Mastering Perilunate & Lunate Dislocation Repair: An Intraoperative Guide to Greater and Lesser Arc Injuries
Key Takeaway
This masterclass guides orthopaedic fellows through the operative management of complex perilunate and lunate dislocations, encompassing both lesser and greater arc injuries. We meticulously detail surgical anatomy, preoperative planning, a combined dorsal and volar approach, precise reduction techniques, ligament repair, and fracture fixation. Emphasis is placed on real-time intraoperative decision-making, complication avoidance, and comprehensive postoperative care for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater, colleagues. Today, we are undertaking the surgical management of a profoundly challenging and frequently devastating wrist injury: perilunate and lunate dislocations. These injuries represent the extreme end of the spectrum of carpal instability, specifically focusing on the complex continuum of lesser and greater arc injuries. It is imperative to understand that these are not mere "wrist sprains" or simple ligamentous tweaks; they represent catastrophic disruptions to carpal kinematics, global wrist stability, and the fundamental biomechanics of the upper extremity. Such injuries demand meticulous attention to detail, a profound understanding of three-dimensional anatomy, and precise, unyielding surgical intervention.
Nonoperative management of these injuries, as the literature has definitively proven, yields predictably poor and unacceptable results. Attempting to treat a perilunate dislocation with closed reduction and casting invariably leads to recurrent instability, chronic debilitating pain, severe deformity, and rapid, progressive radiocarpal and midcarpal degenerative changes. Our singular goal in the operating room today is to achieve a rigid, anatomical reduction of all carpal elements and secure stable fixation to restore normal carpal mechanics, thereby preventing the long-term sequelae of post-traumatic arthritis and carpal collapse.
These injuries typically result from high-energy mechanisms, most classically an extreme axial load applied to a hyperextended, ulnarly deviated, and intercarpally supinated wrist. This violent mechanism places the strong volar ligamentous structures under immense tension while simultaneously subjecting the dorsal structures to severe compression and shear forces. The kinetic energy dissipates through the carpus in a highly predictable radial-to-ulnar direction, creating a cascade of structural failures. The distinction between lesser and greater arc injuries dictates our specific operative strategy, but both mandate a comprehensive reconstruction.
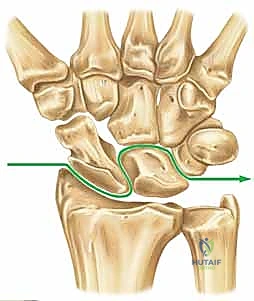
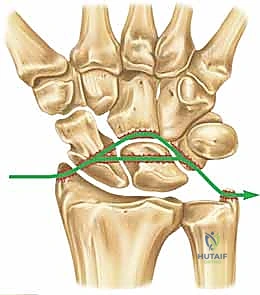
Lesser arc injuries are purely capsuloligamentous and progress through four sequential stages, originally described in the landmark biomechanical studies by Mayfield, Johnson, and Kilcoyne. Stage I involves the disruption of the critical scapholunate (SL) ligament complex. Stage II sees the energy wave propagate through the space of Poirier, disrupting the volar capsule. Stage III involves the failure of the lunotriquetral (LT) interosseous ligament and the ulnotriquetrocapitate complex, allowing the capitate to dislocate dorsally. Finally, Stage IV culminates in the complete volar extrusion of the lunate into the carpal tunnel.
Conversely, greater arc injuries follow a similar pathophysiological progression but involve associated osseous failures—carpal fractures that propagate through the radial styloid, scaphoid, capitate, or triquetrum. The transscaphoid perilunate fracture-dislocation is the most common variant of the greater arc injury. Recognizing whether you are dealing with a purely ligamentous lesser arc injury or a fracture-variant greater arc injury is the foundational step in preoperative templating and intraoperative execution.
Detailed Surgical Anatomy and Biomechanics
Before we even contemplate our initial incision, we must mentally reconstruct the intricate, unforgiving anatomy of the carpus. The human wrist is a biomechanical marvel, functioning as a complex, intercalated system of dual rows that allows highly coordinated, paired motion within both the radial–ulnar deviation and flexion–extension planes. The eight carpal bones are entirely devoid of tendinous insertions; they act as a passive intercalated segment. Their motion is entirely dependent upon and guided by a precise, unyielding ligamentous architecture and complex bony geometry.
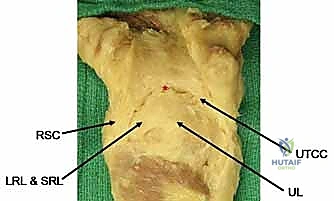
The stability of the carpus relies heavily on its ligamentous structures, which we broadly categorize into extrinsic and intrinsic ligaments. The volar extrinsic ligaments are the prime stabilizers of the wrist, arranged in a robust double-V configuration. This specific anatomical arrangement creates a region of relative capsular weakness between the apices of the V's, famously known as the space of Poirier. The inner-V ligaments include the long radiolunate (LRL), radioscapholunate (RSL)—which is more of a neurovascular conduit than a true mechanical stabilizer—the short radiolunate (SRL), and the ulnolunate (UL) ligaments. The outer-V consists of the radioscaphocapitate (RSC) and the ulnotriquetrocapitate complex (UTCC). It is through the space of Poirier that the lunate typically herniates during a Stage IV Mayfield dislocation.
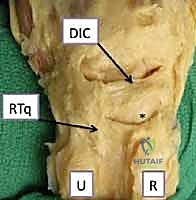
The dorsal extrinsic ligaments, while providing less absolute structural stability compared to their massive volar counterparts, are nonetheless crucial for preventing dorsal intercalated segment instability (DISI) and guiding normal carpal tracking. The primary dorsal stabilizers are the radiotriquetral (RT) ligament, also known as the dorsal radiocarpal ligament, and the dorsal intercarpal (DIC) ligament. Together, these form a dorsal V-shaped stabilizing complex. During our surgical approach, meticulous preservation and subsequent repair of these dorsal structures are mandatory to prevent post-operative subluxation of the carpus.
Equally critical are the intrinsic ligaments, the direct intercarpal connections that provide intra-row stability and maintain the proximal row as a cohesive functional unit. The scapholunate (SL) interosseous ligament is the primary stabilizer of the scaphoid-lunate articulation, composed of dorsal, proximal, and volar regions, with the dorsal region being the thickest and most biomechanically significant. The lunotriquetral (LT) interosseous ligament maintains the lunate-triquetrum relationship, with its volar portion being the most robust. Disruption of these intrinsic ligaments is the hallmark of perilunate instability, and their anatomical repair is the cornerstone of our surgical reconstruction.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention in the setting of perilunate and lunate dislocations is rarely ambiguous. Surgical management is the absolute standard of care for nearly all acute presentations of these injuries. The indications are driven by the necessity to restore carpal anatomy, decompress vital neurovascular structures, and establish a stable biomechanical environment conducive to ligamentous healing.
Acute perilunate and lunate dislocations constitute an absolute indication for urgent surgical intervention, particularly when accompanied by signs of median neuropathy. The volar displacement of the lunate into the rigid confines of the carpal tunnel frequently results in acute, severe compression of the median nerve. In such scenarios, delayed intervention is unacceptable, as it rapidly leads to irreversible axonal damage and profound functional deficits. Even in the absence of acute nerve compression, the profound instability of the carpus necessitates open reduction, internal fixation, and primary ligamentous repair to prevent the inevitable progression to advanced carpal collapse.
Relative indications for specific surgical approaches depend on the chronicity of the injury and the presence of associated fractures. While acute injuries (less than 4 weeks old) are highly amenable to primary repair, chronic or neglected dislocations (presenting months after the initial trauma) present a significantly more complex challenge. In chronic cases, severe soft tissue contractures, bone resorption, and early chondral damage may preclude anatomical reduction, pushing the surgeon toward salvage procedures such as proximal row carpectomy (PRC) or partial wrist arthrodesis.
| Indication / Contraindication Category | Specific Clinical Scenarios | Rationale / Management Strategy |
|---|---|---|
| Absolute Surgical Indications | Acute lunate/perilunate dislocation, Acute carpal tunnel syndrome, Open fracture-dislocations. | Urgent decompression of the median nerve; prevention of irreversible cartilage damage; restoration of biomechanical stability. |
| Relative Surgical Indications | Delayed presentation (4-8 weeks), Polytrauma patient with higher priority life-saving needs. | Attempt primary repair if cartilage is viable and reduction is possible; otherwise, prepare for salvage procedures. |
| Absolute Contraindications | Medically unstable patient (e.g., severe hemodynamic compromise), Active life-threatening systemic infection. | Life over limb; initial management limited to splinting and closed reduction attempts until patient is stable for anesthesia. |
| Relative Contraindications | Severe pre-existing radiocarpal arthritis, Low-demand elderly patient with severe medical comorbidities. | Consider non-operative management or primary salvage procedures (e.g., total wrist fusion) to minimize surgical morbidity. |
Contraindications to comprehensive open reduction and internal fixation are exceedingly rare and are generally limited to patients who are medically unfit for prolonged anesthesia or those with devastating, life-threatening polytrauma that precludes immediate orthopedic reconstruction. In such extreme cases, a temporizing closed reduction and percutaneous pinning may be attempted, though this is strictly a damage-control measure, not a definitive solution.
Pre-Operative Planning, Templating, and Patient Positioning
Effective surgical management of complex carpal trauma begins long before the first incision is made. A rigorous, systematic approach to preoperative planning is the blueprint for intraoperative success. A typical history involves a high-energy trauma—a fall from a height, a motor vehicle collision, or a severe athletic injury. Patients present with profound pain, diffuse swelling, gross deformity, and an absolute inability to range the wrist.
The physical examination must be exhaustive, with a critical focus on the neurologic assessment. Median neuropathy is exceedingly common, ranging from mild dysesthesia in the radial three-and-a-half digits to overt motor dysfunction of the thenar musculature. The presence of acute carpal tunnel syndrome in this scenario elevates the injury to a true surgical emergency. Palpation of the carpus, while limited by swelling, may reveal specific point tenderness indicative of associated greater arc fractures.


Our primary diagnostic tools are high-quality, orthogonal radiographs. True posteroanterior (PA) and lateral views are paramount. On the PA view of a perilunate dislocation, we meticulously evaluate the disruption of Gilula's three carpal arcs. The lunate, normally trapezoidal, assumes a triangular or "piece of pie" shape due to its abnormal rotation. On the lateral view, the crucial concentricity of the distal radius, lunate, and capitate is lost, clearly demonstrating the dorsal dislocation of the capitate out of the lunate fossa.

In the case of a complete Stage IV lunate dislocation, the PA radiograph again shows the disruption of Gilula's lines, but the lateral radiograph reveals the classic "spilled teacup" sign. The lunate is volarly displaced, severely flexed, and lies entirely anterior to the volar cortex of the distal radius, while the capitate drops proximally to articulate directly with the radial articular surface. Advanced imaging, such as CT scanning, is highly recommended in greater arc injuries to precisely define the fracture geometry of the scaphoid or capitate, aiding in screw trajectory planning.
Patient positioning is critical for a seamless operation. The patient is placed in the supine position with the operative arm extended on a radiolucent hand table. This radiolucency is non-negotiable; it allows for unhindered intraoperative fluoroscopy without the need to awkwardly manipulate the injured extremity. A well-padded pneumatic tourniquet is applied to the proximal arm. The C-arm must be sterilely draped and positioned parallel to the table, allowing the surgeon to obtain true PA and lateral views instantly.
Step-by-Step Surgical Approach and Fixation Technique
We utilize a combined dorsal and volar approach. This dual-incision technique is the gold standard, as it is the only method that affords comprehensive visualization of the entire pathology, allows for complete decompression of the median nerve, and provides the necessary access for anatomic reduction and repair of both the volar and dorsal ligamentous structures.

The Dorsal Approach:
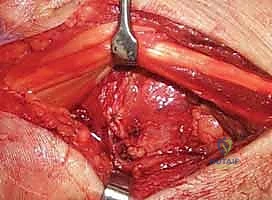
We begin with a universal dorsal skin incision, a longitudinal or slightly curvilinear incision extending from the distal radius, just ulnar to Lister's tubercle, distally towards the base of the third metacarpal. We meticulously raise full-thickness medial and lateral skin flaps to preserve the subdermal vascular plexus and protect the dorsal sensory branches of the radial and ulnar nerves.
We identify the extensor retinaculum and open the third extensor compartment, mobilizing and transposing the extensor pollicis longus (EPL) tendon radially. Next, we subperiosteally elevate the fourth extensor compartment (extensor digitorum communis and extensor indicis proprius) ulnarly. This exposes the dorsal radiocarpal joint capsule. We perform a ligament-sparing capsulotomy, typically a Berger flap (a radially based, inverted-V capsulotomy) that preserves the integrity of the dorsal intercarpal and radiotriquetral ligaments.

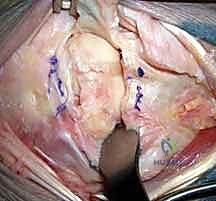
Upon entering the joint dorsally, the magnitude of the injury becomes apparent. The midcarpal joint is grossly unstable, and in a perilunate dislocation, the capitate rests dorsal to the lunate. We irrigate the joint copiously to remove hematoma and osteochondral debris. We inspect the proximal articular surfaces of the scaphoid, lunate, and triquetrum, assessing the status of the SL and LT interosseous ligaments.

The Volar Approach:
Leaving the dorsal wound packed with a moist sponge, we supinate the forearm and execute an extended carpal tunnel incision. This incision crosses the wrist crease in a zig-zag fashion to prevent scar contracture and extends distally into the palm. We divide the transverse carpal ligament comprehensively, immediately decompressing the median nerve. The nerve is carefully retracted radially with a vessel loop.

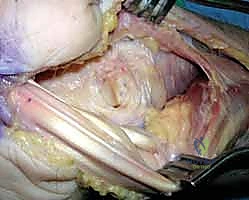
Deep to the flexor tendons, which are retracted ulnarly, we identify the massive rent in the volar capsule through the space of Poirier. In a true lunate dislocation, the lunate will be found sitting entirely within this space, impinging on the flexor tendons and median nerve. We must carefully mobilize the lunate, ensuring we do not tether its remaining fragile volar blood supply (via the short radiolunate ligament).

Reduction and Fixation:
With both approaches open, we proceed with reduction. This is a coordinated bimanual maneuver. Through the volar approach, the surgeon applies direct pressure to the volar pole of the lunate, pushing it dorsally and distally back into the lunate fossa of the radius. Simultaneously, through the dorsal approach, longitudinal traction is applied to the hand, and the capitate is levered volarly over the dorsal lip of the lunate to restore the normal colinear relationship of the radius, lunate, and capitate.

Once provisional reduction is achieved, we utilize 0.062-inch or 0.045-inch Kirschner wires as "joysticks" placed into the scaphoid and lunate dorsally. These joysticks allow us to manipulate the carpal bones, correcting the classic flexed posture of the scaphoid and the extended posture of the lunate, closing the scapholunate gap.

Under strict fluoroscopic guidance, we pin the carpus to maintain this anatomical reduction. The standard pinning sequence involves driving K-wires from the scaphoid into the lunate, the scaphoid into the capitate, and the triquetrum into the lunate. If a transscaphoid fracture is present (greater arc), we prioritize rigid internal fixation of the scaphoid utilizing a headless compression screw, inserted via either a dorsal or volar approach depending on the fracture location, before completing the intercarpal pinning.

Ligamentous Repair:
With the bony architecture stabilized, we turn our attention to the soft tissues. Dorsally, the avulsed remnants of the scapholunate interosseous ligament are meticulously repaired. We utilize micro-suture anchors (typically 1.5mm to 2.0mm) placed into the dorsal rim of the scaphoid or lunate, depending on the side of the avulsion, passing non-absorbable sutures through the ligamentous stump.
We repeat this process for the lunotriquetral ligament if it is amenable to repair. Volarly, the massive rent in the space of Poirier must be closed. We reapproximate the stout volar extrinsic ligaments using heavy, slow-absorbing or non-absorbable sutures, ensuring a watertight closure of the volar capsule to prevent recurrent volar subluxation of the lunate.
Finally, the dorsal capsular flap (Berger flap) is repaired anatomically. The extensor retinaculum is closed, leaving the EPL transposed subcutaneously to prevent attrition rupture against the dorsal hardware. The wounds are closed in layers, and the limb is placed in a well-padded, bulky short-arm thumb-spica splint.
Complications, Incidence Rates, and Salvage Management
Despite flawless surgical execution, perilunate and lunate dislocations are fraught with high rates of complications due to the sheer violence of the initial trauma. The surgeon must be intimately aware of these potential pitfalls, counsel the patient extensively preoperatively, and be prepared to execute salvage procedures when primary reconstructions fail or degenerate.
The most immediate and concerning complication is persistent median neuropathy. While acute carpal tunnel release typically resolves the compression, severe initial contusion or traction injury to the nerve can result in permanent dysesthesia or motor weakness. Furthermore, the precarious blood supply of the proximal carpal row, particularly the scaphoid and lunate, renders them highly susceptible to avascular necrosis (AVN). Transient ischemia of the lunate is common, but true, progressive Kienböck's-like collapse or scaphoid proximal pole AVN occurs in a notable percentage of cases, necessitating later vascularized bone grafting or salvage procedures.
The most insidious long-term complication is the development of post-traumatic osteoarthritis, specifically Scapholunate Advanced Collapse (SLAC) or Scaphoid Nonunion Advanced Collapse (SNAC). Even with anatomical reduction, the severe chondral impact at the time of injury often leads to progressive joint space narrowing, particularly at the radioscaphoid and midcarpal articulations. Loss of reduction, pin breakage, or failure of ligament healing inevitably accelerates this degenerative cascade.
| Complication | Estimated Incidence | Pathophysiology & Management Strategy |
|---|---|---|
| Median Neuropathy | 20% - 40% | Contusion/compression from volar lunate. Management: Immediate surgical decompression (carpal tunnel release). |
| Post-Traumatic Arthritis (SLAC/SNAC) | 30% - 60% (Long-term) | Cartilage damage at impact; subtle loss of reduction. Management: Proximal Row Carpectomy (PRC) or 4-Corner Fusion. |
| Avascular Necrosis (Lunate/Scaphoid) | 10% - 20% | Disruption of intraosseous/capsular blood supply. Management: Vascularized bone graft, core decompression, or salvage fusion. |
| Carpal Stiffness / Loss of ROM | > 80% | Capsular scarring, prolonged immobilization. Management: Aggressive hand therapy, dynamic splinting, rare arthroscopic capsular release. |
| Hardware Failure / Loss of Reduction | 5% - 15% | Premature pin removal, non-compliance, poor bone quality. Management: Revision pinning, progression to salvage arthrodesis if ligaments fail to heal. |
When primary repair fails and the patient develops debilitating, painful arthritis, salvage procedures become the definitive treatment. Proximal row carpectomy (PRC) involves the excision of the scaphoid, lunate, and triquetrum, allowing the capitate to articulate with the lunate fossa of the radius. Alternatively, a scaphoid excision and four-corner fusion (capitate, hamate, lunate, triquetrum) provide a stable, pain-free wrist while preserving roughly 50% of normal flexion-extension arc. In the most severe cases of pan-carpal arthritis, a total wrist arthrodesis is the final, definitive solution.
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation following a perilunate reconstruction is a delicate balance between protecting the fragile ligamentous repairs and preventing profound, debilitating carpal stiffness. The protocol must be strictly phased, highly supervised by a specialized certified hand therapist (CHT), and tailored to the specific intraoperative findings and the rigidity of the fixation.
Phase I: Absolute Immobilization (Weeks 0-4)
Immediately post-operatively, the patient is placed in a bulky, rigid thumb-spica splint. At the first post-operative visit (7-10 days), sutures are removed, and the patient is transitioned into a rigid, custom-molded short-arm thumb-spica cast. During this phase, absolute immobilization of the wrist and thumb base is mandatory. However, aggressive, active range of motion of the fingers, elbow, and shoulder is initiated immediately to prevent tendon adhesions and proximal joint stiffness. Edema control is paramount.
**Phase II: Pin Removal and Protected Motion (Weeks 8
