
A 32-year-old active manual laborer presents with persistent ulnar-sided wrist pain following a fall on an outstretched hand three months ago. Clinical examination reveals pain at the fovea and tenderness with DRUJ ballottement. You suspect a TFCC injury. What is your diagnostic and classification strategy, and why is the foveal attachment so clinically significant?

Candidate: I would examine the patient with the foveal stress test and look for DRUJ instability. I'd order an MRI to confirm. I would classify it using the Palmer classification system. The foveal attachment is important because it stabilizes the DRUJ, and if it's torn, the joint will be unstable.
Failure to distinguish between Palmer 1 (traumatic) and Palmer 2 (degenerative) lesions. Candidates often jump to imaging without mentioning dynamic arthroscopic testing (trampoline/hook tests) or failing to acknowledge that MRI often misses foveal avulsions due to the complex anatomy.
The candidate must define the Palmer classification (1A-D vs 2A-E). They should note that Palmer 1B (peripheral/foveal) is the focus here. They must emphasize that the foveal attachment is the "primary" stabilizer of the DRUJ. They should describe the "Trampoline test" (for central integrity) and the "Hook test" (for foveal avulsion) as the diagnostic gold standard, noting that MRI is useful but arthroscopy is definitive for assessing the foveal footprint.
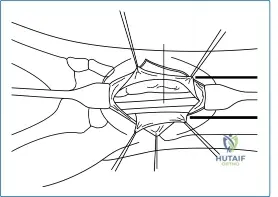
You are performing a diagnostic wrist arthroscopy. You have established the 3-4 portal. Describe the "nick and spread" technique for establishing this portal and detail the anatomical structures you are protecting to avoid iatrogenic complications.

Candidate: I use a #15 blade to only incise the skin. Then I use a mosquito hemostat to bluntly spread down to the capsule, pushing away nerves and veins, before inserting the cannula.
Ignoring the sensory nerves. A high-scoring candidate MUST mention the Superficial Branch of the Radial Nerve (SBRN) and the Dorsal Cutaneous Branch of the Ulnar Nerve (DCBUN) by name and explain that the "nick and spread" technique is specifically designed to prevent tethering/injury to these branches.
The 3-4 portal is between the EPL and EDC. The candidate must state: 1. Skin incision only with a blade. 2. Blunt spreading to the joint capsule to avoid injury to the sensory branches of the radial and ulnar nerves, which are mobile in the subcutaneous plane. 3. Mentioning that joint distension with 5-10ml saline prior to entry provides a 'cushion' that pushes the capsule away from the carpal surfaces, reducing the risk of articular scuffing.
During your midcarpal evaluation, you encounter this finding. What is the classification system used, and what does this grade imply for your management?

Candidate: That is a scapholunate ligament tear. I would use the Geissler classification. Grade 1 is attenuation, Grade 2 is mild separation, Grade 3 allows a probe to pass, and Grade 4 is complete instability.
Failing to mention the clinical significance. A Grade 3 or 4 Geissler lesion is not just an 'arthroscopic finding'; it is a potential precursor to SLAC wrist and dictates a change in management from simple debridement to potential ligament reconstruction or pinning.
The candidate must correctly define the Geissler Classification (I: attenuation/hemorrhage, II: step-off/separation, III: probe pass-through, IV: "drive-through" sign). They must add: "My management depends on the grade and chronicity. For Grade III/IV, I would evaluate the feasibility of arthroscopic-assisted pinning or open capsulodesis/reconstruction, stressing the importance of evaluating the scapholunate joint dynamically for progression to SLAC."
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding surgery-of-the-wrist