Ulnar Shortening Osteotomy: An Intraoperative Masterclass for Ulnocarpal Impaction Syndrome
Key Takeaway
This masterclass guides fellows through Ulnar Shortening Osteotomy for ulnocarpal impaction. We'll cover intricate surgical anatomy, meticulous preoperative planning, precise patient positioning, and a granular, step-by-step intraoperative execution. Learn critical techniques, avoid common pitfalls, and master postoperative management to achieve optimal patient outcomes in this complex wrist procedure.
Comprehensive Introduction and Patho-Epidemiology
Colleagues, let us delve into the precise, biomechanically profound procedure known as the ulnar shortening osteotomy (USO). This intervention is far more than a simple bone resection; it is a masterclass in restoring the delicate equilibrium of the wrist. We execute this procedure primarily to alleviate chronic compressive overloading at the ulnocarpal articulation—a pathologic state universally recognized as ulnocarpal impaction syndrome or ulnocarpal abutment. This condition is the direct result of static or dynamic ulnar-positive variance, which precipitates a cascade of degenerative changes leading to debilitating wrist pain, diminished grip strength, and profound functional impairment in our patients. Our surgical objective is twofold: to mechanically decompress the ulnocarpal joint and to simultaneously optimize the tension of the ulnocarpal and radioulnar marginal ligaments of the triangular fibrocartilage complex (TFCC), thereby restoring stability to the distal radioulnar joint (DRUJ).
To master this procedure, we must first possess a crystal-clear understanding of the underlying patho-epidemiology. Ulnar impaction syndrome fundamentally stems from an ulna that is relatively too long compared to the radius. This "ulnar-positive variance" can be a congenital anatomical variant, but in our clinics, we more frequently encounter the acquired forms. Consider the traumatic sequelae we see regularly: a malunited distal radius fracture with radial shortening, longitudinal radioulnar dissociation (such as an Essex-Lopresti injury), a Galeazzi fracture-dislocation, or premature closure of the distal radius physis secondary to trauma in a young athlete. Each of these scenarios disrupts the meticulously balanced length relationship between the radius and the ulna, shifting the biomechanical burden onto the ulnar side of the wrist.
The biomechanical consequences of this shift are staggering and well-documented in the seminal literature. The interosseous membrane, acting as a critical hinge for forearm rotation, normally facilitates the transmission of axial loads. In a wrist with neutral ulnar variance, the radius absorbs approximately 80% of the axial load, while the ulna transmits the remaining 20%. However, Palmer and Werner elegantly demonstrated that an ulnar-positive variance of merely 2.5 mm alters this dynamic catastrophically, increasing the load transmitted through the ulna to a staggering 42.7%. Conversely, a negative variance of 2.5 mm reduces the ulnar load to a mere 3.1%. This exponential increase in load directly impacts the TFCC, the lunate, and the triquetrum, accelerating mechanical wear and tear.
The natural history of untreated ulnocarpal impaction is characterized by an inevitable progression of degenerative changes, exacerbated by persistent heavy demand and repetitive loading across the positively variant joint. The Palmer classification of TFCC lesions provides an indispensable anatomical roadmap of these progressive degenerative changes (Class II lesions). The cascade begins with Type IIA (initial TFCC wear), progresses to Type IIB (TFCC wear combined with lunate or ulnar head chondromalacia), and advances to Type IIC (frank TFCC perforation). If left unchecked, the pathology extends to Type IID (involving lunotriquetral ligament perforation) and finally Type IIE (widespread ulnocarpal arthritis). Recognizing this predictable deterioration underscores the absolute necessity for timely, definitive surgical intervention when conservative measures have been exhausted.
Detailed Surgical Anatomy and Biomechanics
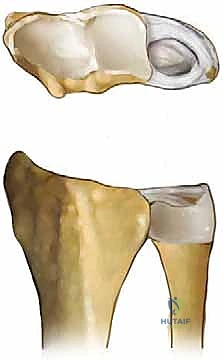
Before we make our incision, we must mentally map the complex surgical anatomy of the distal forearm and wrist. The interosseous membrane (IOM) is a structure of paramount importance. It is not merely a fascial sheet, but a highly complex, multi-layered ligamentous complex featuring a thickened central band. This central band spans obliquely from the proximal radius to the distal ulna, acting as a crucial longitudinal stabilizer and a hinge for forearm rotation. It is responsible for transmitting significant axial loads from the radius to the ulna. During an ulnar shortening osteotomy, altering the length of the ulna inherently alters the tension across the IOM, which plays a secondary role in stabilizing the DRUJ post-operatively.
Crucially for our surgical approach, we must meticulously respect the vascular anatomy of the ulnar diaphysis. The distal half of the ulna receives its primary endosteal and periosteal blood supply from small, segmental branches of the anterior and posterior interosseous arteries. These delicate vessels typically enter the ulna at intervals of 1 to 3 centimeters, originating from the direction of the interosseous membrane. During our surgical approach and subsequent periosteal elevation, these segmental vessels are highly vulnerable to iatrogenic injury. Meticulous dissection and strictly limited, careful subperiosteal elevation are absolutely essential to protect this blood supply. Compromising these vessels drastically increases the risk of delayed union or nonunion at the osteotomy site—the most dreaded complication of this procedure.
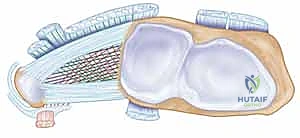
The Distal Radioulnar Joint (DRUJ) and its associated capsuloligamentous structures form the next critical anatomical tier. The DRUJ is an inherently unstable articulation, relying heavily on the extrinsic support of the TFCC. The TFCC is a complex structure comprising the articular disc, the dorsal and volar radioulnar ligaments, the meniscus homologue, the ulnocarpal ligaments (ulnolunate and ulnotriquetral), and the extensor carpi ulnaris (ECU) subsheath. The volar and dorsal radioulnar ligaments are the primary stabilizers of the DRUJ. Understanding the spatial orientation of these ligaments is vital, as the ulnar shortening osteotomy directly impacts their tension.
Biomechanically, the genius of the ulnar shortening osteotomy lies in its dual effect. By resecting a precise wafer of bone from the ulnar diaphysis, we not only physically decompress the ulnocarpal joint—relieving the direct abutment against the lunate and triquetrum—but we also generate a proximal translation of the distal ulnar segment. This proximal shift effectively tightens the ulnocarpal ligament complex and the stabilizing ligaments of the TFCC. This "ligamentotaxis" effect provides a powerful secondary benefit: it stabilizes a previously lax or subluxating DRUJ. Therefore, the USO is uniquely suited for patients who present with both ulnocarpal impaction and mild to moderate DRUJ instability, achieving two critical biomechanical goals through a single diaphyseal intervention.
Clinical Evaluation and Advanced Diagnostic Imaging
Our patient evaluation must be exhaustive, as ulnocarpal impaction syndrome often masquerades as other ulnar-sided wrist pathologies. A meticulous history is paramount. We must inquire about the onset of pain (acute traumatic vs. insidious repetitive motion), its exact characterization, and any associated mechanical symptoms such as clicking or crepitus. Pain is typically localized to the ulnar-sided wrist and is classically exacerbated by activities requiring power grip, forearm pronation, and ulnar deviation—maneuvers that dynamically increase ulnocarpal loading. We must also carefully document previous surgeries, particularly distal radius fracture fixations, and screen for any signs of ulnar nerve involvement, noting burning or tingling in the ring and small fingers.
The physical examination requires a systematic, provocative approach. With the elbow resting on the examination table and the hand pointing superiorly, we systematically palpate the anatomical structures. Tenderness localized over the distal ulna, the TFCC, or the ulnocarpal joint space is highly suggestive of impaction. We then proceed to specific provocative tests. The Piano Key Test assesses DRUJ stability; painful dorsal laxity of the distal ulna compared to the contralateral side suggests significant DRUJ incompetence. The Ulnar Compression Test, performed by applying axial load to the wrist in ulnar deviation, will reliably exacerbate pain and often elicit crepitus in the presence of ulnocarpal abutment or arthritis. Finally, the Lunotriquetral Ballottement (Reagan Shuck) Test is essential to evaluate for concomitant lunotriquetral interosseous ligament tears, a frequent passenger in advanced Palmer Type II lesions.
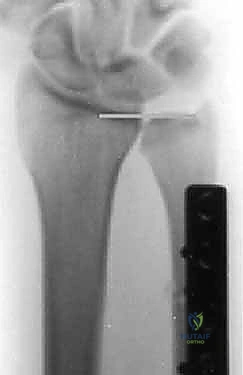
Imaging serves as our architectural blueprint for surgical planning. We mandate a comprehensive plain radiographic series. This begins with strictly neutral rotation posteroanterior (PA) and lateral views of both wrists to accurately assess static ulnar variance and the morphology of the sigmoid notch. However, static views are insufficient. We must obtain a pronated grip view (the clenched fist PA). As Tomaino and others have definitively demonstrated, active power grip forces the radius proximally relative to the ulna, increasing dynamic ulnar variance by an average of 2.5 mm. This view often unmasks profound dynamic impaction in wrists that appear neutrally variant on resting films.





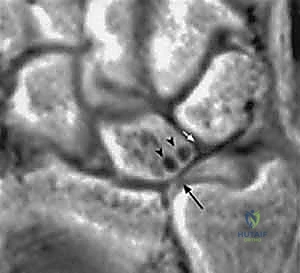
Advanced imaging and diagnostic modalities are frequently employed to refine our surgical strategy. High-resolution Magnetic Resonance Imaging (MRI), particularly when enhanced with intra-articular contrast (MR arthrography), is invaluable. It allows us to detect central TFCC perforations, evaluate the integrity of the intrinsic carpal ligaments (scapholunate and lunotriquetral), and identify early subchondral cystic changes or bone marrow edema in the proximal ulnar aspect of the lunate—the hallmark of advanced impaction. When diagnostic uncertainty persists, or when concomitant intra-articular pathology requires debridement, we utilize wrist arthroscopy. Arthroscopy remains the gold standard for directly visualizing chondral damage, assessing the trampoline effect of the TFCC, and confirming the precise Palmer classification prior to executing the extra-articular osteotomy.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of a successful ulnar shortening osteotomy. We do not operate on radiographic findings alone; we operate on symptomatic patients who have failed a rigorous trial of conservative management. The primary indication for this procedure is symptomatic ulnocarpal impaction syndrome—whether driven by static or dynamic ulnar-positive variance—that has proven refractory to rest, activity modification, NSAIDs, splinting, and targeted corticosteroid injections. A secondary, yet highly effective, indication is the presence of a central TFCC tear associated with positive ulnar variance, where shortening the ulna unloads the repair site and tightens the peripheral capsular structures to restore DRUJ stability.
We must also recognize the utility of USO in the management of mild, early-stage DRUJ osteoarthritis. In specific morphological variants of the sigmoid notch, shortening the ulna shifts the articular contact area proximally, moving the ulnar head away from the degenerated distal aspect of the sigmoid notch and into a more congruent, pristine articular surface. Furthermore, USO is indicated in cases of longitudinal radioulnar dissociation (such as chronic Essex-Lopresti injuries) where restoring the relative length of the forearm bones is critical to re-establishing the integrity of the interosseous membrane and the DRUJ.
However, we must be equally strict regarding our contraindications. The absolute contraindication to a diaphyseal ulnar shortening osteotomy is the presence of advanced, diffuse osteoarthritis of the DRUJ. If the entire sigmoid notch and ulnar head are denuded of cartilage, altering the length of the ulna will not alleviate pain; it may, in fact, exacerbate it by increasing joint contact pressures in a severely arthritic joint. In such cases, salvage procedures such as the Darrach resection, the Sauvé-Kapandji procedure, or ulnar head arthroplasty are required. Another absolute contraindication is an active, untreated infection in the surgical field.
Relative contraindications require careful clinical judgment and extensive patient counseling. Active smokers are at a profoundly elevated risk for delayed union and nonunion due to nicotine-induced microvascular vasoconstriction and impaired osteogenesis. We strongly advocate for smoking cessation protocols prior to elective osteotomy. Poorly controlled diabetes mellitus, chronic use of systemic corticosteroids, and severe osteoporosis also represent significant relative contraindications, as they compromise bone healing and hardware purchase. Finally, patient non-compliance is a major red flag; the post-operative rehabilitation protocol requires strict adherence to immobilization and activity restrictions to ensure successful union.
| Category | Specific Conditions |
|---|---|
| Primary Indications | Symptomatic ulnocarpal impaction (static or dynamic variance) refractory to conservative care; Central TFCC tears with positive variance; Early DRUJ instability secondary to positive variance. |
| Secondary Indications | Early/focal DRUJ osteoarthritis (unloading distal sigmoid notch); Longitudinal radioulnar dissociation (e.g., chronic Essex-Lopresti). |
| Absolute Contraindications | Advanced, diffuse DRUJ osteoarthritis; Active local or systemic infection; Incongruent DRUJ that subluxates upon shortening. |
| Relative Contraindications | Active tobacco use (high nonunion risk); Poorly controlled diabetes; Severe osteoporosis; Patient non-compliance or inability to adhere to rehab. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the difference between a masterfully executed surgery and an intraoperative struggle. The process begins with precise radiographic templating. Using calibrated PA and clenched fist radiographs, we calculate the exact millimeter resection required to achieve our goal: a neutral to slightly negative (-1 mm) ulnar variance. We must account for the thickness of the saw blade (kerf), which typically removes an additional 1 mm of bone. Over-shortening is a critical error; resecting more than 5 to 6 mm can drastically alter the kinematics of the DRUJ, potentially leading to impingement of the ulnar head against the proximal margin of the sigmoid notch.
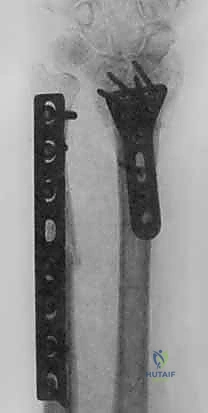
Hardware selection is the next critical step in our pre-operative workflow. Modern ulnar shortening is overwhelmingly performed using dedicated, precision osteotomy systems. These sets feature sophisticated sliding jigs that allow for highly controlled, parallel osteotomy cuts and built-in compression mechanisms. We generally prefer a 6-hole or 7-hole dynamic compression plate designed specifically for the ulnar diaphysis. The debate between a transverse versus an oblique osteotomy heavily favors the oblique cut (typically angled at 45 degrees). The oblique osteotomy vastly increases the surface area for bone healing, allows for the placement of an interfragmentary lag screw through the plate, and provides superior rotational control during compression.



Anesthesia and tourniquet management are standardized to optimize the surgical field and patient comfort. We strongly advocate for regional anesthesia—specifically, a supraclavicular or axillary brachial plexus block—combined with light general anesthesia or deep intravenous sedation. The regional block provides excellent intraoperative muscle relaxation and profound post-operative analgesia, significantly reducing the need for systemic opioids. A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mmHg following exsanguination with an Esmarch bandage, ensuring a bloodless field for meticulous dissection.
Patient positioning must facilitate unrestricted access to the ulnar aspect of the forearm and seamless integration of intraoperative fluoroscopy. The patient is positioned supine with the operative extremity extended on a radiolucent hand table. The shoulder is abducted to 90 degrees, and the elbow is slightly flexed. We position the C-arm fluoroscopy unit either coming in from the foot of the table or parallel to the arm board, ensuring that we can easily obtain true PA and lateral views of the wrist and forearm without compromising the sterile field. A sterile bump is often placed under the wrist to facilitate neutral positioning during plate application.
Step-by-Step Surgical Approach and Fixation Technique
We begin with a longitudinal incision over the distal and middle thirds of the ulnar diaphysis. While a dorsal approach is described, we strongly prefer the volar-ulnar approach. The incision is placed directly over the palpable subcutaneous border of the ulna, typically extending 8 to 10 centimeters. We carefully deepen the incision through the subcutaneous tissues, remaining acutely vigilant for the dorsal sensory branch of the ulnar nerve (DSBUN). This critical nerve typically crosses the operative field from volar to dorsal approximately 5 to 8 centimeters proximal to the ulnar styloid. It must be meticulously identified, mobilized, and protected with vessel loops throughout the procedure to prevent painful post-operative neuromas.
The deep fascial interval is developed between the flexor carpi ulnaris (FCU) volarly and the extensor carpi ulnaris (ECU) dorsally. We elevate the FCU muscle belly and retract it volarly, exposing the palmar and ulnar aspects of the ulnar diaphysis. Here, surgical discipline is paramount: periosteal elevation must be strictly limited to the footprint of the plate. We use a sharp elevator to clear only the necessary bone, preserving the dorsal and interosseous soft tissue attachments. This rigorous adherence to minimal periosteal stripping is the primary defense against devascularizing the bone and precipitating a nonunion.



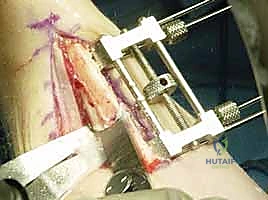
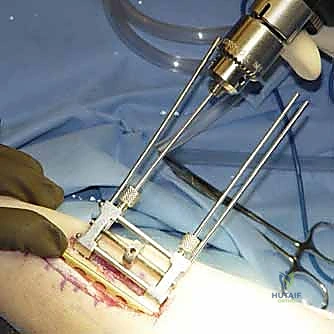
With the diaphysis exposed, we apply the dedicated cutting jig. The jig is temporarily fixed to the bone using bicortical screws. We utilize a sharp, cooled oscillating saw to execute the osteotomy. Copious cold saline irrigation is non-negotiable during the cutting phase to prevent thermal necrosis of the bone ends, which is a major contributor to nonunion. We make the proximal cut first, followed by the distal cut, removing the precisely templated wafer of bone. The oblique nature of the cut (usually 45 degrees) allows the bone ends to slide seamlessly together without rotational malalignment.


Following the resection, the compression device integrated into the jig is activated. We slowly and deliberately compress the osteotomy site until
Clinical & Radiographic Imaging Archive




