flexion, the interphalangeal (IP) joints in full extension, and the wrist in 20° to 30° of extension. The anatomical rationale for this position is paramount: the collateral ligaments of the MCP joints are eccentrically attached dorsal to the axis of rotation. Therefore, they are maximally taut in flexion and lax in extension. Conversely, the volar plates of the IP joints are taut in extension. Immobilizing the hand in the intrinsic plus position maintains these critical ligamentous structures at their maximal length, preventing the devastating "claw hand" deformity that occurs when these ligaments contract during the healing phase. Moist sponges (soaked in sterile saline or glycerin) are biomechanically superior to dry sponges in this layer; they conform to the complex topographical contours of the hand, distribute compressive pressure evenly, and actively promote the capillary absorption of blood and exudate, minimizing hematoma formation.
The surgical anatomy of the web spaces is highly specialized, designed to provide maximum mobility while maintaining structural integrity. The first web space is a complex, multi-layered anatomical region. The skin of the first web is highly distensible dorsally but heavily tethered volarly. Deep to the subcutaneous tissue lies the investing fascia of the intrinsic musculature, specifically the adductor pollicis and the first dorsal interosseous muscles. The princeps pollicis artery, a terminal branch of the radial artery, courses deep within this space, while the superficial radial nerve provides critical sensory innervation to the dorsal aspect. In a first web space contracture, the pathology is rarely confined to the skin; the investing fascia of these muscles frequently undergoes severe fibrotic shortening, requiring meticulous surgical release prior to any skin flap transposition.
The lesser web spaces (second, third, and fourth) are defined by a different set of anatomical constraints. The distal boundary of these spaces is formed by the natatory ligaments (superficial transverse metacarpal ligaments), which run transversely across the volar aspect of the web spaces, resisting excessive digital abduction. Deep to these lie the true transverse metacarpal ligaments, which connect the volar plates of the adjacent MCP joints. The neurovascular bundles course vertically through the lumbrical canals, intimately associated with the fascial septa of the web space. When a linear contracture develops in a lesser web space, the natatory ligaments are frequently incorporated into the fibrotic scar band. Reconstructive efforts, such as dorsal rectangular flaps, must carefully navigate this anatomy, releasing the fibrotic natatory ligaments while meticulously preserving the digital nerves and arteries that lie immediately deep to the contracture band.
Exhaustive Indications and Contraindications
The decision to proceed with web space reconstruction, as well as the selection of specific postoperative modalities, must be guided by a rigorous evaluation of indications and contraindications. Surgical intervention is generally indicated when a contracture significantly impedes activities of daily living (ADLs), limits occupational function, or causes persistent pain due to tethering. For the first web space, an inability to achieve at least 40 to 45 degrees of palmar abduction or an inability to span large objects (e.g., a large cylinder or jar) constitutes a strong indication for release. In the lesser web spaces, indications include an inability to independently abduct the digits, rotational malalignment during flexion caused by asymmetric tethering, or hygiene issues related to severe syndactyly.
The choice of reconstructive technique is dictated by the quality and availability of the surrounding tissue. A linear scar contracture bordered by healthy, pliable, and elastic skin is the classic indication for a local tissue rearrangement, such as a four-flap Z-plasty or a dorsal rectangular flap. These techniques provide vascularized tissue coverage and break the linear line of tension without the need for distant donor sites. However, if the contracture is the result of a broad, diffuse burn scar where the surrounding tissue is equally compromised and inelastic, local flaps are contraindicated. In such scenarios, the surgeon must resort to radical excision of the scar tissue followed by the application of full-thickness skin grafts (FTSG) or, in severe cases involving exposed deep structures, regional or free vascularized tissue transfer (e.g., a lateral arm flap or anterolateral thigh flap).
Absolute contraindications to elective web space reconstruction include active, untreated local or systemic infection, severe peripheral vascular disease that compromises the viability of local flaps, and profound patient noncompliance. A patient who is unable or unwilling to participate in the grueling postoperative rehabilitation protocol, which includes rigorous splinting and painful therapy sessions, will inevitably experience a recurrence of the contracture, rendering the surgical intervention futile. Relative contraindications include heavy tobacco use, which significantly increases the risk of marginal flap necrosis, and severe, unmanaged psychiatric conditions that preclude adherence to postoperative instructions.
| Modality / Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Four-Flap Z-Plasty (1st Web) | Severe linear scar contracture; healthy adjacent skin; loss of thumb palmar abduction >30°. | Diffuse burn scarring of the entire web; active local infection; inadequate vascularity. | Heavy smoking; severe diabetes mellitus; moderate noncompliance. |
| Dorsal Rectangular Flap | Linear contracture of 2nd, 3rd, or 4th web spaces; mild/moderate syndactyly. | Lack of pliable dorsal skin; extensive dorsal hand trauma/burns. | Prior incisions compromising the dorsal flap pedicle. |
| Full-Thickness Skin Graft | Broad, diffuse web space contractures where local flaps are impossible; deep burn sequelae. | Exposed bare tendon, bone, or joint capsule (requires vascularized flap). | Poor donor site availability; high risk of graft shear. |
| Early Active Motion (AROM) | Most uncomplicated tendon repairs; stable fracture fixation; post-contracture release. | Unstable fractures; tenuous vascular repairs; specific complex nerve repairs. | Patient inability to comprehend motion limits. |
| Forced Passive Motion | NONE. (Historically used, now universally recognized as harmful). | All postoperative hand surgery patients. | N/A |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the hallmark of successful hand surgery and is critical for both the execution of web space flaps and the anticipation of postoperative needs. This planning begins with tourniquet management. The pneumatic tourniquet is indispensable for providing a bloodless surgical field, allowing for the precise identification of delicate neurovascular structures. Exsanguination is achieved using an Esmarch bandage or sterile Rhys-Davies exsanguinator before inflating the tourniquet to approximately 100 mmHg above the patient's systolic blood pressure (typically 200-250 mmHg for adults). However, tourniquet time must be strictly monitored, ideally not exceeding 120 minutes to prevent ischemic neuropraxia and severe muscle damage. Immediately before the tourniquet is deflated, the hand must be kept constantly elevated. This critical step prevents the sudden, forceful engorgement of the vascular tree, thereby mitigating immediate postoperative edema and reactive hemorrhage into the newly elevated flap spaces.
Preoperative templating of the flaps is an exacting geometric exercise. For the first web space, the standard 60-degree Z-plasty provides a theoretical 73% increase in length along the axis of the central limb. However, for severe contractures, this is often insufficient. The four-flap Z-plasty (often utilizing a combination of 90-degree and 120-degree angles) provides a significantly broader and deeper release. The surgeon must draw the central limb directly over the crest of the linear scar contracture. The four distinct flaps are then outlined, meticulously calculating the angles to ensure the base-to-length ratio supports adequate perfusion to the tips of the flaps. Broad-based flaps are absolutely essential; narrow, acutely angled flaps are highly prone to distal necrosis, which would expose the newly released web space and lead to a recurrence worse than the original deformity.
Patient positioning and anesthesia are tailored to facilitate both intraoperative precision and postoperative comfort. The patient is typically positioned supine with the operative extremity extended on a radiolucent hand table. Regional anesthesia, such as an axillary or supraclavicular brachial plexus block, is highly preferred over general anesthesia. Regional blocks not only provide excellent intraoperative anesthesia but also induce a profound sympathectomy. This sympathetic blockade results in significant vasodilation, maximizing arterial inflow to the newly transposed flaps during the critical early postoperative hours. Furthermore, the extended pain control allows the patient to tolerate the immediate postoperative elevation and initial dressing application without the systemic side effects of high-dose intravenous opioids.
Pediatric considerations in preoperative planning and postoperative care present unique and demanding challenges. The pediatric forearm is distinctly conical, tapering rapidly from the elbow to the wrist. Splints and bandages applied to children have a notoriously high propensity to slip distally, rendering the immobilization ineffective and potentially causing pressure sores. Furthermore, children exhibit inherent noncompliance with immobilization protocols. To effectively control this, surgeons must plan to apply a long-arm splint or cast, extending well above the elbow, combined with a tube of stockinette that encloses the entire extremity, often incorporating the thumb or adjacent digits for added stability. Adults and caregivers responsible for the child’s postoperative care must be thoroughly educated preoperatively and proven competent in evaluating the vascular status of the fingers (capillary refill, color, temperature, and turgor).
Step-by-Step Surgical Approach and Fixation Technique
First Web Space Contracture Reconstruction
The reconstruction of a severe first web space contracture using a four-flap Z-plasty is a highly effective procedure when executed with geometric precision and meticulous tissue handling.
- Preoperative Marking and Geometry: Under tourniquet control, the central limb of the Z-plasty is drawn directly over the most prominent crest of the linear scar contracture. The four flaps are then designed. To achieve maximum deepening, two broad-angled flaps (often 90 degrees) and two narrower flaps (often 45 to 60 degrees) are designed to interdigitate. The precise angles are dictated by the pliability of the local skin.
- Incision and Flap Elevation: Sharp incisions are made down through the dermis into the subcutaneous fat. The flaps are elevated using delicate skin hooks rather than crushing forceps. Dissection must remain superficial to the deep fascia to preserve the delicate subdermal vascular plexus that provides the sole blood supply to these random-pattern flaps.
- Deep Contracture Release: Elevation of the skin flaps alone is rarely sufficient. The underlying fascial bands, particularly the thickened investing fascia over the adductor pollicis and the first dorsal interosseous muscles, must be systematically released or excised. The surgeon must palpate the web space while passively abducting the thumb to identify and divide all restricting tethering bands, taking extreme care to protect the radial artery branches and sensory nerves.
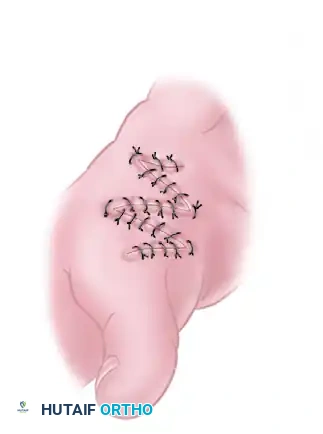
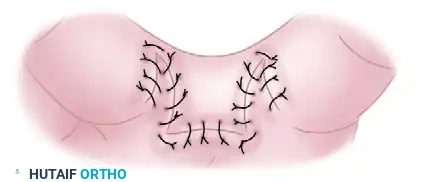
- Flap Transposition and Closure: Once full, unhindered passive abduction of the thumb is achieved, the four flaps are rotated and transposed into their new, interdigitated positions. The geometry of the four-flap system allows the tight linear scar to be broken up, dramatically deepening the web space. The flaps are sutured in place using fine, non-absorbable monofilament sutures (e.g., 5-0 or 6-0 nylon). The sutures must be placed with minimal tension; if excessive tension is noted, the flaps must be revised, or supplemental skin grafting may be required.
Second, Third, and Fourth Web Space Reconstruction
For linear contractures of the lesser web spaces, the dorsal rectangular flap technique provides a highly reliable method for restoring the normal slope and depth of the commissure.

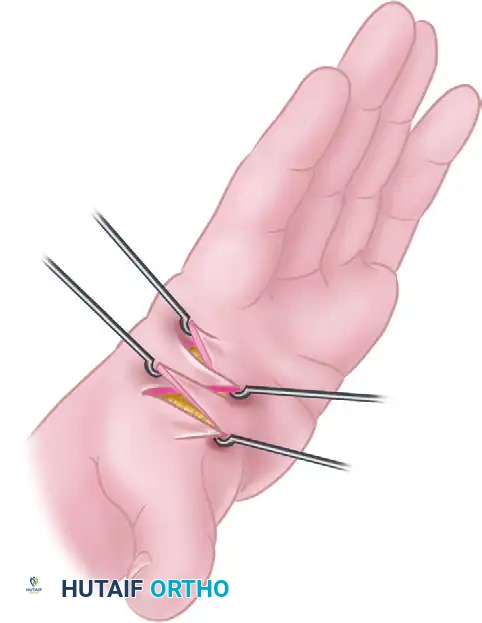
- Assessment and Flap Design: The web space is evaluated under tension by passively abducting the adjacent digits to identify the exact vector of the linear scar. A proximally based dorsal rectangular or trapezoidal flap is outlined over the dorsal aspect of the web space. Volar triangular flaps are simultaneously designed to interdigitate with the distal end of the dorsal flap once it is advanced.

- Elevation of the Dorsal Flap: The dorsal flap is elevated carefully from distal to proximal. The dissection plane is critical; it must remain superficial to the extensor paratenon to ensure the extensor tendons continue to glide smoothly. The dorsal sensory branches of the ulnar or radial nerves must be identified and protected during this elevation.
- Release of the Natatory Ligaments: The fibrotic bands causing the volar web contracture are sharply excised. The natatory ligaments, which are frequently hypertrophied and involved in the fibrotic process, require partial resection to allow the digits to diverge normally. The neurovascular bundles are visualized and protected during this deep release.
- Rotation, Interdigitation, and Suturing: The dorsal flap is advanced volarly and rotated into the depth of the newly created web space. The volar triangular flaps are interdigitated with the distal edge of the dorsal flap. This strategic interdigitation breaks the linear line of tension exactly at the deepest point of the commissure, providing healthy, pliable skin where the mechanical stress is highest, thereby preventing recurrence. The flaps are secured with 5-0 chromic gut or nylon sutures.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications in hand surgery and web space reconstruction can and do occur. The margin for error is exceptionally narrow, and the consequences of complications are often functionally devastating. The most feared immediate postoperative complication following flap reconstruction is vascular compromise leading to flap necrosis. This can manifest as either venous congestion (the flap appears blue, engorged, with brisk but dark capillary refill) or arterial insufficiency (the flap is pale, cool, with absent capillary refill). Venous congestion is more common and is frequently caused by excessive tension on the suture line, a hematoma compressing the pedicle, or an overly constrictive dressing.
If vascular compromise is detected, immediate intervention is mandatory. The first step is to completely loosen the surgical dressing and remove any constricting bandages. If the flap remains compromised, a few sutures at the point of maximal tension must be released. If a hematoma is present, it must be evacuated immediately. In cases of severe, refractory venous congestion where the pedicle is intact but venous outflow is inadequate, the application of medicinal leeches (Hirudo medicinalis) can be a highly effective salvage strategy. The leeches actively remove congested blood, and their saliva contains hirudin, a potent anticoagulant that promotes continued bleeding from the bite site, temporarily acting as an artificial venous outflow tract until angiogenesis establishes new venous channels.
Infection is another severe complication that can rapidly destroy gliding planes and lead to catastrophic stiffness. While routine, complete redressing of wounds is generally unnecessary and disrupts the healing milieu, the dressing must be opened under sterile conditions if an infection is clinically suspected (e.g., escalating throbbing pain, systemic fever, malodor, or excessive purulent drainage). If a deep space infection is confirmed, the patient must be returned to the operating room for formal irrigation and debridement, followed by culture-directed intravenous antibiotic therapy.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management Protocol |
|---|---|---|---|
| Flap Necrosis (Venous/Arterial) | 3% - 8% | Broad-based flap design; meticulous hemostasis; tension-free closure; avoid tight dressings. | Release sutures; evacuate hematoma; medicinal leeches (for venous congestion); hyperbaric oxygen therapy (HBOT); eventual skin grafting if necrosis demarcates. |
| Postoperative Hematoma | 2% - 5% | Strict tourniquet deflation before closure; precise electrocautery; immediate postoperative elevation; moist compressive dressings. | Immediate sterile evacuation; re-cauterization of bleeding vessels; reapplication of compressive dressing. |
| Deep Space Infection | 1% - 3% | Strict sterile technique; prophylactic antibiotics; avoidance of hematoma (which acts as culture medium). | Operative irrigation and debridement (I&D); open wound management or delayed primary closure; targeted IV antibiotics. |
| Severe Joint Stiffness | 10% - 15% | Immobilization in "intrinsic plus" position; early active range of motion (AROM); aggressive edema control. | Intensive hand therapy; dynamic/static progressive splinting; late surgical tenolysis or capsulotomy (last resort). |
| Recurrence of Contracture | 5% - 12% | Adequate deep fascial release; breaking linear tension lines (Z-plasty); strict adherence to postoperative splinting. | Revision surgery with more complex flap design (e.g., regional flap) or full-thickness skin grafting. |
Phased Post-Operative Rehabilitation Protocols
The rehabilitation phase following hand surgery, particularly after complex web space reconstructions, is a highly structured, phased process that demands a well-integrated team approach involving the surgeon, a certified hand therapist (CHT), and a compliant patient. The surgeon must take the lead in prescribing and monitoring the therapy program, tailoring it to the specific biomechanical stability of the surgical repair.
Phase I: Immediate Postoperative Phase (Days 0 to 14)
The primary goals during this phase are the absolute control of edema, the protection of the surgical repair, and the prevention of stiffness in uninvolved joints. Elevation must be maintained rigorously for at least 48 to 72 hours postoperatively. Effective elevation requires the hand to be positioned strictly above the level of the heart. This can be achieved using specialized foam elevation blocks, overhead suspension systems, or properly arranged pillows. Merely supporting the hand in a standard sling while the patient is ambulatory is highly ineffective and often exacerbates dependent edema.
During this phase, fingers that are not explicitly splinted for surgical reasons must be exercised immediately. Active range of motion (AROM) of the uninvolved digits acts as a physiological musculovenous pump, actively clearing protein-rich lymphatic fluid. Furthermore, the shoulder is highly susceptible to becoming stiff, especially in older patients. Patients must be explicitly instructed to abduct and elevate the shoulder toward the head several times daily to prevent the insidious onset of adhesive capsulitis. The surgical dressing remains intact unless complications are suspected.
Phase II: Intermediate Healing Phase (Weeks 2 to 4)
At approximately 10 to 14 days, the initial bulky dressing is removed, and the wounds are inspected. Suture removal in hand surgery often dictates a modified timeline compared to other anatomical regions. Because the hand is subjected to high dynamic forces, sutures may be left in place for up to 3 weeks, particularly in areas of high tension like a transposed Z-plasty web space.
Once the flaps are deemed viable and the incisions are healing, the rigid postoperative splint is often transitioned to a custom-molded thermoplastic splint. For web space reconstructions, this splint is designed to maintain the web spaces in maximal abduction (within the limits of skin tension) to prevent the maturing scar tissue from contracting. Aggressive active range of motion of the involved digits is initiated. Scar massage techniques, utilizing emollients, are begun to soften the maturing collagen and prevent adherence to underlying fascial planes.
Phase III: Remodeling and Functional Return (Weeks 4 and Beyond)
As the scar tissue enters the remodeling phase, therapy intensifies. If residual stiffness or contracture is noted, static progressive or dynamic splinting is introduced to provide a low-load, prolonged stretch to the tissues. For web space reconstructions, the use of custom silicone elastomer web spacers is highly effective. These spacers are worn inside the splint or during the day to maintain the surgical correction, apply gentle pressure to the scar, and soften the tissue.
Surgical Warning: Throughout all phases of rehabilitation, applying excessive heat to the hand and forcing passive manipulation of joints by the patient, therapist, or surgeon are strictly contraindicated. Forced passive motion induces microtrauma to the delicate healing tissues, exacerbates the inflammatory cascade, and ultimately leads to increased fibrosis, heterotopic ossification, and intractable stiffness.
The ultimate goal of therapy is the return to functional activities of daily living (ADLs). Often, the best therapy is the patient’s usual work; if possible, patients should be offered the opportunity to return to work on a limited or modified-duty basis. This functional rehabilitation yields significant beneficial psychological effects and promotes the integration of the reconstructed hand into normal motor patterns.
Summary of Landmark Literature and Clinical Guidelines
The principles of postoperative care and web space reconstruction detailed in this chapter are deeply rooted in decades of landmark orthopedic and plastic surgery literature. The paradigm shift from prolonged immobilization to early active motion in hand surgery was pioneered by the seminal works of Kleinert and Duran in the context of flexor tendon repairs. Their research fundamentally altered the understanding of tendon healing, demonstrating that controlled biomechanical stress promotes intrinsic tendon healing and prevents restrictive
