Mastering the Diagnosis and Management of Wrist Conditions
Key Takeaway
Diagnosing wrist conditions requires a profound understanding of carpal kinematics, precise clinical examination, and a structured imaging algorithm. This guide covers Taleisnik’s columnar theory, Lichtman’s ring concept, and Mayfield’s stages of perilunar instability. It provides orthopaedic surgeons with an evidence-based framework for evaluating wrist trauma, differentiating soft tissue from osseous pathology, and executing appropriate surgical interventions for carpal instability.
Comprehensive Introduction and Patho-Epidemiology
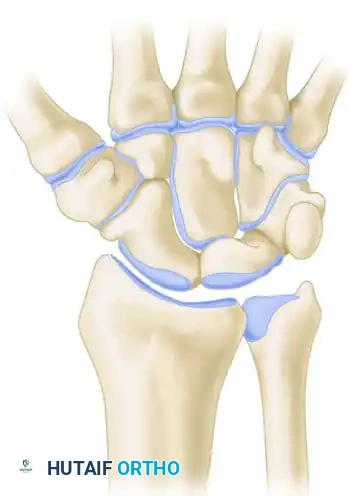
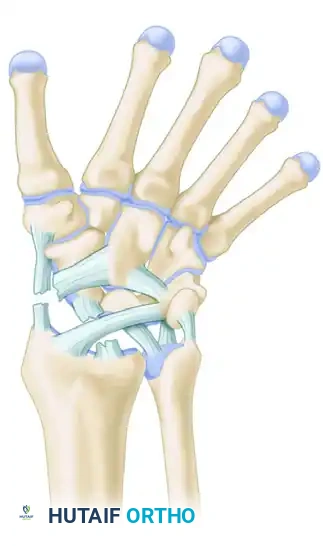
The human wrist is an intricate biomechanical marvel, comprising eight carpal bones, multiple articulating surfaces, and a complex network of intrinsic and extrinsic ligaments. The diagnosis of wrist conditions—whether acute traumatic injuries or chronic degenerative pathologies—demands a meticulous, systematic approach. For the orthopaedic surgeon, mastering the diagnostic algorithm is paramount to preventing long-term sequelae such as carpal collapse, chronic instability, and post-traumatic osteoarthritis, most notably Scapholunate Advanced Collapse (SLAC) or Scaphoid Nonunion Advanced Collapse (SNAC).
Epidemiologically, wrist injuries represent a significant proportion of musculoskeletal trauma presenting to emergency departments and orthopaedic clinics. Distal radius fractures alone account for approximately one-sixth of all fractures treated in emergency settings, while scaphoid fractures constitute nearly 70% of all carpal fractures. Ligamentous injuries, particularly scapholunate (SL) dissociations, are frequently missed during initial evaluations, leading to a high incidence of delayed presentations. The socioeconomic impact of these injuries is profound, often affecting young, working-age individuals and resulting in substantial lost wages, prolonged rehabilitation, and complex medicolegal or workers' compensation claims.
Understanding the patho-epidemiology requires an appreciation of the continuous spectrum of tissue failure. The severity and specific pattern of injury depend on four critical variables: the magnitude and vector of the applied force in three dimensions; the duration and amplitude of forces; the hand position at impact (degree of extension, ulnar/radial deviation, and intercarpal supination); and inherent patient-specific ligamentous laxity. High-energy, rapid-loading events such as motor vehicle collisions produce vastly different failure patterns than low-energy, sustained loads or repetitive microtrauma.
A precise clinical history remains the cornerstone of accurate diagnosis. The clinician must document standard demographic data, including age, hand dominance, occupation, and hobbies, as these factors directly dictate surgical decision-making and postoperative rehabilitation goals. Furthermore, inquiring about modifying factors, previous wrist injuries, and the presence of underlying systemic inflammatory arthropathies is essential for stratifying risk and managing patient expectations before embarking on complex carpal reconstructive procedures.
Detailed Surgical Anatomy and Biomechanics
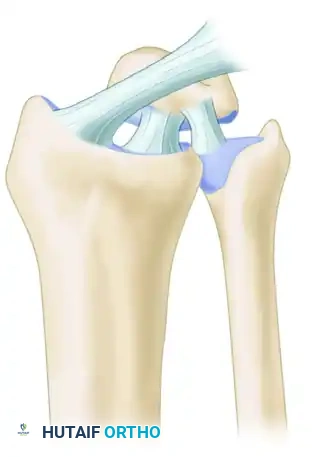
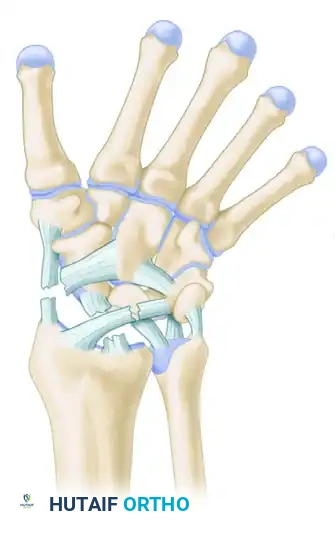
To accurately diagnose and manage wrist instability, the surgeon must possess a profound understanding of carpal kinematics and the stabilizing ligamentous structures. The carpus is devoid of direct tendinous insertions, relying entirely on its articular geometry and a robust capsuloligamentous network for stability under compressive loads. Two primary biomechanical models dominate contemporary orthopaedic thought: Taleisnik’s Columnar Concept and Lichtman’s Ring Concept.
Taleisnik’s Columnar Concept
Taleisnik proposed that the wrist functions via three distinct longitudinal columns. The Central (Flexion-Extension) Column comprises the entire distal carpal row (trapezium, trapezoid, capitate, hamate) and the lunate. This column is primarily responsible for the transmission of flexion and extension forces from the hand to the forearm. The Lateral (Mobile) Column consists solely of the scaphoid, which bridges the proximal and distal rows, providing critical stability and mobility. The Medial (Rotary) Column comprises the triquetrum, functioning as a pivot point for carpal rotation.


Lichtman’s Ring Concept and Intercalated Segmental Instability
Lichtman expanded upon carpal kinematics by describing the carpus as an oval ring. In this model, the proximal and distal carpal rows act as semirigid posts stabilized by robust interosseous ligaments. Normal, controlled mobility occurs primarily at the scaphotrapezial and triquetrohamate joints. Any break in this ring—whether osseous (e.g., scaphoid fracture) or ligamentous (e.g., scapholunate dissociation)—destabilizes the kinematic chain.
Depending on the location of the break, the lunate will fall into an abnormal posture. If the scapholunate ligament fails, the scaphoid flexes while the lunate and triquetrum extend, producing a Dorsal Intercalated Segmental Instability (DISI) deformity. Conversely, if the lunotriquetral ligament fails, the lunate flexes with the scaphoid while the triquetrum extends, resulting in a Volar Intercalated Segmental Instability (VISI) deformity.
The Spectrum of Perilunar Instability (Mayfield Stages)
Mayfield, Johnson, and Kilcoyne classically described the progressive stages of perilunar instability resulting from wrist hyperextension, ulnar deviation, and intercarpal supination. This sequential failure occurs in four distinct stages around the lunate, representing a continuum of catastrophic ligamentous disruption.
Stage I: Scapholunate Dissociation
The injury initiates radially with the disruption of the scapholunate (SL) interosseous ligament and the volar radioscaphocapitate ligament. This results in rotatory subluxation of the scaphoid and the classic "Terry Thomas" sign on AP radiographs.
Stage II: Capitolunate Disruption
As the force propagates ulnarly, the space of Poirier (an inherently weak area in the volar capsule between the capitate and lunate) is breached. The capitate subluxates dorsally relative to the lunate, disrupting the midcarpal joint.
Stage III: Lunotriquetral Disruption (Perilunate Dislocation)
The force continues through the lunotriquetral (LT) interosseous ligament. The entire carpus dislocates dorsally, leaving only the lunate articulated with the distal radius within the lunate fossa.
Stage IV: Lunate Dislocation
The final stage involves the failure of the dorsal radiocarpal ligament. The capitate is driven proximally, forcing the lunate to rotate and dislocate volarly into the carpal tunnel. This frequently causes acute median nerve compression, representing an orthopaedic emergency that requires immediate reduction to prevent irreversible neuropathy and lunate avascular necrosis.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention in wrist pathology hinges on a delicate balance between patient functional demands, the chronicity of the injury, and the presence of degenerative articular changes. Acute instability patterns and displaced intra-articular fractures almost universally mandate surgical fixation to restore anatomic alignment and kinematic function. Conversely, chronic conditions with established osteoarthritis require salvage procedures designed to eliminate pain at the expense of motion.
Absolute indications for emergent or urgent surgical intervention include acute perilunate or lunate dislocations (Mayfield Stages II-IV), open carpal fractures, and acute carpal tunnel syndrome secondary to trauma. Relative indications encompass acute scapholunate or lunotriquetral ligament ruptures with demonstrable dynamic or static instability, displaced scaphoid fractures, and symptomatic nonunions. In the realm of chronic degenerative conditions, procedures such as Proximal Row Carpectomy (PRC) or Four-Corner Arthrodesis (4CA) are indicated for advanced SLAC or SNAC wrists where conservative measures (e.g., splinting, NSAIDs, corticosteroid injections) have been exhausted.
Contraindications must be meticulously evaluated. Absolute contraindications include active deep infection, medically unstable patients who cannot tolerate anesthesia, and severe generalized complex regional pain syndrome (CRPS) in the affected extremity. Relative contraindications often revolve around patient compliance; a patient unwilling or unable to adhere to strict postoperative immobilization and phased rehabilitation protocols is a poor candidate for complex ligamentous reconstructions. Furthermore, performing a PRC in a patient with capitate head arthritis is strictly contraindicated, as the procedure relies on a pristine capitate-lunate fossa articulation.
| Pathology / Condition | Primary Surgical Indication | Contraindications & Alternative Management |
|---|---|---|
| Acute Perilunate Dislocation | Mayfield Stage II-IV; Acute median neuropathy; Inability to maintain closed reduction. | Contra: Medically unstable. Alt: Immediate closed reduction and splinting until stable for surgery. |
| Acute Scapholunate Tear | Widened SL interval (>3mm); Positive Watson shift test; Acute trauma (< 4-6 weeks). | Contra: Pre-existing SLAC arthritis. Alt: Conservative casting (rarely effective for complete tears); Salvage procedures if chronic. |
| Scaphoid Nonunion | Persistent fracture gap > 6 months; Cystic changes; SNAC progression. | Contra: SNAC Stage III (radioscaphoid and midcarpal arthritis). Alt: Vascularized bone grafting for AVN; 4-corner fusion for advanced SNAC. |
| SLAC Wrist (Stage II) | Radioscaphoid arthritis with preserved midcarpal joint; Intractable pain. | Contra: Capitate head arthritis (for PRC). Alt: Proximal Row Carpectomy (PRC) or Four-Corner Arthrodesis. |
| Kienböck's Disease (Stage II/IIIa) | Lunate sclerosis/collapse with negative ulnar variance. | Contra: Advanced carpal collapse with secondary arthritis. Alt: Joint leveling procedures (radial shortening osteotomy); Revascularization. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the bedrock of successful wrist surgery. The radiographic evaluation follows a strict, stepwise algorithm to ensure no subtle instability or occult fracture is missed. The initial evaluation must always include four standard views: Posteroanterior (PA), Lateral, Oblique, and a specialized Scaphoid view. The PA view is scrutinized for disruptions in Gilula's carpal arcs, ulnar variance, and joint space narrowing. The lateral view is critical for evaluating carpal alignment—specifically the collinear relationship of the radius, lunate, and capitate—and for measuring the scapholunate angle (normal 30°-60°) and capitolunate angle (normal <15°).
If routine radiographs are normal but clinical suspicion remains high (e.g., persistent dorsal radial wrist pain, positive Watson scaphoid shift test), advanced imaging is mandated. Dynamic fluoroscopy, including clenched fist and radial/ulnar deviation views, can unmask dynamic instability. Computed Tomography (CT) is the gold standard for evaluating osseous anatomy, assessing fracture union, and templating for intra-articular step-offs. Magnetic Resonance Imaging (MRI), particularly high-resolution 3T MRI or MR Arthrography, is highly sensitive for occult fractures, avascular necrosis (Kienböck's or Preiser's disease), and intrinsic ligament or Triangular Fibrocartilage Complex (TFCC) tears.
Templating and Surgical Setup
Preoperative templating involves overlaying digital templates on scaled radiographs to determine the appropriate size of implants, such as headless compression screws for scaphoid fractures or circular plates for four-corner fusions. Anticipating the need for bone graft—whether local distal radius autograft, iliac crest autograft, or allograft—must be established prior to the incision.
Patient positioning is standardized but requires fastidious attention to detail. The patient is placed supine with the operative extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm, typically inflated to 250 mmHg after exsanguination with an Esmarch bandage. The use of regional anesthesia, such as a supraclavicular or axillary brachial plexus block, is highly recommended as it provides excellent intraoperative muscle relaxation and superior postoperative analgesia. A mini-C-arm fluoroscopy unit must be positioned perpendicular to the hand table, allowing the surgeon to seamlessly transition between AP, lateral, and oblique dynamic views without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
Surgical intervention in the wrist requires meticulous soft tissue handling and precise anatomic restoration. The choice of approach—dorsal, volar, or combined—is dictated by the specific pathology.
The Dorsal Approach to the Wrist
The dorsal approach provides unparalleled exposure to the proximal carpal row, midcarpal joint, and the dorsal aspect of the distal radius. It is the workhorse approach for SL ligament repairs, proximal row carpectomies, and dorsal perilunate reductions.
1. Incision and Dissection: A longitudinal incision is made centered over Lister’s tubercle, extending from the distal third of the radius to the base of the third metacarpal. Full-thickness skin flaps are elevated to protect the sensory branches of the radial and ulnar nerves.
2. Retinacular Management: The extensor retinaculum is exposed. The third extensor compartment is opened longitudinally, and the Extensor Pollicis Longus (EPL) tendon is transposed radially. The second and fourth compartments are elevated subperiosteally from the distal radius, preserving their gliding layers to prevent postoperative tendon adhesions.
3. Capsulotomy: A ligament-sparing capsulotomy is critical to prevent iatrogenic instability. The Berger dorsal intercarpal ligament-splitting approach creates a radially based, V-shaped flap that preserves the dorsal radiocarpal and dorsal intercarpal ligaments.
4. Intervention (e.g., SL Ligament Repair): The midcarpal and radiocarpal joints are inspected. For an acute SL tear, the joint is debrided of hematoma. The scaphoid and lunate are anatomically reduced using 0.045-inch or 0.062-inch K-wires as joysticks. Once the SL interval is closed and the DISI deformity corrected, the bones are pinned together (scaphoid-lunate and scaphoid-capitate). The SL ligament is then repaired directly using micro-suture anchors placed into the scaphoid footprint. A dorsal capsulodesis (e.g., Blatt or Moran technique) may be added to augment the repair.
5. Closure: The capsular flap is meticulously repaired with non-absorbable sutures to prevent dorsal intercalated instability. The EPL is left transposed in the subcutaneous tissue to prevent attrition rupture against retained hardware or regenerating bone.
The Volar Approach (Extended Carpal Tunnel)
The volar approach is mandatory for Stage IV lunate dislocations to decompress the median nerve and repair the volar capsular rents, specifically the Space of Poirier.
1. Incision: An extended carpal tunnel incision is utilized, crossing the wrist crease obliquely (often incorporating a Bruner-type zigzag) to prevent debilitating flexion contractures.
2. Decompression: The transverse carpal ligament is divided completely, decompressing the median nerve. The nerve is gently retracted radially.
3. Reduction: The dislocated lunate is identified within the carpal canal. The volar radiocarpal ligaments are inspected for avulsions. The lunate is gently reduced dorsally into the lunate fossa. This often requires simultaneous dorsal pressure on the capitate and volar pressure on the lunate, facilitated by joystick K-wires.
4. Repair: The robust volar ligaments (radioscaphocapitate and radiolunotriquetral) are repaired using heavy non-absorbable sutures or suture anchors. This is frequently combined with a dorsal approach to address the concomitant SL and LT ligament tears (the "front-and-back" approach).
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, wrist surgery carries a significant risk of complications due to the tenuous blood supply of the carpus and the dense concentration of neurovascular structures. The surgeon must be prepared to identify and manage these complications promptly to prevent catastrophic functional loss.
Infection is relatively rare in elective wrist surgery (<2%) but increases significantly in open trauma. Complex Regional Pain Syndrome (CRPS) is a devastating complication characterized by severe pain, swelling, sudomotor changes, and joint stiffness. Its incidence can approach 5-10% following high-energy trauma. Early recognition and aggressive multimodal management—including neuropathic pain modulators (gabapentin), sympathetic blocks, and intensive occupational therapy—are critical.
Hardware complications, such as K-wire migration, pin-tract infections, or screw back-out, occur in 5-15% of cases. Nonunion is a particularly notorious complication following scaphoid fractures or intercarpal arthrodesis. Scaphoid nonunion rates can reach 10-15% depending on the fracture location (proximal pole fractures carry the highest risk due to retrograde blood supply). Avascular necrosis (AVN) of the scaphoid (Preiser's disease) or lunate (Kienböck's disease) can occur idiopathically or post-traumatically, leading to inevitable carpal collapse.
When primary reconstructive procedures fail, or post-traumatic osteoarthritis develops, salvage management is required. The goal shifts from preserving normal kinematics to providing a stable, painless wrist.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Scaphoid Nonunion | 10 - 15% | Proximal pole fracture; Delayed presentation; Inadequate immobilization. | Vascularized bone graft (e.g., 1,2-ICSRA); Screw revision; Salvage (PRC or 4CA) if SNAC develops. |
| Hardware Failure / Migration | 5 - 15% | Premature mobilization; Poor bone quality; Inadequate fixation construct. | Hardware removal; Revision internal fixation; Conversion to arthrodesis. |
| CRPS (Type I) | 5 - 10% | High-energy trauma; Prolonged immobilization; Median nerve irritation. | Aggressive hand therapy; Stellate ganglion blocks; Gabapentinoids; Vitamin C prophylaxis. |
| Post-Traumatic Osteoarthritis | 20 - 40% (Long-term) | Unrecognized SL tear (SLAC); Malreduced intra-articular fracture. | Proximal Row Carpectomy (PRC); Four-Corner Arthrodesis; Total Wrist Arthrodesis. |
| Lunate Avascular Necrosis | < 5% (Post-trauma) | Stage IV Lunate Dislocation; Disruption of volar/dorsal blood supply. | Revascularization procedures; Radial shortening osteotomy; Proximal row carpectomy. |
Phased Post-Operative Rehabilitation Protocols
The ultimate success of any complex wrist reconstruction is heavily dependent on strict adherence to a phased postoperative rehabilitation protocol. The delicate balance between protecting the surgical repair and preventing debilitating stiffness requires constant communication between the orthopaedic surgeon and the specialized hand therapist.
Phase I: Maximum Protection (0-2 Weeks)
Immediately following surgery, the wrist is immobilized in a bulky plaster splint or a rigid sugar-tong splint to prevent forearm rotation. Elevation above the level of the heart is mandatory to control edema. Active range of motion (ROM) of the non-immobilized joints—specifically the digits, thumb, elbow, and shoulder—is initiated on postoperative day one. This early digital motion is critical to prevent extensor tendon adhesions and to mitigate the risk of CRPS.
Phase II: Controlled Mobilization (2-8 Weeks)
At the 10-14 day mark, sutures are removed. Depending on the stability of the repair, the patient is transitioned to a custom-molded thermoplastic short-arm cast or a rigid removable splint. If K-wires were utilized for carpal stabilization (e.g., SL repair or perilunate reduction), they remain in place for a minimum of 8 weeks to allow for adequate biologic healing of the ligaments. During this phase, the splint is removed only for hygiene and highly supervised, gentle active ROM exercises. Proprioceptive re-education begins, emphasizing the Dart-Thrower's Motion (DTM). DTM (radial extension to ulnar flexion) is a highly functional arc of motion that occurs primarily at the midcarpal joint, thereby minimizing stress on the healing scapholunate interosseous ligament.
Phase III: Progressive Range of Motion (8-12 Weeks)
At 8 weeks, percutaneous K-wires are removed in the clinic. The patient begins a formal, intensive hand therapy program focusing on active and active-assisted ROM. Passive stretching and aggressive joint mobilization are strictly avoided during this early phase to prevent stretching out the newly repaired capsuloligamentous structures. Edema control via compression garments and scar management techniques (silicone gel pads, cross-friction massage) are optimized.
Phase IV: Strengthening and Return to Function (12+ Weeks)
Progressive strengthening is introduced using putty, grip devices, and graduated weights. Work-hardening programs are initiated for manual laborers. Patients must be extensively counseled that maximal medical improvement following major carpal reconstructive surgery may take up to 12 to 18 months. Furthermore, a mild to moderate permanent loss of terminal flexion and extension (typically 20-30% reduction compared to the contralateral side) is an expected outcome and does not signify clinical failure.
Summary of Landmark Literature and Clinical Guidelines
The contemporary management of wrist conditions is built upon a foundation of landmark biomechanical and clinical studies. Mastery of this literature is essential for the academic orthopaedic surgeon, as it directly dictates current treatment algorithms and evidence-based clinical guidelines.
Taleisnik’s seminal 1976 work on the columnar carpus revolutionized the understanding of load transmission across the wrist. By conceptualizing the scaphoid as the mobile link between the proximal and distal rows, Taleisnik provided the biomechanical rationale for why scaphoid fractures and SL dissociations are so devastating to global carpal kinematics. This was further refined by Lichtman’s Ring Theory, which elegantly explained the pathomechanics of intercalated segmental instability (VISI and DISI) and guided the development of targeted ligamentous reconstructions.
Mayfield, Johnson, and Kilcoyne’s 1980 cadaveric study remains the definitive text on perilunar instability. By demonstrating that carpal ligamentous failure occurs in a predictable, sequential pattern (Stages I through IV) based on wrist hyperextension, ulnar deviation, and intercarpal supination, they provided surgeons with a reliable roadmap for diagnosing and treating perilunate dislocations. Current clinical guidelines mandate that any patient presenting with a mechanism of injury consistent with Mayfield's criteria must undergo rigorous radiographic evaluation to rule out subtle Stage I or II injuries.
Watson and Ballet’s 1984 description of the Scapholunate Advanced Collapse (SLAC) pattern fundamentally altered the management of chronic wrist pain. They demonstrated that untreated SL dissociation leads to a predictable progression of osteoarthritis, beginning at the radial styloid, progressing to the entire radioscaphoid joint, and eventually involving the capitolunate articulation, while characteristically sparing the radiolunate joint. This observation forms the absolute basis for current salvage guidelines: Proximal Row Carpectomy is indicated only if the capitate head and lunate fossa are preserved, whereas Four-Corner Arthrodesis is required if midcarpal arthritis is present.
Finally, Berger’s anatomical studies on the dorsal capsuloligamentous structures of the wrist led to the development of the ligament-sparing dorsal capsulotomy. Current surgical guidelines strongly advocate for this tissue-preserving approach, as it significantly reduces the incidence of iatrogenic postoperative stiffness and dorsal instability, thereby improving long-term functional outcomes in complex carpal reconstructions.
