Masterclass: Surgical Drainage of Deep Space Hand Infections

Key Takeaway
This masterclass guides fellows through the urgent surgical drainage of deep space hand infections. We cover essential anatomy, meticulous preoperative planning, and granular intraoperative execution for thenar, midpalmar, hypothenar, and Parona's spaces. Emphasizing neurovascular protection, thorough débridement, and critical post-operative management, this session ensures optimal patient outcomes and complication avoidance.
Comprehensive Introduction and Patho-Epidemiology
Deep space infections of the hand represent a formidable clinical challenge and a true orthopedic emergency. These are not superficial cellulitides that can be managed with a trial of oral antibiotics and outpatient observation; these are aggressive, rapidly progressive limb-threatening, and potentially life-threatening conditions. The unique, closed fascial architecture of the hand creates an environment where purulent exudate under pressure can rapidly lead to ischemic necrosis of vital neurovascular and tendinous structures. A delay in definitive surgical extirpation and decompression invariably leads to devastating consequences, including profound functional loss, contiguous osteomyelitis, systemic sepsis, and in severe cases, the necessity for digital or hand amputation. There is absolutely no role for nonoperative management once a deep space abscess has formed; prompt, aggressive, and precise surgical intervention is the gold standard of care.
The pathophysiology of these infections typically involves direct inoculation of bacteria into the deep fascial spaces via penetrating trauma, such as a puncture wound, animal bite, or human bite. Alternatively, they may arise from the contiguous spread of adjacent infections, most notably suppurative flexor tenosynovitis that ruptures through the proximal cul-de-sac of the flexor tendon sheath into the midpalmar or thenar spaces. Hematogenous seeding is exceptionally rare but can occur in severely immunocompromised patients. The enclosed nature of these spaces means that even a small volume of purulence significantly elevates interstitial pressure, compromising capillary perfusion and leading to a vicious cycle of tissue ischemia, necrosis, and further bacterial proliferation. The dense palmar aponeurosis forces the expanding purulence to track along the paths of least resistance, often spreading proximally into the forearm or dorsally into the web spaces.
Epidemiologically, the bacteriology of deep space hand infections has evolved significantly over the past two decades. While Staphylococcus aureus remains the most frequently isolated organism, the prevalence of Methicillin-resistant Staphylococcus aureus (MRSA) has surged, necessitating a shift in empiric antibiotic regimens. Streptococcus species are also common, particularly in cases presenting with rapid proximal lymphatic spread. In cases of animal bites, Pasteurella multocida must be suspected, whereas human bites (clenched-fist injuries) classically involve a polymicrobial flora including Eikenella corrodens, Streptococcus viridans, and various anaerobes. Furthermore, patients with underlying systemic comorbidities—particularly poorly controlled diabetes mellitus, chronic renal failure, intravenous drug use, or iatrogenic immunosuppression—are at a markedly increased risk for atypical, polymicrobial, and rapidly fulminant infections.
Recognizing the systemic implications of these localized infections is critical for the treating surgeon. A localized midpalmar abscess can rapidly evolve into systemic inflammatory response syndrome (SIRS) or frank sepsis. Therefore, the surgeon must not only focus on the mechanical drainage of the hand but also work in concert with infectious disease specialists and medical intensivists to manage the patient's systemic physiologic derangements. The overarching goal is a rapid, multidisciplinary approach: immediate broad-spectrum intravenous antibiotics following culture acquisition, emergent surgical decompression and radical débridement, followed by tailored antimicrobial therapy and aggressive postoperative rehabilitation.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel is ever brought to the skin, the operating surgeon must possess an intimate, three-dimensional understanding of the intricate anatomy of the hand's deep fascial spaces. These spaces, originally elegantly described by Kanavel, are not empty voids but rather potential spaces filled with loose areolar tissue, bounded by rigid fascial septa. They serve as the anatomical highways for infection to spread rapidly, driven by the hand's complex architecture. The hand contains three primary deep potential spaces: the thenar, midpalmar, and hypothenar spaces. Additionally, Parona’s space in the distal forearm must be thoroughly understood, as it is intimately connected to the hand spaces and serves as a conduit for proximal extension.
The Thenar Space
The thenar space is uniquely positioned and represents the most frequently involved deep space in clinical practice. Its borders are strictly defined: dorsally by the robust fascia of the adductor pollicis muscle; volarly by the flexor tendon sheath of the index finger and the radial aspect of the palmar fascia; and radially by the insertion of the adductor pollicis tendon and fascia onto the proximal phalanx of the thumb. The ulnar border is formed by the midpalmar septum, which separates it from the midpalmar space. Infections here can spread rapidly due to the dynamic motion of the thumb and index finger, which acts as a mechanical pump, disseminating purulence through the loose areolar tissue.
Navigating the thenar space surgically requires meticulous attention to critical neurovascular structures. The volar approach places the surgeon in direct proximity to the recurrent motor branch of the median nerve—the "million-dollar nerve"—which is absolutely vital for thenar muscle function and thumb opposition. Additionally, the digital nerves to the thumb and radial aspect of the index finger, the princeps pollicis artery, and the proper digital arteries must be identified and protected. If a thenar space infection is left untreated, the purulence will inevitably destroy the fascia of the adductor pollicis, tracking between its transverse and oblique heads to spread to the dorsal aspect of the hand, presenting as a massive, fluctuant swelling in the first dorsal web space.
The Midpalmar Space
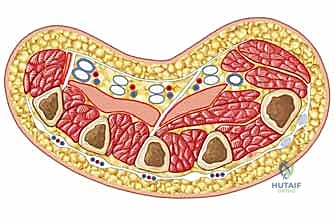
The midpalmar space lies deep within the central concavity of the hand. It is bounded radially by the midpalmar septum (extending from the third metacarpal to the palmar fascia) and ulnarly by the hypothenar septum (extending from the fifth metacarpal to the palmar fascia). Dorsally, it rests upon the fascia of the second and third palmar interosseous muscles and the third, fourth, and fifth metacarpals. Volarly, it is roofed by the flexor tendon sheaths of the long, ring, and small fingers, and the dense, unyielding palmar aponeurosis. While less common than thenar infections, midpalmar abscesses are exceptionally dangerous due to their immediate proximity to the flexor tendons and the superficial palmar arch.
Surgical exploration of the midpalmar space demands profound respect for the superficial palmar arch and the common and proper digital nerves and arteries supplying the central digits. The unyielding nature of the palmar aponeurosis means that palmar swelling is often deceptively minimal; instead, the interstitial pressure forces fluid dorsally via the lumbrical canals, resulting in massive dorsal hand edema. This anatomical quirk frequently misleads inexperienced clinicians into making inappropriate dorsal incisions for what is fundamentally a volar deep space infection.

The Hypothenar and Parona’s Spaces
The hypothenar space is a relatively isolated compartment, making infections here less common and typically the result of direct penetrating trauma to the ulnar border of the hand. It is bounded radially by the hypothenar septum, dorsally by the periosteum of the fifth metacarpal, and volarly/ulnarly by the investing fascia of the hypothenar musculature (abductor digiti minimi, flexor digiti minimi brevis, opponens digiti minimi). The primary structures at risk during drainage are the ulnar nerve, specifically its deep motor branch, and the ulnar artery, which dive deep into the palm at the proximal border of this space.
Parona’s space is a deep, quadrilateral potential space located in the distal volar forearm, situated just proximal to the wrist crease. It lies superficial to the pronator quadratus muscle and interosseous membrane, and deep to the flexor digitorum profundus (FDP) tendons and their enveloping synovial sheaths. Critically, Parona’s space is continuous with the midpalmar space distally. Infection here usually results from contiguous proximal spread from a ruptured radial or ulnar bursa (complicating suppurative flexor tenosynovitis). When an infection involves both the radial and ulnar bursae and communicates via Parona’s space, it forms the classic and highly destructive "horseshoe abscess," requiring extensive volar forearm and palmar decompression.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention in the setting of a suspected deep space hand infection is rarely equivocal. The presence of purulence within these closed fascial compartments dictates immediate surgical decompression. However, distinguishing between early, superficial cellulitis (which may occasionally respond to aggressive intravenous antibiotics and elevation) and a true deep space abscess requires astute clinical judgment, a high index of suspicion, and a thorough understanding of the indications and contraindications for surgery.
Absolute indications for surgical drainage include any clinical or radiographic evidence of a localized abscess within the thenar, midpalmar, hypothenar, or Parona's spaces. Furthermore, the presence of systemic inflammatory response syndrome (SIRS) or frank sepsis in conjunction with a hand infection mandates emergent operative source control. Failure of a suspected cellulitis to improve after 12 to 24 hours of appropriate, culture-directed intravenous antibiotic therapy and strict elevation also constitutes a strong indication for surgical exploration, as this often heralds an underlying, undrained deep collection. Additionally, any infection complicated by signs of compartment syndrome of the hand or impending skin necrosis requires immediate fasciotomy and débridement.
Contraindications to the surgical drainage of deep space hand infections are entirely relative, as this is fundamentally a limb-saving and potentially life-saving procedure. In patients with profound hemodynamic instability or severe, uncorrectable coagulopathy, the timing of surgery must be carefully coordinated with critical care and anesthesia teams to optimize the patient prior to induction. However, source control cannot be indefinitely delayed. In extreme cases where general anesthesia is absolutely contraindicated, the procedure may be performed under regional anesthesia (e.g., axillary or supraclavicular block) or, in dire circumstances, wide-awake local anesthesia with no tourniquet (WALANT), though the latter is less ideal for extensive, deep débridement requiring wide exposure.
| Category | Specific Clinical Scenarios | Management Strategy |
|---|---|---|
| Absolute Indications | Fluctuant mass in thenar, midpalmar, or hypothenar eminence | Emergent operative I&D, copious irrigation, broad-spectrum IV antibiotics. |
| MRI or Ultrasound confirmed deep space fluid collection | Emergent operative I&D, targeted débridement. | |
| Hand infection with systemic sepsis or SIRS criteria | Emergent surgical source control, ICU admission, infectious disease consult. | |
| Progressive symptoms despite 24h of appropriate IV antibiotics | Operative exploration to rule out occult deep space abscess or tenosynovitis. | |
| Relative Indications | Severe dorsal edema with suspected volar deep space involvement | Volar exploration based on Kanavel's signs and clinical suspicion; avoid isolated dorsal incisions. |
| Relative Contraindications | Severe, uncorrected coagulopathy (e.g., INR > 3.0, Plt < 50k) | Rapid reversal of coagulopathy with FFP/PCC/Platelets concurrently with surgical preparation. |
| Extreme hemodynamic instability | Resuscitation and vasopressor support; consider regional anesthesia or WALANT if general is prohibitive. |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning for a deep space hand infection is a dynamic process that begins the moment the patient enters the emergency department. It is not merely a logistical formality; it is the critical phase where the surgeon anticipates anatomical challenges, formulates a precise surgical strategy, and optimizes the patient for a safe and effective procedure. A meticulous history and physical examination are paramount. The surgeon must ascertain the mechanism of injury, paying particular attention to any history of penetrating trauma, animal or human bites, or foreign body exposure. The timeline of symptom progression and any prior antibiotic treatments must be documented.
The physical examination must be systematic and thorough. For suspected thenar space infections, the examiner will note profound swelling and exquisite tenderness localized to the thenar eminence. The patient will characteristically hold their thumb in an abducted and slightly flexed position to maximize the volume of the thenar space and minimize capsular tension. If the infection has tracked dorsally, significant swelling and tenderness will be evident in the first dorsal web space. In contrast, midpalmar space infections present with loss of the normal palmar concavity, exquisite tenderness over the central palm, and the fingers (particularly the middle and ring fingers) held in a semi-flexed posture. It is crucial to differentiate this from suppurative flexor tenosynovitis; in a pure midpalmar space infection, there is typically less pain with passive extension of the digits and an absence of exquisite tenderness along the entire length of the flexor tendon sheath.

Diagnostic imaging and laboratory studies form the cornerstone of the preoperative workup. Standard anteroposterior, lateral, and oblique radiographs of the hand and wrist are absolutely mandatory to rule out radiopaque foreign bodies, underlying fractures, or evidence of chronic osteomyelitis (e.g., periosteal reaction, cortical destruction) or subcutaneous gas indicative of a necrotizing infection. While ultrasound can be utilized at the bedside to identify localized fluid collections, and MRI provides unparalleled anatomical detail regarding the extent of soft tissue involvement, these modalities should never delay emergent surgical intervention in a clinically obvious case. Laboratory workup must include a complete blood count (CBC) with differential, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), comprehensive metabolic panel, and, crucially, aerobic and anaerobic blood cultures if the patient exhibits any systemic signs of infection.

Patient positioning and operating room setup must be standardized to ensure optimal surgical flow and safety. The patient is positioned supine on the operating table. A standard, radiolucent hand table is securely attached to the operative side, ensuring it is well-padded and positioned to allow the surgeon and assistant unencumbered access to the entire upper extremity. A nonsterile pneumatic tourniquet is applied over copious cast padding to the proximal upper arm. The limb is exsanguinated by elevation (avoiding Esmarch bandages to prevent proximal dissemination of septic emboli), and the tourniquet is inflated to 250 mmHg (or 100 mmHg above systolic blood pressure). General anesthesia or a robust regional block (axillary or supraclavicular) is preferred to provide profound muscle relaxation and patient comfort during extensive deep dissection. A wide sterile prep and drape, extending from the fingertips to the mid-humerus, is essential to allow for proximal extension of incisions if tracking purulence is discovered.
Step-by-Step Surgical Approach and Fixation Technique
The intraoperative execution of deep space infection drainage requires a meticulous, systematic approach. The overarching goals are absolute: obtain reliable microbiological cultures, achieve complete decompression and drainage of the purulent collection, perform a radical sharp débridement of all necrotic and devitalized tissue, and execute copious pulsatile or gravity irrigation to mechanically reduce the bacterial bioburden. Adherence to these principles is non-negotiable for a successful outcome.
The crucial first step, prior to the administration of any prophylactic or therapeutic intravenous antibiotics in the operating room, is the acquisition of pristine microbiological specimens. Deep tissue swabs, or preferably, direct aspiration of purulent fluid using a sterile syringe, must be obtained immediately upon breaching the abscess cavity. These specimens must be sent for immediate Gram stain, aerobic, anaerobic, mycobacterial, and fungal cultures. Administering antibiotics prior to culture acquisition significantly increases the risk of false-negative results, severely hampering the infectious disease team's ability to tailor long-term antimicrobial therapy. Once cultures are secured, the anesthesiologist is instructed to administer a broad-spectrum intravenous antibiotic regimen.
1. Incision and Drainage of Thenar Space Infections
The surgical approach to the thenar space can be executed via a volar or dorsal incision, and frequently, a combined approach is necessitated for complete extirpation of the infection. The volar approach is the workhorse incision. The surgeon makes a curvilinear incision adjacent and strictly parallel to the thenar crease, beginning approximately 1 cm proximal to the first web space and extending 3 to 4 cm proximally. This placement avoids crossing flexion creases at a perpendicular angle, thereby mitigating the risk of postoperative flexion contractures.

Dissection proceeds cautiously through the subcutaneous tissue. Using blunt dissection with Metzenbaum scissors or a Freer elevator, the surgeon meticulously penetrates the palmar fascia. This is a high-stakes anatomical zone. The surgeon must actively identify, mobilize, and protect the recurrent motor branch of the median nerve, the proper digital nerves to the thumb, and the princeps pollicis artery. Retraction must be gentle to avoid neuropraxia.


Upon breaching the fascia overlying the adductor pollicis, the abscess cavity is entered. After culture acquisition, aggressive sharp débridement of all necrotic fat, fascia, and devitalized muscle is performed. The cavity is then irrigated with 6 to 9 liters of sterile normal saline. If the infection has tracked dorsally, a counter-incision in the first dorsal web space is required.

2. Incision and Drainage of Midpalmar Space Infections
Accessing the midpalmar space requires a carefully planned volar incision to avoid injury to the superficial palmar arch and the digital neurovascular bundles. A transverse incision made directly within the distal palmar crease is often preferred as it provides excellent exposure while resulting in a cosmetically and functionally superior scar. Alternatively, a longitudinal incision placed over the third or fourth metacarpal, avoiding the weight-bearing surfaces of the palm, can be utilized.

The skin and dense palmar aponeurosis are incised. Deep to the aponeurosis, the surgeon encounters the flexor tendons and the lumbrical muscles. The dissection must proceed bluntly between the flexor tendons of the long and ring fingers or the ring and small fingers to enter the midpalmar space, which lies deep to these structures and superficial to the interosseous fascia.
The superficial palmar arch and the common digital nerves must be visualized and protected with silastic vessel loops or gentle blunt retraction. Once the space is entered and cultures obtained, thorough débridement and high-volume irrigation are performed. Given the depth and complexity of this space, the wound is universally left open, packed loosely with iodoform or plain gauze to facilitate continuous drainage and prevent premature skin closure over an infected cavity.
3. Incision and Drainage of Parona’s Space
When a deep space infection extends proximally into the distal forearm, or in the case of a horseshoe abscess, Parona’s space must be widely decompressed. This is typically approached via a longitudinal volar-ulnar incision in the distal forearm, extending proximally from the wrist crease.

The incision is carried down through the antebrachial fascia. The flexor carpi ulnaris and the ulnar neurovascular bundle are identified and retracted ulnarly, while the massive flexor digitorum profundus (FDP) muscle belly and tendons are retracted radially.

This maneuver exposes the deep, quadrilateral space overlying the pronator quadratus. If a horseshoe abscess is present, a secondary volar-radial incision may be necessary to fully decompress the radial bursa and ensure complete communication and drainage across the entire width of the distal forearm.

Following radical débridement and copious irrigation, drains (such as a Penrose or a small Jackson-Pratt) are frequently placed through these incisions to prevent fluid re-accumulation, and the skin is left open to heal by secondary intention or delayed primary closure.
Complications, Incidence Rates, and Salvage Management
The surgical management of deep space hand infections, while definitive, is fraught with potential complications. These arise not only from the destructive nature of the infection itself but also from the iatrogenic risks inherent in navigating the complex, compact anatomy of the hand. The surgeon must be acutely aware of these potential pitfalls, counsel the patient appropriately preoperatively, and possess the technical armamentarium to manage them effectively should they occur.
The most common complication following deep space infection and subsequent surgical drainage is postoperative stiffness and loss of terminal range of motion. The profound inflammatory response, coupled with necessary surgical dissection and postoperative immobilization, rapidly leads to the formation of dense, restrictive adhesions around the flexor tendons and joint capsules. Iatrogenic neurovascular injury is a catastrophic complication that requires immediate recognition and microsurgical repair. Damage to the recurrent motor branch of the median nerve during a thenar space approach results in devastating loss of thumb opposition, often necessitating delayed tendon transfer (e.g., extensor indicis proprius to abductor pollicis brevis) for functional salvage.
More severe complications include the contiguous spread of infection leading to flexor tendon rupture or osteomyelitis of the metacarpals or phalanges. Tendon rupture secondary to septic necrosis requires complex, staged reconstruction, often utilizing silicone rod placement followed by free tendon grafting once the tissue bed is definitively sterile and supple. Osteomyelitis mandates aggressive bone débridement, potentially resulting in skeletal defects that require delayed bone grafting or, in recalcitrant cases, ray amputation to achieve source control and preserve the function of the remaining hand.
| Complication | Estimated Incidence | Salvage Management and Preventative Strategies |
|---|---|---|
| Postoperative Stiffness | 40% - 60% | Prevention: Early active ROM, rigorous hand therapy. Salvage: Intensive therapy, dynamic splinting, delayed surgical tenolysis/capsulotomy (minimum 6 months post-infection). |
| Iatrogenic Nerve Injury | 1% - 3% | Prevention: Meticulous blunt dissection, wide exposure, |
