Postoperative Closed Irrigation for Pyogenic Flexor Tenosynovitis: The Modified Neviaser Technique
Key Takeaway
Postoperative closed irrigation is a highly effective surgical intervention for acute pyogenic flexor tenosynovitis. Utilizing the modified Neviaser technique, a catheter is introduced proximally at the A1 pulley, allowing continuous or intermittent saline irrigation through the flexor sheath, exiting distally at the A4 pulley. This method reduces bacterial load and hydrostatic pressure while preserving the flexor pulley system, though open drainage remains necessary for chronic infections with tendon necrosis.
Comprehensive Introduction and Patho-Epidemiology
Pyogenic flexor tenosynovitis (PFT) represents one of the most formidable and rapidly progressive orthopedic emergencies encountered in hand surgery, characterized by an aggressive bacterial infection proliferating within the closed, unyielding fibro-osseous space of the digital flexor tendon sheath. The pathophysiology of this condition is fundamentally driven by the accumulation of purulent exudate within a confined synovial space, which precipitates a rapid, exponential increase in localized hydrostatic pressure. This pressure dynamic not only causes the severe, unrelenting pain classically described by Kanavel's four cardinal signs but also critically compromises the delicate microvascular perfusion to the flexor tendons, which are supplied by the highly sensitive vincula brevia and longa. The resulting ischemic environment, coupled with the profound inflammatory cascade, creates a perfect storm for tissue destruction.
At the cellular level, the introduction of pathogenic bacteria into the synovial fluid initiates a massive influx of polymorphonuclear leukocytes (neutrophils). While these cells attempt to phagocytize the invading organisms, they simultaneously release a localized deluge of destructive proteolytic enzymes, including matrix metalloproteinases (MMPs), elastases, and bacterial collagenases. If left untreated, or if inadequately decompressed, this enzymatic degradation combined with microvascular ischemia will inevitably result in irreversible tendon necrosis, catastrophic fibrinous adhesion formation, and profound, permanent loss of hand function. The tendon rapidly loses its inherent tensile strength, transforming from a robust, gliding structure into a friable, necrotic mass susceptible to spontaneous rupture even under minimal physiological loads.
Epidemiologically, pyogenic flexor tenosynovitis most frequently arises from penetrating trauma, such as a seemingly innocuous puncture wound, a thorn prick, or an animal bite, which directly inoculates the synovial sheath with virulent organisms. Staphylococcus aureus remains the most ubiquitous causative pathogen, accounting for the vast majority of acute presentations, with Methicillin-resistant Staphylococcus aureus (MRSA) representing an increasingly prevalent and challenging subset. Other common organisms include Streptococcus species, while Pasteurella multocida and Eikenella corrodens must be highly suspected in the context of feline/canine and human bite wounds, respectively. Hematogenous seeding of the flexor sheath, though rare, can occur in immunocompromised patients or those with disseminated gonococcal infection, necessitating a high index of clinical suspicion when no antecedent trauma is reported.
Postoperative closed irrigation, popularized and meticulously refined as the modified Neviaser technique, remains a foundational cornerstone in the surgical management of acute PFT. By establishing a controlled, proximal-to-distal fluid gradient through the infected tendon sheath, the surgeon can mechanically wash out the overwhelming bacterial load, dilute inflammatory cytokines, and flush away destructive proteolytic enzymes. Crucially, this closed technique achieves these goals while preserving the critical biomechanical integrity of the annular pulley system, thereby mitigating the severe morbidity associated with radical open debridement and extensive pulley sacrifice.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the synovial sheaths and the surrounding fibro-osseous architecture is an absolute prerequisite for successfully executing the modified Neviaser technique without causing catastrophic iatrogenic injury. The digital flexor tendon sheath is a highly specialized, double-walled synovial tube comprising an outer parietal layer and an inner visceral layer (the epitenon), which intimately envelops the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons. This closed system is designed to minimize friction during tendon excursion, providing a highly lubricated gliding surface facilitated by synovial fluid, which also serves as the primary nutritional source for the relatively avascular segments of the tendons via diffusion.
The flexor tendon sheaths of the index, middle, and ring fingers typically exist as isolated anatomical compartments. They originate proximally at the neck of the metacarpal, just proximal to the first annular (A1) pulley, and extend distally to the broad insertion of the FDP tendon at the volar base of the distal phalanx. This isolation generally confines the initial pyogenic process to the affected digit. Conversely, the synovial anatomy of the thumb and the small finger presents a distinctly different and more perilous clinical scenario. The synovial sheath of the thumb continues proximally as the radial bursa, while the sheath of the small finger expands proximally into the ulnar bursa.
Crucially, in a significant majority of the population (approximately 50% to 80%), these radial and ulnar bursae communicate directly at the level of the carpal tunnel within the deep fascial space of the distal forearm, known as Parona's space. Parona's space is anatomically bound anteriorly by the flexor tendons and posteriorly by the pronator quadratus muscle. An aggressive infection originating in the small finger can rapidly track proximally through the ulnar bursa, cross Parona's space, and descend distally into the radial bursa of the thumb, creating the dreaded and limb-threatening "horseshoe abscess." In such complex presentations, the standard digital irrigation system must be aggressively modified to address these extensive proximal bursal extensions to prevent ascending forearm fasciitis.
Biomechanically, the flexor tendons are held in close apposition to the phalanges by a complex retinacular system comprising five robust annular pulleys (A1 through A5) and three pliable cruciate pulleys (C1 through C3). The A2 pulley, located over the proximal phalanx, and the A4 pulley, situated over the middle phalanx, are the primary biomechanical constraints that prevent tendon bowstringing during active flexion. The modified Neviaser technique is specifically designed to access the synovial sheath through the more expendable membranous intervals (such as proximal to the A1 pulley and distal to the A4 pulley), thereby strictly preserving the A2 and A4 pulleys. Iatrogenic division of these critical pulleys during decompression will result in profound biomechanical failure, loss of active range of motion, and severe flexor lag, severely compromising the functional outcome even if the infection is successfully eradicated.
Exhaustive Indications and Contraindications
The critical decision to utilize closed postoperative irrigation versus proceeding to radical open debridement depends entirely on the chronicity of the infection, the host's physiological status, and the intraoperative macroscopic appearance of the flexor tendon and its surrounding synovial fluid. The Michon classification system remains the universally accepted standard for staging pyogenic flexor tenosynovitis and directly dictates the appropriate surgical intervention. Proper patient selection is the single most important determinant of success when employing the modified Neviaser technique; attempting closed irrigation on an inappropriately advanced infection will inevitably result in treatment failure and profound morbidity.
Favorable indications for closed postoperative irrigation encompass early, acute presentations that have not yet progressed to structural tissue degradation. Specifically, patients presenting within 24 to 48 hours of symptom onset or the initial penetrating trauma are the ideal candidates. According to the Michon staging system, closed irrigation is highly effective and definitively indicated for Stage I and Stage II infections. In Michon Stage I, the intraoperative assessment reveals a sheath distended with cloudy, serous, or serosanguineous exudate, but the surrounding synovium is merely hyperemic and inflamed, with no frank pus. In Michon Stage II, the sheath contains frankly purulent fluid under pressure, yet the flexor tendon itself remains structurally viable, maintaining its normal pearly-white, glistening appearance without evidence of surface fragmentation or necrosis.
Conversely, closed catheter irrigation is absolutely contraindicated, and immediate open surgical drainage becomes mandatory, under several specific conditions. The primary contraindication is a Michon Stage III infection. In this advanced stage, the flexor tendon appears grossly necrotic, dull, yellowish, or fragmented, and the surrounding pulley system may be partially destroyed by the enzymatic onslaught. Attempting to irrigate a necrotic tendon is futile; the dead tissue serves as an un-eradicable nidus for ongoing sepsis. Furthermore, chronic infections or delayed presentations characterized by extensive loculated abscesses, thick fibrinous adhesions, or organized purulence within the sheath preclude the use of closed irrigation, as these mechanical barriers will prevent the free, unimpeded flow of the irrigant from proximal to distal.
Atypical pathogens also represent a strict contraindication to simple closed irrigation. Indolent infections caused by mycobacterial species (e.g., Mycobacterium marinum) or deep fungal organisms typically incite a profound, granulomatous hypertrophic tenosynovitis. These atypical infections do not respond to simple fluid washout; they mandate an extensive, meticulous open synovectomy to physically excise the diseased, hypertrophic tissue burden.
Indications and Contraindications by Michon Staging
| Michon Stage | Intraoperative Findings | Tendon Viability | Recommended Surgical Intervention |
|---|---|---|---|
| Stage I | Cloudy, serous, or serosanguineous fluid; hyperemic, inflamed synovium; no frank purulence. | 100% Viable, glistening, structurally intact. | Closed Postoperative Irrigation (Modified Neviaser Technique). |
| Stage II | Frank purulence under pressure within the synovial sheath; significant synovial hypertrophy. | Viable, glistening, no macroscopic evidence of necrosis or fragmentation. | Closed Postoperative Irrigation (Modified Neviaser Technique). |
| Stage III | Thick, organized purulence; loculated abscesses; destruction of the pulley system. | Necrotic, dull, fragmented, yellowish, loss of structural integrity. | Open Debridement, extensive tenosynovectomy, potential staged reconstruction. |
| Atypical | Granulomatous tissue, hypertrophic "rice body" synovitis (Mycobacterial/Fungal). | Variable, often structurally compromised by chronic invasive granulomas. | Open Radical Synovectomy, tailored antimicrobial therapy. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning, diagnostic workup, and meticulous patient positioning are critical to the safe and effective execution of the modified Neviaser technique. While traditional "templating" in orthopedics often refers to fracture fixation or arthroplasty, in the context of pyogenic flexor tenosynovitis, templating involves the precise preoperative mapping of the anticipated surgical incisions, the clinical estimation of proximal bursal involvement, and the strategic planning of catheter routing. The surgeon must carefully examine the hand to determine if the infection is confined to a single digital sheath (index, middle, ring) or if there is clinical evidence—such as swelling and tenderness proximal to the wrist crease—suggesting extension into the radial bursa, ulnar bursa, or Parona's space.
Preoperative diagnostic imaging and laboratory investigations form the foundation of the surgical plan. Standard multi-planar radiographs of the affected hand are mandatory to rule out retained radiopaque foreign bodies, underlying fractures, or established osteomyelitis, which would necessitate a radical alteration of the surgical approach. High-resolution point-of-care ultrasound (POCUS) has emerged as an invaluable adjunct, allowing the surgeon to non-invasively visualize fluid distension within the tendon sheath, confirm the presence of loculations, and map the proximal extent of the effusion into the forearm. Concurrently, baseline inflammatory markers, including C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and a complete blood count (CBC) with differential, must be obtained to monitor the systemic response to the localized infection and track postoperative therapeutic efficacy.
The selection of anesthesia is a critical safety consideration. The procedure must be performed under a reliable regional block (such as an ultrasound-guided axillary or supraclavicular brachial plexus block) or general anesthesia. Local infiltration anesthesia (e.g., a digital block or wide local infiltration) is strictly and unequivocally contraindicated. Injecting local anesthetic directly into an infected, pressurized space not only risks the mechanical dissemination of virulent bacteria into adjacent, previously uninvolved fascial planes, but it also fails to provide the necessary proximal analgesia required for potential extension into the palm or forearm if a horseshoe abscess is encountered.
Patient positioning and the management of the pneumatic tourniquet require strict adherence to established orthopedic infection protocols. The patient is positioned supine with the affected upper extremity extended on a radiolucent hand table. The limb is prepped and draped using standard sterile technique. A pneumatic tourniquet is applied to the proximal arm. Crucially, the surgeon must not exsanguinate the limb using an Esmarch bandage. Mechanically compressing the infected extremity with an Esmarch bandage will forcefully milk purulent material proximally, potentially rupturing the synovial sheath and disseminating the localized infection into the deep fascial spaces of the hand and forearm. Instead, the surgeon must rely on gravity exsanguination: the arm is simply elevated at 60 to 90 degrees for 3 to 5 minutes to allow venous drainage before the tourniquet is rapidly inflated to 250 mm Hg (or 100 mm Hg above the patient's systolic blood pressure).
Step-by-Step Surgical Approach and Fixation Technique
The modified Neviaser technique requires a meticulous, systematic approach to establish a reliable proximal-to-distal irrigation gradient while strictly preserving the biomechanical integrity of the flexor pulley system. The "fixation" in this context refers to the secure anchoring of the inflow catheters and outflow drains to the skin, which is paramount to prevent inadvertent dislodgment during the crucial postoperative continuous irrigation phase.
Step 1: Proximal Exposure (The A1 Pulley)
The primary objective of the proximal exposure is to safely access the membranous, proximal-most portion of the flexor tendon sheath immediately proximal to the A1 pulley. The surgeon begins by making a straight transverse incision parallel to the distal palmar crease, directly overlying the metacarpal neck of the affected digit. Alternatively, a volar zigzag (Bruner) incision can be utilized over the A1 pulley region to provide extensile exposure if conversion to open drainage becomes necessary.
Careful blunt dissection is carried out through the subcutaneous adipose tissue. The surgeon must meticulously identify, mobilize, and protect the digital neurovascular bundles, which lie volar and adjacent to the flexor sheath on either side. These structures are gently retracted using blunt hook retractors to expose the proximal origin of the flexor sheath. Upon adequate visualization, the surgeon will typically observe the synovial sheath bulging significantly under high hydrostatic tension. The underlying fluid—whether cloudy, serosanguineous, or frankly purulent—is often clearly visible through the translucent synovial membrane.
Step 2: Sheath Decompression and Culture
With the proximal sheath exposed, a small, precise transverse or V-shaped window is sharply created in the membranous sheath immediately proximal to the proximal edge of the A1 pulley. As the pressurized fluid is released, the surgeon must immediately capture the exudate using sterile swabs or a syringe. This fluid is urgently dispatched to the microbiology laboratory for comprehensive analysis, including aerobic, anaerobic, and acid-fast bacilli (AFB) cultures, fungal cultures, and an immediate Gram stain to guide empiric antibiotic therapy.
Step 3: Distal Exposure (The A4 Pulley)
To establish a functional outflow tract, the distal aspect of the synovial sheath must be opened. The surgeon makes a second, distinct incision in the midaxial line on either the radial or ulnar side of the finger, located precisely in the distal portion of the middle phalanx. Alternatively, a careful transverse incision can be made directly over the volar distal interphalangeal (DIP) flexion crease.
Dissection is carried down through the subcutaneous tissue to the fibro-osseous canal, strictly avoiding the distal neurovascular structures. The A4 pulley is identified, and a small window is sharply created in the flexor sheath immediately distal to the distal edge of the A4 pulley. The surgeon must exercise extreme caution to ensure the broad insertion of the FDP tendon into the base of the distal phalanx is not inadvertently compromised or lacerated during this distal decompression.
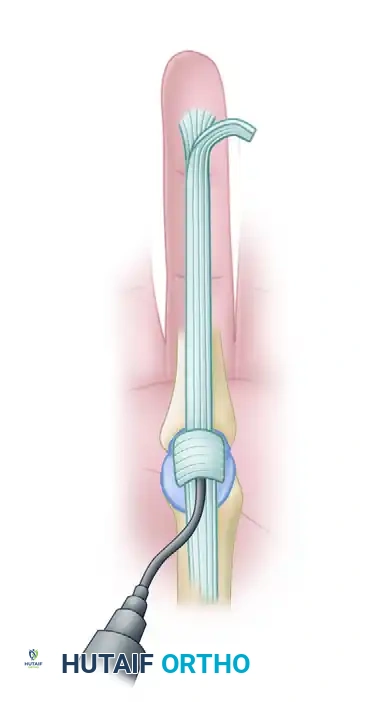
Step 4: Catheter Insertion, Routing, and Fixation
The efficacy of the irrigation system is entirely dependent on a unidirectional, proximal-to-distal flow that mechanically flushes bacteria and debris out of the dependent distal wound. Using smooth, non-toothed forceps or a fine hemostat, the surgeon carefully introduces a 16-gauge or 18-gauge pliable polyethylene catheter (a pediatric feeding tube or a dedicated epidural catheter is highly effective) into the proximal window beneath the A1 pulley.
The catheter is advanced gently from proximal to distal within the flexor sheath for a distance of exactly 1.5 to 2.0 cm. Do not advance the catheter further. A catheter inserted too deeply can cause localized mechanical pressure necrosis on the underlying FDS or FDP tendons, leading to delayed rupture. Distally, a small sliver of a sterile rubber drain (e.g., a 1/4-inch Penrose drain) is placed into the distal window beneath the A4 pulley and brought out through the distal skin incision to mechanically maintain the patency of the outflow tract.
Step 5: System Testing and Closure
Before closure, the system must be rigorously tested. Using a 30-mL syringe filled with sterile normal saline, the surgeon forcefully irrigates the sheath through the proximal catheter. The surgeon must visually verify that the fluid flows freely and unimpeded out of the distal wound, effectively clearing immediate fibrinous debris.
Once patency is confirmed, the proximal palmar wound is closed loosely around the inflow catheter using non-absorbable monofilament sutures (e.g., 4-0 Nylon). The fixation of the catheter is critical: it must be sutured securely to the palmar skin using a Roman sandal or finger-trap suture technique to prevent inadvertent pull-out during postoperative mobilization. The distal wound is closed around the rubber drain, ensuring it is left deliberately loose. A tight distal closure will obstruct outflow, leading to fluid extravasation into the digit and precipitating an iatrogenic compartment syndrome. The hand is then wrapped in a bulky, non-compressive soft dressing, supported by a volar resting splint in the intrinsic-plus position.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and aggressive antibiotic therapy, the management of pyogenic flexor tenosynovitis carries a significant risk of severe complications. The closed, relatively avascular nature of the flexor tendon sheath makes it highly susceptible to irreversible damage if the infection is not rapidly and completely eradicated. The most devastating complications arise from either delayed presentation, unrecognized Michon Stage III necrosis, or technical failures in the irrigation system leading to persistent, localized sepsis.
Tendon necrosis and subsequent spontaneous rupture represent the most catastrophic structural failures. This occurs when the inflammatory pressure and bacterial collagenases overwhelm the delicate vincula supply, leading to ischemic death of the tendon substance. If a necrotic tendon is erroneously treated with closed irrigation, the dead tissue acts as a persistent nidus for infection, leading to chronic purulent drainage and eventual rupture. In such salvage scenarios, the surgeon must abandon the closed system, return to the operating room, and perform a radical open debridement. This involves extensive tenosynovectomy, complete excision of the necrotic tendon, and potentially the placement of a silicone tendon spacer (Hunter rod) to preserve the fibro-osseous canal for a staged tendon reconstruction once the infection has been definitively cleared.
Postoperative stiffness and severe flexion contractures are the most common functional complications, occurring in up to 30-40% of cases despite successful eradication of the infection. This stiffness is driven by the aggressive formation of dense, fibrinous peritendinous adhesions between the flexor tendons and the parietal sheath, effectively tethering the gliding mechanism. Salvage management for severe, refractory stiffness typically involves an intensive, prolonged course of specialized hand therapy. If therapy fails after 3 to 6 months of maximal effort, a formal open tenolysis may be indicated, though the results are often unpredictable and carry a risk of re-triggering the inflammatory cascade.
Iatrogenic compartment syndrome of the digit is a direct technical complication of the modified Neviaser technique. It occurs when the distal outflow tract becomes occluded (either by a tight skin closure, a kinked Penrose drain, or thick fibrinous debris) while continuous proximal irrigation is maintained. The irrigant extravasates into the closed compartments of the finger, leading to acute microvascular compromise. Immediate salvage requires cessation of the irrigation, removal of the distal sutures, and wide opening of the distal wound to decompress the digit.
Complications and Salvage Management Summary
| Complication | Estimated Incidence | Pathophysiology | Salvage Management / Intervention |
|---|---|---|---|
| Severe Stiffness / Adhesions | 30% - 40% | Fibrinous exudate organizing into dense peritendinous scar tissue. | Aggressive early active motion; late open tenolysis if refractory. |
| Tendon Necrosis / Rupture | 5% - 10% | Ischemic death via vincula compromise and enzymatic collagenolysis. | Open debridement, tendon excision, staged Hunter rod reconstruction. |
| Iatrogenic Compartment Syndrome | < 5% | Occlusion of distal outflow tract leading to fluid extravasation into the digit. | Immediate cessation of irrigation, release of distal skin sutures. |
| Persistent/Ascending Infection | 5% - 15% | Retained loculations, unrecognized Stage III, or atypical pathogens. | Conversion to radical open drainage and extensive synovectomy. |
| Digital Amputation | 1% - 3% | Overwhelming sepsis, irreversible necrosis, or gangrene. | Terminal ray amputation to achieve source control and save the hand. |
(Above: An example of a Michon Stage III infection with gross purulence and early tendon necrosis, which mandates open drainage rather than closed irrigation.)
Phased Post-Operative Rehabilitation Protocols
The ultimate functional success of the modified Neviaser technique is not determined solely in the operating theater; it relies heavily on a meticulous, highly disciplined postoperative ward care regimen and a phased rehabilitation protocol. The postoperative phase is a delicate balance between aggressively flushing the infection from the sheath and initiating early motion to prevent the catastrophic formation of peritendinous adhesions.
During the initial 48 hours postoperatively, the primary focus is on continuous or high-frequency intermittent irrigation. The established protocol dictates that the wounds are irrigated with 30 mL of sterile normal saline every 2 hours via the proximal catheter. Alternatively, a continuous gravity-drip IV tubing system can be connected to the catheter and set at a rate of 10 to 15 mL per hour. During every single flush, the nursing staff and surgical team must visually verify the patency of the system by observing the free, unimpeded flow of the irrigant out of the distal rubber drain. If resistance is encountered, the surgeon must be immediately notified, as the catheter may be kinked, or the outflow tract may be blocked by thick fibrinous debris, requiring urgent unblocking or adjustment to prevent fluid extravasation.
At the 48-hour mark, a critical clinical evaluation is performed. The bulky surgical dressing is removed under strict sterile conditions on the ward to allow for direct examination of the affected digit. The surgeon looks for definitive signs of clinical resolution: a marked decrease in digital erythema, a reduction in fusiform swelling, and, most importantly, significantly diminished pain upon passive extension of the digit. If these signs of resolution are clearly present, and the effluent fluid is clear, the inflow catheter and the distal rubber drain are carefully removed.
Once the hardware is removed (typically at 48 to 72 hours), the rehabilitation phase shifts immediately to aggressive adhesion prevention. A lighter, non-restrictive dressing is applied. Under the strict guidance of a specialized certified hand therapist (CHT), the patient begins an aggressive regimen of early active motion (EAM) and place-and-hold exercises. Passive range of motion is minimized initially to prevent excessive stress on the recovering tendon. Edema control is paramount during this phase, utilizing compressive wraps (e.g., Coban) and strict limb elevation. Between therapy sessions, the hand is rested in a custom-molded thermoplastic splint in the intrinsic-plus position (wrist in 20° to 30° extension, metacarpophalangeal joints in 70° to 90° flexion, and interphalangeal joints in full extension) to maintain collateral ligament length and prevent contractures.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the surgical management of pyogenic flexor tenosynovitis is deeply rooted in a rich history of landmark orthopedic literature, which continues to inform modern clinical guidelines and best practices. The foundational understanding of this disease process was established by Allen B. Kanavel in the early 20th century. Kanavel's seminal anatomical studies and clinical observations defined the four cardinal signs of flexor tenosynovitis (fusiform swelling, flexed resting posture, tenderness along the flexor sheath, and excruciating pain on passive extension), which remain the gold standard for clinical diagnosis today. Kanavel initially advocated for extensive open incisions, which, while life-saving in the pre-antibiotic era, often resulted in devastatingly stiff and non-functional hands.
The paradigm shifted significantly with the introduction of closed tendon sheath irrigation. The technique was popularized and refined by Neviaser, who recognized that mechanically flushing the closed synovial space could eradicate the bacterial load while preserving the critical annular pulley system. The
