Arthroscopic TFCC Débridement & Ulnar Shortening: An Intraoperative Masterclass

Key Takeaway
Join us in the OR for an immersive masterclass on arthroscopic TFCC débridement and ulnar shortening. We'll meticulously cover patient positioning, portal placement, precise débridement techniques, and controlled ulnar head resection. Learn to navigate critical anatomy, avoid pitfalls, and ensure optimal outcomes for ulnar wrist pain and abutment syndrome.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows and colleagues, to the operating theater and to this definitive masterclass on ulnar-sided wrist pathology. Historically relegated to the ambiguous moniker of the "black box of the wrist," the ulnocarpal articulation and its primary stabilizing structure, the Triangular Fibrocartilage Complex (TFCC), have become areas of profound surgical refinement over the last three decades. Today, we are addressing a ubiquitous yet technically demanding clinical scenario: symptomatic TFCC tears inextricably linked to, and often exacerbated by, ulnar abutment syndrome (ulnar impaction syndrome). Our surgical intervention will consist of an arthroscopically assisted TFCC débridement seamlessly followed by an arthroscopic ulnar shortening, commonly referred to as the arthroscopic wafer procedure.
This intraoperative masterclass is designed to elucidate the meticulous precision, profound understanding of wrist biomechanics, and advanced arthroscopic dexterity required to execute this combined procedure successfully. The transition from open arthrotomies and diaphyseal ulnar shortening osteotomies (USO) to all-arthroscopic management represents a paradigm shift in hand surgery. This evolution offers patients diminished morbidity, accelerated rehabilitation, and preservation of the pristine distal radioulnar joint (DRUJ) extra-articular anatomy. However, this minimally invasive approach demands an uncompromising mastery of intra-articular spatial orientation and fluoroscopic interpretation.
The epidemiology of TFCC pathology is bimodal, presenting as acute traumatic tears in young, active individuals and as chronic, attritional tears in older populations. When combined with ulnar abutment syndrome, the pathology is almost exclusively degenerative, driven by altered load transmission across the ulnocarpal axis. Repetitive axial loading, particularly in positions of ulnar deviation and pronation, accelerates the mechanical degradation of the central articular disc. Recognizing this patho-epidemiological link is the cornerstone of our surgical rationale: to treat the tear without addressing the underlying positive ulnar variance is to invite inevitable clinical failure.
Therefore, our objective is twofold. First, we must meticulously débride the unstable, inflammatory margins of the TFCC tear to eliminate mechanical catching and chemical synovitis. Second, we must decompress the ulnocarpal joint by resecting the distal dome of the ulnar head, effectively converting an ulnar-plus or ulnar-neutral variance to an ulnar-minus variance, thereby halting the degenerative cascade. This chapter will guide you through every nuance of this elegant, highly effective surgical solution.
Detailed Surgical Anatomy and Biomechanics
Before we even consider making an incision or establishing a portal, we must review the intricate architectural and biomechanical framework of the ulnar wrist. A superficial understanding of this anatomy will invariably lead to iatrogenic injury and suboptimal outcomes.
The Triangular Fibrocartilage Complex Architecture
The TFCC is not merely a passive fibrocartilaginous disc; it is a highly specialized, multi-component ligamentous complex that serves as the primary stabilizer of the DRUJ and the principal shock absorber for the ulnar carpus. The central articular disc is avascular and aneural, rendering it incapable of primary healing but highly susceptible to mechanical wear. Radially, it attaches to the hyaline cartilage-covered distal lip of the sigmoid notch of the radius. Ulnarly, the anatomy becomes vastly more complex, bifurcating into a superficial layer that inserts onto the base of the ulnar styloid and a deep layer (the ligamentum subcruentum) that inserts into the fovea at the base of the ulnar styloid.
The peripheral margins of the TFCC are highly vascularized, supplied by branches of the ulnar artery and the anterior/posterior interosseous arteries. This vascularity is crucial for the healing of peripheral tears (Palmer Type 1B) but is largely irrelevant for the central degenerative tears (Palmer Type II) we are addressing today. The complex is further reinforced by the dorsal and palmar radioulnar ligaments, the ulnocarpal ligaments (ulnolunate and ulnotriquetral), the meniscus homologue, and the extensor carpi ulnaris (ECU) subsheath.
During arthroscopy, recognizing the tensioning of these structures during forearm rotation is critical. The dorsal radioulnar ligament tightens in pronation, while the palmar radioulnar ligament tightens in supination. Aggressive débridement that breaches these critical peripheral stabilizing ligaments will precipitate catastrophic, iatrogenic DRUJ instability. Our surgical mandate is to confine our resection strictly to the avascular central articular disc.
Ulnocarpal Biomechanics and Abutment Pathophysiology
The biomechanical principles governing the wrist were elegantly quantified by Palmer and Werner. In a normal wrist with ulnar-zero variance, the radius absorbs approximately 80% of the axial load, while the ulna absorbs the remaining 20%. However, this load distribution is highly dynamic and exquisitely sensitive to changes in ulnar variance. A mere 2.5 mm increase in ulnar length (ulnar-plus variance) shifts the ulnar load bearing from 20% to a staggering 42%.
This pathological load shift is the fundamental driver of ulnar abutment syndrome. The repetitive impaction of the ulnar head against the proximal pole of the lunate and the triquetrum leads to a predictable sequence of degenerative changes. Initially, the central articular disc of the TFCC undergoes attritional thinning and subsequent perforation (Palmer Type IIA and IIB). As the abutment continues, chondromalacia develops on the ulnar head and the proximal ulnar aspect of the lunate (Palmer Type IIC).
If left unaddressed, this relentless mechanical conflict progresses to attenuation and eventual rupture of the lunotriquetral (LT) interosseous ligament (Palmer Type IID), culminating in advanced ulnocarpal and DRUJ arthritis (Palmer Type IIE). By performing an arthroscopic ulnar shortening (wafer procedure), we are mechanically uncoupling the ulnocarpal joint. Resecting 2 to 3 mm of the distal ulna beneath the TFCC tear effectively normalizes the load transmission, alleviating the impaction forces and providing profound, durable pain relief.
Exhaustive Indications and Contraindications
Patient selection is the absolute determinant of success in arthroscopic TFCC débridement and ulnar shortening. This procedure is not a panacea for all ulnar-sided wrist pain; it is a highly targeted intervention for a specific pathoanatomical cascade.
Patient Selection Criteria
The ideal candidate for this combined procedure presents with chronic, ulnar-sided wrist pain that is exacerbated by power grip, pronation, and ulnar deviation. Clinical examination typically reveals point tenderness over the TFCC (between the FCU and ECU tendons), a positive ulnar impaction test, and pain with passive compression of the ulnocarpal joint. Crucially, these patients must have failed a rigorous course of conservative management, including non-steroidal anti-inflammatory drugs (NSAIDs), prolonged splinting, activity modification, and potentially intra-articular corticosteroid injections.
From a classification standpoint, we are targeting Palmer Type II (degenerative) lesions. Specifically, Palmer Type IIA (TFCC wear), IIB (TFCC wear with lunate/ulnar chondromalacia), and IIC (TFCC perforation with chondromalacia) are the prime indications for arthroscopic débridement and wafer resection. In these stages, the lunotriquetral ligament remains intact, and the DRUJ is stable.
Conversely, Palmer Type IID (lunotriquetral ligament tear) and IIE (ulnocarpal arthritis) often require more extensive reconstructive or salvage procedures, such as an open ulnar shortening osteotomy (to tighten the ulnocarpal ligaments) or a limited ulnocarpal fusion. Furthermore, the degree of ulnar-plus variance is a critical determining factor. The arthroscopic wafer procedure is generally indicated for patients with an ulnar-plus variance of 1 to 3 mm. Attempting an arthroscopic resection for variances greater than 4 mm is technically prohibitive, risks violating the sigmoid notch, and is better served by an extra-articular diaphyseal ulnar shortening osteotomy.
Summary Table of Indications and Contraindications
| Category | Arthroscopic TFCC Débridement & Wafer Procedure |
|---|---|
| Primary Indications | Palmer Type IIA, IIB, and IIC degenerative TFCC tears. |
| Variance Criteria | Ulnar-plus variance of 1 mm to 3 mm (or symptomatic ulnar-neutral). |
| Clinical Presentation | Chronic ulnocarpal abutment pain refractory to >3 months of conservative care. |
| Absolute Contraindications | Active joint infection; DRUJ instability; advanced ulnocarpal arthritis (Palmer IIE). |
| Relative Contraindications | Ulnar-plus variance > 4 mm (favor open USO); reverse obliquity of the sigmoid notch; complete lunotriquetral ligament dissociation (Palmer IID). |
| Anatomical Considerations | A thick, intact TFCC without a central perforation makes the arthroscopic wafer technically challenging, often requiring a deliberate iatrogenic central perforation to access the ulnar head. |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning for an arthroscopic wafer procedure requires meticulous attention to radiographic detail. The success of the operation hinges on calculating the exact millimeter resection required to decompress the joint without destabilizing the DRUJ.
Diagnostic Workup and Advanced Imaging
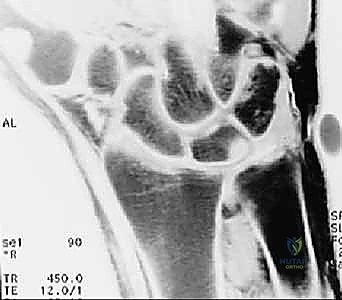
The radiographic evaluation begins with a high-quality, standardized wrist series. The most critical image is the Palmer 90/90 neutral rotation view. Because ulnar variance changes dynamically with forearm rotation—increasing in pronation and decreasing in supination—a standardized view is mandatory to prevent gross miscalculation. The patient is positioned with the shoulder abducted to 90 degrees, the elbow flexed to 90 degrees, and the forearm in absolute neutral rotation.

FIG 3 • A. Ulnar-plus variance unequivocally demonstrated on a standardized 90/90 neutral rotation PA view, confirming the mechanical basis for the patient's abutment syndrome.
On this view, we carefully scrutinize the proximal ulnar pole of the lunate and the radial aspect of the triquetrum for subchondral sclerosis or cystic changes, which are pathognomonic for chronic impaction. We then template the exact amount of ulnar shortening required. Our surgical objective is to achieve a final ulnar variance of minus 1 to minus 2 mm.
Advanced imaging, specifically Magnetic Resonance Imaging (MRI), is indispensable. We utilize high-resolution 3T MRI, often with intra-articular gadolinium (MR arthrography), to delineate the exact morphology of the TFCC tear and assess the integrity of the intrinsic carpal ligaments.
FIG 3 • B,C. T1 and T2-weighted MRIs of a wrist with ulnar abutment. Note the hyperintense signal on the T2 sequence at the ulnar proximal lunate, indicative of intraosseous edema and microtrabecular trauma secondary to chronic impaction.
The MRI allows us to map the extent of the central perforation. If the tear is small, we know we will need to enlarge it during the débridement phase to gain adequate access to the ulnar dome for the subsequent wafer resection. Furthermore, the MRI helps rule out concomitant pathologies, such as Kienböck's disease or occult carpal fractures, which would drastically alter our surgical algorithm.
Operating Room Setup and Patient Positioning
The patient is positioned supine on the operating table with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is placed high on the brachium. Regional anesthesia, typically an axillary or supraclavicular brachial plexus block, is preferred as it provides excellent intraoperative muscle relaxation and prolonged postoperative analgesia.
We employ a specialized wrist arthroscopy traction tower. The index and long fingers are secured in sterile Chinese finger traps. We apply approximately 10 to 15 pounds of longitudinal traction. It is imperative that counter-traction is applied via a padded arm-holder positioned proximal to the elbow, ensuring the traction force is isolated across the radiocarpal and midcarpal joints.
A mini C-arm fluoroscope is positioned perpendicular to the hand table, allowing for seamless transition between arthroscopic visualization and radiographic confirmation. The fluoroscopy monitor should be positioned directly adjacent to the arthroscopy monitor, directly in the surgeon's line of sight, to facilitate real-time correlation during the ulnar resection phase.
Step-by-Step Surgical Approach and Fixation Technique
We now transition to the operative execution. This procedure demands a systematic, unhurried approach, respecting the delicate neurovascular anatomy of the dorsal wrist.
Portal Placement and Diagnostic Arthroscopy
We begin by mapping our portals. The dorsal sensory branch of the radial nerve (DSBRN) and the dorsal sensory branch of the ulnar nerve (DSBUN) are at significant risk during portal establishment. We primarily utilize the 3-4 portal (viewing) and the 4-5 or 6R portal (working).
To establish the 3-4 portal, located just distal to Lister's tubercle between the EPL and EDC tendons, I make a precise, longitudinal skin incision—never transverse, to avoid transecting superficial nerve branches. I utilize a mosquito hemostat to bluntly dissect down through the subcutaneous tissues to the radiocarpal capsule. A sharp trocar is used only to pierce the capsule, immediately exchanged for a blunt obturator to enter the joint, thereby preventing iatrogenic scuffing of the scaphoid or lunate articular surfaces.
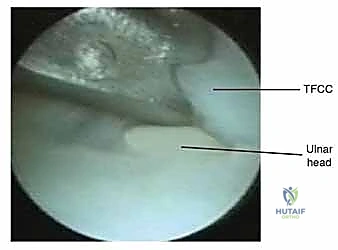
Once the 2.7mm, 30-degree arthroscope is introduced and the joint is distended with lactated Ringer's solution, we perform a comprehensive diagnostic sweep. We assess the radioscaphocapitate ligament, the scapholunate interosseous ligament, and the articular surfaces of the proximal carpal row. We then direct our attention ulnarly to visualize the TFCC.

Intraoperative arthroscopic view demonstrating a central degenerative TFCC tear (Palmer Type II), characterized by frayed, unstable fibrillated margins overlying the ulnar head.

Further arthroscopic inspection reveals the extent of the degenerative perforation, exposing the chondromalacic articular surface of the distal ulna beneath the tear.
Mechanical TFCC Débridement
Having identified the central degenerative tear, we establish our working portal, typically the 4-5 portal or the 6R portal, using the same meticulous blunt dissection technique. The goal of this phase is to excise the inflamed, redundant, and mechanically unstable edges of the torn TFCC until a smooth, stable perimeter of healthy fibrocartilage is achieved.

Introduction of a mechanical shaver through the working portal. The shaver is carefully positioned to engage the unstable radial and palmar margins of the TFCC tear.
We utilize a combination of mechanized shavers (2.0mm or 2.9mm), arthroscopic punches, and radiofrequency (RF) wands. The motorized shaver, set to oscillate, is highly effective for rapidly clearing the fibrillated tissue.
Active mechanical débridement of the TFCC. The suction function of the shaver clears debris, maintaining optimal visualization of the tear margins and the underlying ulnar head.
Great care must be taken to maintain the integrity of the peripheral attachments. We resect only the avascular central portion. If the existing perforation is too small to allow access for the subsequent ulnar shortening, we deliberately enlarge the tear centrally, creating a sufficient window to introduce our burr directly over the ulnar dome.
Post-débridement view showing a clean, stable rim of the TFCC. The central perforation has been appropriately contoured to provide unimpeded access to the distal ulna for the wafer resection.
Arthroscopic Wafer Procedure and Ulnar Shortening
With the TFCC débrided and the ulnar head exposed, we proceed to the arthroscopic wafer procedure. This is the most technically demanding portion of the operation. The objective is to resect 2 to 3 mm of the distal ulnar dome, decorticating the articular cartilage and the underlying subchondral bone, to achieve an ulnar-minus variance.

Introduction of a high-speed, 2.9mm shielded arthroscopic burr through the central TFCC defect, making initial contact with the articular cartilage of the ulnar head.
We introduce a shielded, high-speed arthroscopic burr (typically 2.9mm or 3.5mm) through the working portal. The shield of the burr must always be oriented dorsally or towards the carpus to protect the lunate and triquetrum from catastrophic iatrogenic damage.

Active burring of the ulnar dome. The resection begins centrally and progresses radially and ulnarly. Copious irrigation is critical to clear bone debris and prevent thermal necrosis.
The resection must be systematic. I typically begin centrally and work radially towards the sigmoid notch, and then ulnarly towards the styloid. Crucially, the resection must stop short of the DRUJ. We must preserve the vertical articular surface of the ulnar head that articulates with the sigmoid notch of the radius to maintain DRUJ stability and kinematics.

Progressive decortication of the ulnar head. The subchondral bone is exposed and systematically resected to achieve the templated depth.
To gauge the depth of resection, we use the known diameter of the burr head as a reference. If using a 2.9mm burr, sinking the burr to its equator indicates approximately 1.5mm of resection; sinking it completely flush with the surrounding bone indicates nearly 3mm of resection.

Arthroscopic view confirming a uniform, flat resection bed across the central portion of the distal ulna. The peripheral margins adjacent to the DRUJ are carefully preserved.

Assessment of the resection gap. With the wrist in neutral, there should be a visible clearance between the deep surface of the TFCC and the newly created ulnar plateau.
Throughout the burring process, we frequently pause and utilize the mini C-arm fluoroscope to confirm the depth and uniformity of the resection. The fluoroscopic image must demonstrate a flat, even resection plane, devoid of any residual dorsal or volar osseous ridges that could cause recurrent localized abutment.

Intraoperative fluoroscopy is paramount. This AP view demonstrates the burr in position, allowing real-time assessment of the resection depth relative to the distal radius.

Fluoroscopic confirmation of the completed wafer procedure. Note the conversion to an ulnar-minus variance, successfully decompressing the ulnocarpal joint.
Once the desired ulnar-minus variance is confirmed radiographically, we perform a final, meticulous sweep of the joint with the motorized shaver to evacuate all residual osseous debris and cartilage fragments. Failure to thoroughly irrigate and clear this debris can lead to severe postoperative synovitis and the formation of loose bodies.

Final arthroscopic view after thorough irrigation. The resected ulnar bed is clean, the TFCC margins are stable, and the ulnocarpal joint is effectively decompressed.
The portals are then closed with simple non-absorbable sutures, and a bulky, soft sterile dressing is applied. A volar wrist splint is placed to immobilize the joint in neutral position.
Complications, Incidence Rates, and Salvage Management
While arthroscopic TFCC débridement and wafer resection is highly successful in appropriately selected patients, it is not without risk. The margin for error is narrow, and technical missteps can lead to profound functional impairment.
Intraoperative and Postoperative Complications
The most frequent complication is neuropraxia or structural injury to the dorsal sensory branches of the ulnar or radial nerves. The DSBUN is particularly vulnerable during the establishment of the 6U portal. Strict adherence to longitudinal skin incisions and blunt subcutaneous spreading is the only reliable method to mitigate this risk. Should a painful neuroma develop postoperatively, surgical excision and nerve burying into the pronator quadratus muscle belly may be required.
Iatrogenic articular cartilage damage to the lunate, triquetrum, or the sigmoid notch of the radius is a severe technical failure. This usually occurs due to aggressive, unshielded burr use or forcing trocars into a tight, under-distracted joint. Prevention relies on adequate traction (10-15 lbs), maintaining the burr shield dorsally, and meticulous spatial awareness.
Under-resection of the distal ulna leads to persistent ulnar abutment syndrome and failure of the operation. This highlights the necessity of frequent intraoperative fluoroscopic checks. Conversely, over-resection, particularly if the burr violates the lateral articular margins of the ulnar head, can destabilize the DRUJ, leading to painful subluxation and accelerated arthrosis.
Summary Table of Complications and Salvage Strategies
| Complication | Estimated Incidence | Etiology/Risk Factor | Salvage/Management Strategy |
|---|---|---|---|
| DSBUN/DSBRN Neuropraxia | 2% - 5% | Transverse incisions; sharp dissection; aggressive retractor use. | Observation (often resolves in 6-12 weeks); Gabapentinoids; Neuroma excision if refractory. |
| Iatrogenic Cartilage Scuffing | 1% - 3% | Poor portal trajectory; unshielded burr use; inadequate joint distraction. | Chondroplasty; if severe, may accelerate need for salvage procedures (e.g., partial wrist fusion). |
| Inadequate Resection (Persistent Abutment) | 5% - 10% | Failure to use intraoperative fluoroscopy; misjudging burr depth. | Revision arthroscopic resection or conversion to open diaphyseal ulnar shortening osteotomy. |
| DRUJ Instability | < 2% | Violating the sigmoid notch articulation; over-resection of peripheral TFCC attachments. | Open DRUJ ligamentous reconstruction (e.g., Adams-Berger procedure) or salvage (Darrach/Sauvé-Kapandji). |
| Postoperative Synovitis/Stiffness | 5% - 8% | Inadequate joint irrigation; retained bone debris; prolonged immobilization. | Aggressive hand therapy; intra-articular corticosteroid injection; rarely, arthroscopic synovectomy. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following an arthroscopic wafer procedure is vastly accelerated compared to an open ulnar shortening osteotomy, as there is no diaphyseal fracture requiring osseous union. However, a structured, phased approach is essential to optimize functional recovery and prevent stiffness.
Early Protective Phase (Weeks 0-2)
Immediately postoperatively, the patient is placed in a bulky soft dressing and a rigid volar wrist splint with the wrist in neutral. The primary goals during this phase are edema control, pain management, and protection of the surgical portals. Patients are strictly instructed to keep the extremity elevated above the heart. Immediate, active range of motion of the digits, elbow, and shoulder is initiated on postoperative day one to prevent composite stiffness and promote venous return. The splint remains in place continuously until the first postoperative visit at 10 to 14 days.
Strengthening and Return to Activity (Weeks 2-6+)
At the two-week mark, the sutures are removed. The rigid splint is transitioned to a removable, custom-molded thermoplastic wrist splint. The patient begins formal hand therapy. The initial focus is on restoring
