Lunotriquetral Ligament Repair and Augmentation: An Intraoperative Masterclass
Key Takeaway
This masterclass guides fellows through lunotriquetral ligament repair and augmentation, addressing ulnar-sided wrist instability. We cover comprehensive anatomy, meticulous preoperative planning, and step-by-step intraoperative execution, from incision to capsulotomy and ligament assessment. Emphasis is placed on neurovascular protection, precise instrument use, and critical decision-making. We also delve into pearls, pitfalls, and a robust postoperative rehabilitation protocol to ensure optimal patient outcomes for this complex wrist pathology.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues, to the operating theater. Today, we are undertaking a rigorous examination of a fascinating and notoriously challenging pathology: lunotriquetral (LT) ligament instability. While often overshadowed by its more common and heavily researched scapholunate (SL) counterpart, an isolated or complex injury to the lunotriquetral interosseous ligament can precipitate profound wrist dysfunction, debilitating ulnar-sided pain, and progressive carpal collapse. Our objective in this masterclass is to meticulously dissect the patho-anatomy, articulate precise surgical indications, and execute a flawless repair and augmentation of this critical ligamentous complex to restore native carpal kinematics.
The epidemiology of lunotriquetral ligament injuries is heterogeneous, often presenting a diagnostic conundrum for even the most seasoned hand surgeon. These injuries frequently manifest in the athletic population following acute trauma—typically a fall on an extended, radially deviated wrist that imparts an aggressive intercarpal supination moment. Alternatively, they represent a critical component of the progressive perilunate instability spectrum, specifically Mayfield stages III and IV, or as the primary vector in reverse perilunate injuries. A high index of clinical suspicion is mandatory, as these lesions are frequently missed on initial presentation, dismissing the patient's vague ulnar-sided wrist pain as a mere "sprain."

Pathophysiologically, lunotriquetral instability exists on a continuum. It begins with dynamic instability, where the ligament is partially torn or attenuated, leading to symptomatic "clunking" or catching during specific wrist arcs, despite normal static radiographs. If left untreated, or in cases of high-energy trauma, the injury progresses to static instability. This static collapse, classically recognized as Volar Intercalated Segment Instability (VISI), signifies not only the complete failure of the LT interosseous ligament but also the critical compromise of extrinsic secondary restraints. Understanding this progression from dynamic dysfunction to static collapse is the absolute cornerstone of formulating an effective surgical strategy.
Historically, the treatment algorithms for LT instability have been fraught with high failure rates and unpredictable functional outcomes. Early attempts at simple debridement often failed to address the underlying kinematic uncoupling, while primary arthrodesis (LT fusion) was marred by high non-union rates and unacceptable losses of radiocarpal motion. The modern paradigm, which we will detail extensively, focuses on anatomic or near-anatomic restoration of the ligamentous restraints. Through precise direct repair, judicious use of local capsulodesis, and robust tendon weaves for chronic deficiencies, we can re-establish the critical tether between the lunate and triquetrum, thereby halting the progression of degenerative arthropathy.
Detailed Surgical Anatomy and Biomechanics
Before we make our first incision, we must possess a three-dimensional mastery of the fundamental anatomy and biomechanics of the lunotriquetral complex. This region is unforgiving; a superficial understanding will inevitably lead to surgical failure.
The Lunotriquetral Interosseous Ligament Complex
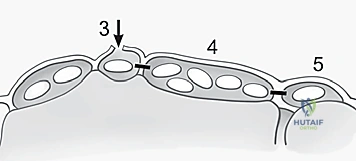
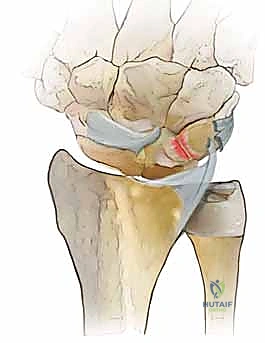
The lunotriquetral interosseous ligament is an intrinsic, highly specialized C-shaped structure that spans the dorsal, proximal, and palmar margins of the articulation between the lunate and the triquetrum. It is anatomically partitioned into three distinct subregions, each possessing unique histological characteristics and biomechanical responsibilities.
The Palmar Portion is the thickest, most robust, and biomechanically most crucial region of the entire LT complex. Composed of dense, transversely oriented collagen fibers, it plays the primary role in transmitting the extension moment of the triquetrum as it engages the hamate during ulnar deviation. Injury to this palmar stout ligament significantly compromises the stability of the proximal carpal row, allowing the triquetrum to abnormally extend independent of the lunate.

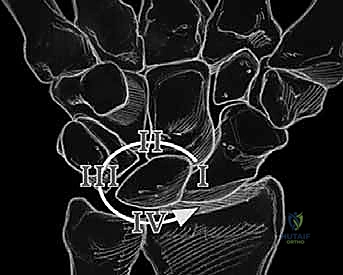


The Dorsal Portion, while quantitatively thinner and less robust than the palmar component, is absolutely vital as a primary rotational constraint. Its integrity is essential for preventing abnormal multi-planar rotation between the lunate and triquetrum. During our dorsal surgical approach, this is the portion we directly visualize and most frequently repair or augment. Finally, the Membranous Region is the central, delicate, avascular zone. It has negligible mechanical strength and minimal effect on rotation, translation, or distraction. Its primary physiological function is to serve as a synovial barrier between the radiocarpal and midcarpal joints; thus, isolated tears here are often clinically silent unless they create a symptomatic meniscoid lesion.
Carpal Kinematics and the Balanced Lunate
The lunate is the keystone of the proximal carpal row, often described in biomechanical literature as a "balanced lunate". It possesses no direct tendinous insertions and is entirely torque-suspended between the scaphoid and the triquetrum via the intrinsic interosseous ligaments. Inherently, due to its articulation with the radius and the trapezium/trapezoid, the scaphoid exhibits a strong tendency to palmar flex. Conversely, the triquetrum, driven by its helicoidal articulation with the hamate, strongly tends to extend.
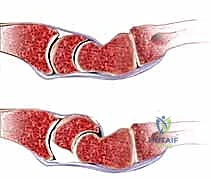
The scapholunate (SL) and lunotriquetral (LT) ligaments act as the critical tethers that balance these massive, opposing forces. They ensure that the entire proximal carpal row moves in a synchronous, coordinated fashion about the lunate during global wrist motion. When the lunotriquetral ligament complex is disrupted, this delicate equilibrium is violently uncoupled. The lunate, now freed from the extending force of the triquetrum, falls under the unopposed flexing influence of the scaphoid.



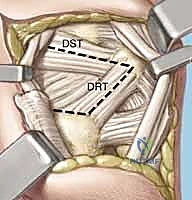
This uncoupling manifests as Volar Intercalated Segment Instability (VISI). However, a critical surgical axiom must be understood: VISI carpal collapse cannot be reproduced experimentally by simply sectioning the dorsal and palmar subregions of the LT ligament alone. The loss of integrity of the extrinsic secondary restraints, most notably the dorsal radiotriquetral (DRT) ligament, is an absolute prerequisite to create static carpal instability. On a standard lateral radiograph, a normal lunotriquetral angle is approximately 14 degrees. In a true VISI collapse, this angle can invert to -16 degrees or more, indicating profound volar flexion of the lunate relative to the triquetrum.
Neurovascular Topography and Ulnar Variance
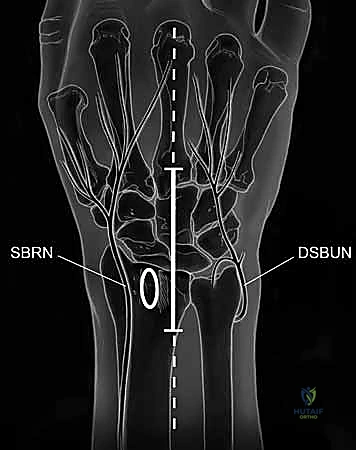
Surgical intervention in this region demands meticulous respect for the local neurovascular topography. During the dorsal approach, two neural structures are at paramount risk. The Dorsal Sensory Branch of the Ulnar Nerve (DSBUN) courses subcutaneously across the ulnar aspect of the dorsal wrist. It is highly susceptible to iatrogenic transection or traction neuropraxia during the initial skin incision and superficial flap elevation. Similarly, the Posterior Interosseous Nerve (PIN) terminates in the deep dorsal wrist capsule. Because it transmits nociceptive signals from the capsule, it is routinely identified and resected (neurectomy) to provide partial denervation and alleviate chronic deep aching pain, but it must be managed intentionally, not accidentally injured.
Furthermore, we must critically evaluate the patient's ulnar variance. Positive ulnar variance dramatically alters load transmission across the ulnocarpal joint. The increased forces can lead to attritional, degenerative tears of the LT ligament complex, often seen in the context of ulnar impaction syndrome. In such scenarios, repairing the LT ligament without addressing the positive ulnar variance (e.g., via an ulnar shortening osteotomy) is a biomechanical fallacy that guarantees surgical failure.
Exhaustive Indications and Contraindications
Patient selection is the ultimate determinant of surgical success in lunotriquetral ligament reconstruction. The decision matrix is complex, relying on the chronicity of the injury, the degree of instability, the presence of secondary restraint failure, and the biological quality of the remaining ligamentous tissue.


Direct anatomic repair is primarily indicated for acute injuries (less than 6 weeks old) where the ligament substance is avulsed from the bone (usually the triquetrum) but remains biologically robust. In subacute or chronic presentations (greater than 3-6 months), the ligament is typically attenuated, retracted, or replaced by non-functional scar tissue. In these instances, direct repair alone is insufficient and must be supplemented with a local capsulodesis or a formal tendon weave reconstruction to provide the necessary biomechanical strength while healing occurs.
Contraindications must be strictly observed. Advanced radiocarpal or midcarpal arthrosis (e.g., degenerative changes at the luno-hamate or pisotriquetral joints) precludes soft-tissue reconstruction, pushing the algorithm toward salvage procedures like limited intercarpal fusions. Additionally, a fixed, irreducible VISI deformity indicates severe, long-standing contractures that will inevitably doom a soft-tissue repair to stretch out and fail.
| Category | Indications for LT Repair/Augmentation | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Clinical Status | Symptomatic dynamic or static LT instability failing 3-6 months of conservative care. | Advanced radiocarpal or midcarpal osteoarthritis. | Poor patient compliance; active heavy manual labor without willingness to modify. |
| Chronicity | Acute (<6 weeks) for direct repair; Chronic (>6 months) requires augmentation/weave. | Fixed, irreducible carpal collapse (irreducible VISI). | Active smoking (significantly impairs ligamentous healing). |
| Anatomy | Reducible carpal alignment; sufficient bone stock for anchor/tunnel placement. | Active local or systemic infection. | Severe positive ulnar variance (must be addressed concurrently with shortening osteotomy). |
| Concomitant Injury | Part of a perilunate dislocation repair algorithm. | Inflammatory arthropathies (e.g., Rheumatoid Arthritis) destroying intrinsic ligaments. | Unaddressed concomitant SL ligament complete rupture. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative preparation sets the stage for a seamless intraoperative experience. The diagnosis of LT instability is notoriously elusive, demanding a battery of specific provocative tests and advanced imaging modalities to confirm the pathology and plan the exact surgical trajectory.
Clinical Evaluation and Provocative Testing
Patients typically present with insidious, vague ulnar-sided wrist pain, often exacerbated by power grip, ulnar deviation, and pronation. On physical examination, pinpoint tenderness directly over the dorsal LT interval is a hallmark sign. However, dynamic testing is where the true functional deficit is revealed. The Ballottement Test (or Reagan test) is performed by firmly stabilizing the lunate with the thumb and index finger of one hand while grasping the triquetrum and pisiform with the other; translating the triquetrum dorsally and volarly will elicit severe pain, crepitus, and increased excursion compared to the contralateral wrist.



Furthermore, the Shear Test (Kleinman's test) involves stabilizing the radiolunate joint while applying a dorsally directed force to the pisiform, loading the palmar LT ligament and producing a painful "clunk." In cases of dynamic instability, moving the wrist from radial deviation to ulnar deviation under axial compression may elicit a sudden, painful "catch-up" clunk. This occurs because the triquetrum, initially uncoupled, suddenly snaps back into alignment with the lunate. Real-time videofluoroscopy is an invaluable adjunct during this maneuver to visualize the transient subluxation.
Advanced Imaging Modalities
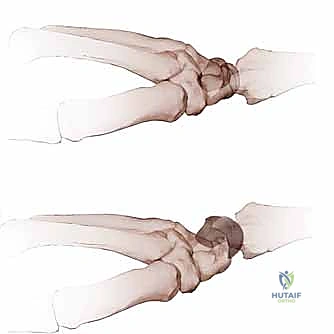
Standard plain radiographs are frequently normal in isolated, dynamic LT injuries. However, meticulously positioned clenched-fist anteroposterior, radial, and ulnar deviation views are mandatory. The surgeon must scrutinize Gilula's arcs for subtle step-offs. While a static LT gap (diastasis) is much less common than in SL injuries, proximal translation of the triquetrum or an overlap of the lunate and triquetrum profiles strongly suggests instability. A true lateral view is critical to measure the radiolunate and lunotriquetral angles to diagnose a static VISI deformity.
When plain films are equivocal, Magnetic Resonance Imaging (MRI) or MR Arthrography is deployed. High-resolution 3T MRI can visualize the dorsal and palmar bands of the LT ligament, though its sensitivity is lower than for the SL ligament. Triple-injection cine-arthrography can demonstrate dye leakage between the radiocarpal and midcarpal joints, but this must be correlated tightly with clinical symptoms, as asymptomatic, age-related degenerative perforations of the membranous LT ligament are highly prevalent in patients over 40. Ultimately, diagnostic wrist arthroscopy remains the gold standard, allowing direct probing of the LT interval to assess for abnormal step-off and loss of tension (Geissler classification).
Operative Setup and Anesthesia
The procedure is typically performed under regional anesthesia (supraclavicular or axillary block) supplemented with intravenous sedation, or under general anesthesia depending on patient preference and expected duration. An upper arm pneumatic tourniquet is applied over copious padding and inflated to 250 mmHg following exsanguination with an Esmarch bandage.


The patient is positioned supine with the operative extremity extended on a radiolucent hand table. The surgeon sits at the axilla, with the assistant opposite. A mini C-arm fluoroscopy unit is brought in perpendicular to the table or from the head of the table, ensuring unobstructed orthogonal views of the carpus without compromising the sterile field. Preoperative templating should include ensuring the availability of 1.0mm and 1.2mm Kirschner wires (K-wires), micro-suture anchors (1.5mm to 2.0mm), and fine non-absorbable braided sutures.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution requires a masterful blend of delicate soft-tissue handling, precise spatial awareness, and rigid biomechanical stabilization. We will outline the dorsal approach, which is the workhorse for LT ligament repair and augmentation.
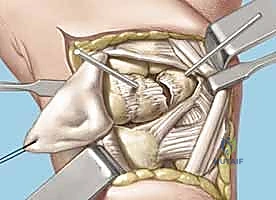
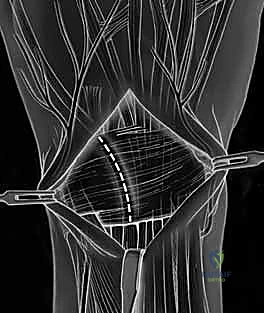
Exposure and Capsulotomy
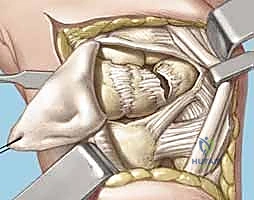
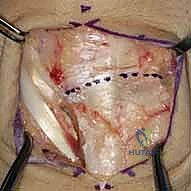
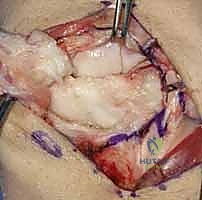
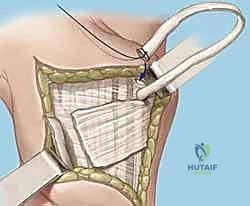
A 5 to 6 cm dorsal longitudinal incision is centered over the radiocarpal joint, in line with the third metacarpal. Careful subcutaneous dissection is paramount to identify and protect the crossing branches of the Dorsal Sensory Branch of the Ulnar Nerve (DSBUN) on the ulnar side, and the superficial radial nerve on the radial side. Veins are preserved where possible to minimize postoperative edema. The extensor retinaculum is identified, and the third extensor compartment is opened to transpose the Extensor Pollicis Longus (EPL) radially.
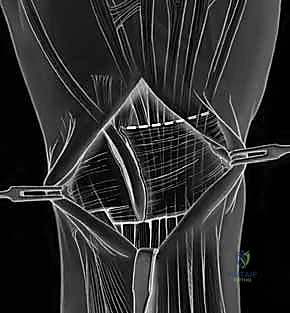
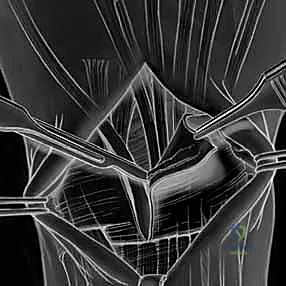
Subperiosteal elevation of the fourth and fifth extensor compartments exposes the dorsal wrist capsule. At this juncture, the Posterior Interosseous Nerve (PIN) is identified on the floor of the fourth compartment, meticulously dissected, and a 1 cm segment is resected to partially denervate the capsule. We then perform a ligament-sparing capsulotomy—typically a modified Berger dorsal radiocarpal flap or a ligament-splitting approach—preserving the integrity of the dorsal intercarpal (DIC) and dorsal radiocarpal (DRC) ligaments for later robust closure.
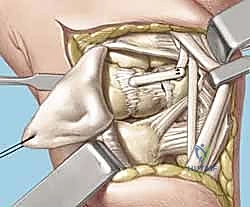
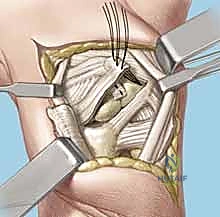
Joint Preparation and Ligament Assessment
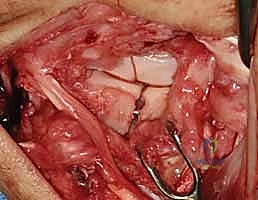
Upon entering the joint, the radiocarpal and midcarpal articulations are thoroughly inspected. The lunotriquetral interval is specifically probed. In an acute avulsion, the dorsal and membranous portions of the ligament will be visibly detached, usually from the triquetral footprint. In chronic cases, the interval may be filled with reactive synovitis and amorphous scar tissue.



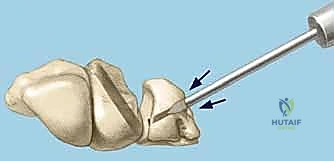
We use a motorized shaver or fine rongeur to meticulously debride the redundant scar and the avascular membranous portion of the ligament, taking extreme care not to violate the critical palmar LT ligament if it remains partially intact. The bony footprints on the lunate and triquetrum are then decorticated using a high-speed burr or curette down to punctate bleeding cancellous bone. This raw bony bed is absolutely critical to stimulate the biological healing response necessary for ligament-to-bone integration.
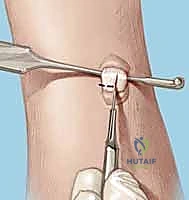
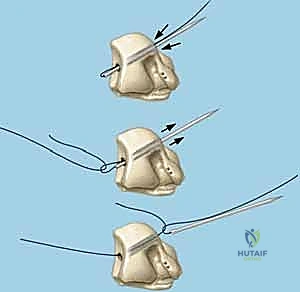
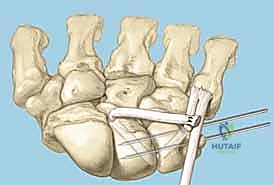
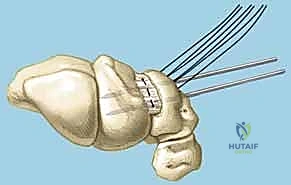
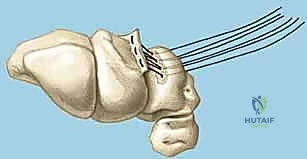
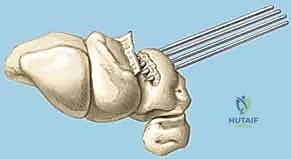
Reduction and Temporary Fixation
Achieving an anatomic reduction before any fixation is applied is non-negotiable. We utilize the "joystick technique" to manipulate the carpal bones. A 1.2mm K-wire is driven dorsally into the lunate, and another into the triquetrum. These wires act as levers. If a VISI deformity is present, the lunate is extended (dorsiflexed) using its joystick, while the triquetrum is simultaneously flexed and translated radially to close the LT interval.