Osteoarthritis of the Wrist: SLAC Management
Key Takeaway
Scapholunate Advanced Collapse (SLAC) is the most common pattern of degenerative wrist osteoarthritis, typically resulting from chronic scapholunate instability. This predictable progression of articular wear spares the radiolunate joint, allowing for motion-preserving salvage procedures. Surgical management depends on the specific stage of degeneration, with options ranging from radial styloidectomy to proximal row carpectomy (PRC) and four-corner arthrodesis, aiming to relieve pain while maintaining functional wrist kinematics.
Comprehensive Introduction and Patho-Epidemiology
Historical Context and Definition
Degenerative osteoarthritis of the wrist is a complex, progressive condition that historically presented a formidable challenge to the orthopaedic surgeon. The most frequent and predictable pattern of articular wear in the human carpus is the Scapholunate Advanced Collapse (SLAC) wrist. Originally elucidated by H. Kirk Watson in the early 1980s, the SLAC pattern is recognized not merely as a random degenerative process, but as an inexorable biomechanical consequence of chronic carpal instability. The condition is intrinsically related to the structural failure of the scapholunate (SL) interosseous ligament, which serves as the primary stabilizer between the scaphoid and lunate. When this vital ligamentous tether is disrupted—typically as a posttraumatic sequela of an untreated or unrecognized hyperextension injury—the synchronous kinematics of the proximal carpal row are irrevocably altered.
Epidemiological Profile
Epidemiologically, SLAC wrist represents the most common etiology of degenerative arthritis in the wrist, accounting for over fifty percent of all carpal osteoarthritis cases observed in clinical practice. It predominantly affects middle-aged to older adults, with a distinct predilection for the male demographic, largely reflecting occupational hazards and a higher incidence of high-energy trauma or repetitive loading activities. Interestingly, many patients present with advanced arthritic changes without recalling a specific, severe traumatic event, often attributing their historical injury to a benign "sprain" that was inadequately immobilized or entirely ignored. This highlights the insidious nature of scapholunate dissociation, where the initial ligamentous insult may be minimally symptomatic, but the long-term kinematic uncoupling leads to catastrophic articular degradation over a period of years to decades.
Pathogenesis of Cartilage Degradation
The pathogenesis of cartilage degradation in the SLAC wrist is a textbook example of altered contact mechanics leading to focal chondral wear. In a healthy wrist, the articular surfaces of the radiocarpal and midcarpal joints are highly congruent, allowing for an even distribution of axial loads across broad surface areas. However, following scapholunate dissociation, the scaphoid assumes a pathologically flexed and pronated posture. This rotary subluxation drastically reduces the contact area between the proximal pole of the scaphoid and the scaphoid fossa of the distal radius. The resultant point-loading generates localized areas of extreme peak pressure, far exceeding the physiological tolerance of the hyaline cartilage. At the cellular level, this mechanical overload induces chondrocyte apoptosis, proteoglycan depletion, and the release of pro-inflammatory cytokines such as interleukin-1 (IL-1) and tumor necrosis factor-alpha (TNF-α), culminating in irreversible cartilage matrix destruction, subchondral sclerosis, and osteophyte formation.
Detailed Surgical Anatomy and Biomechanics
Osseous Architecture and Articular Geometry
To fully comprehend the management of SLAC wrist, the surgeon must possess an intimate understanding of carpal osseous architecture. The proximal carpal row—comprising the scaphoid, lunate, and triquetrum—functions as an intercalated segment. It has no direct tendinous insertions to actively control its spatial orientation; rather, its movement is entirely dictated by the mechanical forces transmitted from the distal carpal row and the restraining forces of the intrinsic and extrinsic ligaments. The scaphoid acts as an essential mechanical tie-rod bridging the proximal and distal carpal rows. Its complex, twisted geometry allows it to articulate with five different bones, making it the linchpin of carpal stability. The lunate, situated centrally, features a spherical proximal articular surface that sits highly congruently within the elliptical lunate fossa of the distal radius. This specific geometric relationship is paramount, as it ensures that the radiolunate articulation remains remarkably preserved even in the most advanced stages of SLAC wrist.
Intrinsic and Extrinsic Ligamentous Anatomy
The stability of the carpus relies heavily on a robust network of intrinsic and extrinsic ligaments. The scapholunate interosseous ligament (SLIL) is a C-shaped intrinsic ligament with three distinct anatomical and biomechanical regions: dorsal, proximal (membranous), and volar. The dorsal region is the thickest and most critical for resisting translational and rotational forces. Extrinsic ligaments, particularly the volar radioscaphocapitate (RSC) ligament and the dorsal intercarpal (DIC) ligament, provide secondary stabilization. The RSC ligament acts as a crucial volar sling, preventing ulnar translation of the carpus. During surgical interventions, particularly Proximal Row Carpectomy (PRC), meticulous preservation of the RSC ligament is an absolute surgical mandate to prevent postoperative volar-ulnar subluxation of the remaining carpus.
Kinematic Uncoupling and Load Transmission
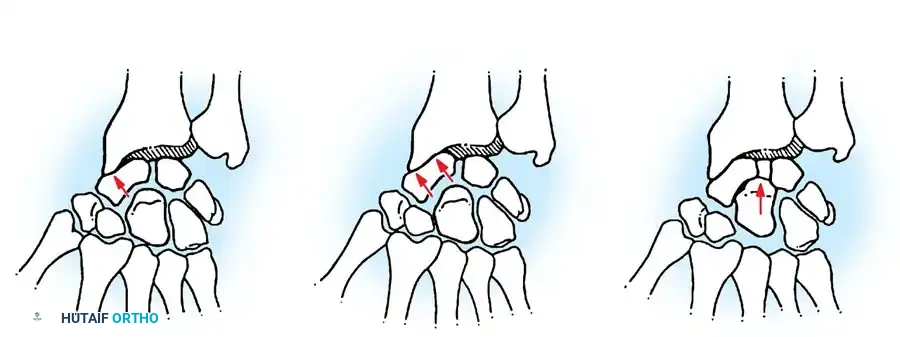
During normal wrist kinematics, the scaphoid and lunate move synergistically. The scaphoid has a natural biomechanical propensity to flex under the longitudinal loading of the trapezium and trapezoid, while the triquetrum has a natural tendency to extend due to its helicoidal articulation with the hamate. The lunate, intercalated between the two, is perfectly balanced by the intact SLIL and lunatotriquetral (LT) ligaments. When the SLIL is ruptured, this delicate kinetic balance is utterly destroyed. The scaphoid flexes uninhibitedly, while the lunate, now tethered only to the triquetrum, falls into extension, creating a Dorsal Intercalated Segment Instability (DISI) deformity. This uncoupling shifts the load transmission path. Instead of force being distributed evenly, the proximal pole of the flexed scaphoid point-loads against the dorsal rim of the radius, while the distal pole impinges on the radial styloid. This abnormal load transmission initiates the highly predictable, sequential pattern of articular wear that characterizes the SLAC wrist.
Exhaustive Indications and Contraindications
Radiographic Staging and Surgical Selection
The selection of the appropriate surgical intervention for SLAC wrist is strictly dictated by the radiographic stage of the disease, utilizing standard posteroanterior (PA), lateral, and clenched-fist radiographs. Watson's original classification defines the progression. Stage I involves degenerative changes localized strictly to the radial styloid and the distal pole of the scaphoid. Stage II exhibits osteoarthritis progressing to involve the entire radioscaphoid articulation. Stage III demonstrates advancing degenerative processes into the midcarpal joint, specifically the capitolunate articulation, while the radiolunate joint remains completely spared. Stage IV, or pancarpal arthritis, involves the radiolunate joint and precludes motion-preserving procedures. The surgeon must correlate these radiographic findings with the patient's age, functional demands, manual labor requirements, and baseline range of motion to formulate an optimal, individualized surgical plan.
Table of Indications and Contraindications
| Surgical Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Radial Styloidectomy (± Denervation) | Stage I SLAC; Isolated radial styloid impingement; Low-demand patients seeking pain relief. | Stage II or III SLAC; Ulnar translocation of the carpus. | High-demand manual laborers; Significant carpal instability. |
| Proximal Row Carpectomy (PRC) | Stage II SLAC; Patients prioritizing range of motion over maximal grip strength. | Stage III SLAC (Capitolunate arthritis); Lunate fossa arthritis; Damage to the RSC ligament. | Heavy manual laborers; Inflammatory arthropathies; Severe ulnar positive variance. |
| Four-Corner Arthrodesis (4CA) | Stage II or Stage III SLAC; High-demand patients requiring maximal grip strength preservation. | Stage IV SLAC (Radiolunate arthritis); Active joint infection; Inadequate bone stock for fusion. | Heavy smokers (high nonunion risk); Elderly patients with low functional demands. |
| Total Wrist Arthrodesis | Stage IV SLAC (Pancarpal arthritis); Failed PRC or 4CA; Severe inflammatory arthritis. | Open physes (in pediatric patients, though rare in SLAC); Active untreated infection. | Patients requiring wrist motion for activities of daily living or specific occupations. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical and Radiographic Assessment
A meticulous pre-operative clinical evaluation is the foundation of successful surgical management. Patients typically present with an insidious onset of dorsal radial wrist pain, progressive loss of extension and radial deviation, and a marked diminution in grip strength compared to the contralateral extremity. Physical examination must include a thorough assessment of the Watson Scaphoid Shift Test, evaluating for the painful dorsal subluxation of the proximal scaphoid pole over the dorsal rim of the radius. Standard radiographs must be scrutinized for the exact extent of joint space narrowing, subchondral cyst formation, and osteophyte presence. The lateral view is critical for quantifying the degree of the DISI deformity, specifically measuring the radiolunate and scapholunate angles, which will dictate the amount of correction required during a four-corner arthrodesis.
Advanced Imaging and Pre-Operative Templating
While plain radiography remains the gold standard for staging, advanced imaging modalities play a vital adjunctive role. Computed Tomography (CT) scans, particularly with sagittal and coronal reformats, are invaluable for assessing the precise integrity of the capitolunate and radiolunate articulations. If there is any ambiguity regarding the presence of Stage III changes, a CT scan is mandatory before committing to a Proximal Row Carpectomy, as unrecognized capitate head arthritis will lead to rapid procedure failure. Pre-operative templating is essential when planning a four-corner fusion. The surgeon must template the size of the circular dorsal fusion plate or the trajectory of headless compression screws to ensure adequate bone purchase without violating the radiolunate joint or the distal articular surfaces of the capitate and hamate.
Operating Room Setup and Patient Positioning
Optimal operating room setup and patient positioning are critical for facilitating precise surgical execution. The patient is positioned supine on the operating table with the affected upper extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Regional anesthesia, such as a supraclavicular or axillary brachial plexus block, is highly recommended as it provides excellent intraoperative muscle relaxation and superior postoperative analgesia. The fluoroscopy unit (C-arm) must be positioned to allow for unobstructed, orthogonal views of the wrist without compromising the sterile field. The surgeon typically sits in the axilla, allowing direct visualization of the dorsal carpus. Prophylactic intravenous antibiotics are administered prior to tourniquet inflation, adhering to strict institutional antimicrobial stewardship protocols.
Step-by-Step Surgical Approach and Fixation Technique
The Dorsal Approach and Neurectomy
Both Proximal Row Carpectomy and Four-Corner Arthrodesis utilize a standard dorsal approach to the wrist. A longitudinal skin incision is made centered over Lister's tubercle, extending from the distal radius to the base of the third metacarpal. Full-thickness fasciocutaneous flaps are elevated to protect the superficial sensory branches of the radial nerve and the dorsal sensory branch of the ulnar nerve. The extensor retinaculum is incised longitudinally over the third dorsal compartment, and the extensor pollicis longus (EPL) tendon is mobilized and transposed radially. A routine posterior interosseous nerve (PIN) neurectomy is performed at this stage; the nerve is identified on the floor of the fourth extensor compartment, intricately associated with the terminal branch of the anterior interosseous artery, and approximately 1 to 2 centimeters of the nerve is resected to provide adjunctive denervation analgesia. A ligament-sparing dorsal capsulotomy, such as the Berger Mayo approach, is then executed. This involves creating a distally based capsular flap by incising along the dorsal intercarpal (DIC) and dorsal radiocarpal (DRC) ligaments, preserving their integrity for robust closure.
Proximal Row Carpectomy Technique
When executing a Proximal Row Carpectomy (PRC) for Stage II SLAC wrist, the objective is the meticulous en bloc or piecemeal excision of the scaphoid, lunate, and triquetrum. Threaded Steinmann pins or specialized corkscrew retractors are inserted into the bones to serve as joysticks, facilitating manipulation. The surgeon must sharply dissect the robust volar ligamentous attachments. Extreme caution is paramount when excising the volar aspect of the proximal row to avoid injuring the underlying radioscaphocapitate (RSC) ligament. The RSC ligament serves as the primary restraint preventing ulnar translation of the carpus; its iatrogenic transection is a catastrophic error that will result in immediate and profound carpal destabilization. Once the proximal row is excised, the proximal pole of the capitate is carefully seated into the lunate fossa of the distal radius. The joint is taken through a full range of motion under fluoroscopy to confirm congruent tracking and the absence of impingement. The dorsal capsule is then meticulously repaired using non-absorbable sutures to prevent dorsal subluxation of the capitate.
Scaphoid Excision and Four-Corner Arthrodesis Technique
For Stage III SLAC wrist, a Four-Corner Arthrodesis (4CA) is the definitive procedure. Following the dorsal exposure, the entire scaphoid is excised. This excision decompresses the radial side of the wrist, eliminating the primary pain generator. The articular surfaces between the capitate, hamate, lunate, and triquetrum are then systematically decorticated. Using a high-speed burr or sharp curettes, the cartilage and subchondral plate are removed down to healthy, bleeding cancellous bone. Thermal necrosis must be strictly avoided by utilizing copious cold saline irrigation during burring. The DISI deformity of the lunate must be anatomically corrected; a K-wire is driven into the lunate to flex it back into a neutral, collinear alignment with the radius. The capitate is subsequently reduced onto the lunate.
Fixation is achieved using either multiple headless compression screws or a dorsal circular locking plate. If a dorsal plate is utilized, the dorsal cortices of the four carpal bones must be flattened with a burr to allow the plate to sit flush, thereby preventing postoperative extensor tendon irritation. Cancellous bone graft, harvested from the excised scaphoid (if structurally viable and non-sclerotic) or from the distal radius at Lister's tubercle, is tightly packed into the decorticated interstices. Rigid compression is confirmed fluoroscopically. The dorsal capsule is repaired, and the extensor retinaculum is closed over the fourth and fifth compartments, leaving the EPL transposed in the subcutaneous tissue.
Complications, Incidence Rates, and Salvage Management
Procedure-Specific Complications
While motion-preserving salvage procedures for SLAC wrist are highly efficacious, they are not without significant potential complications. Following a Four-Corner Arthrodesis, nonunion represents the most formidable challenge, occurring most frequently at the capitolunate interface due to its relatively limited cancellous surface area and the high shear forces across the midcarpal joint. Patient factors, particularly tobacco use, exponentially increase the risk of nonunion. Hardware complications are also prevalent; dorsal circular plates, if not adequately countersunk, can lead to extensor tendon tenosynovitis or outright attritional rupture. Following a Proximal Row Carpectomy, the most concerning long-term complication is the development of progressive radiocapitate osteoarthritis. The geometric mismatch between the capitate head and the lunate fossa alters contact mechanics, which can lead to progressive chondral wear over a period of 10 to 15 years, although many patients remain clinically asymptomatic despite radiographic progression.
Table of Complications and Incidence Rates
| Complication | Associated Procedure | Estimated Incidence | Prevention and Management Strategy |
|---|---|---|---|
| Nonunion | Four-Corner Arthrodesis | 3% - 10% | Prevention: Meticulous decortication, rigid compression, smoking cessation. Management: Revision bone grafting and internal fixation. |
| Hardware Impingement | Four-Corner Arthrodesis | 5% - 15% | Prevention: Countersinking dorsal plates, utilizing headless screws. Management: Hardware removal after solid fusion is achieved. |
| Progressive Radiocapitate OA | Proximal Row Carpectomy | 15% - 20% (Long-term) | Prevention: Strict adherence to indications (No Stage III). Management: Observation if asymptomatic; Total Wrist Fusion if painful. |
| Ulnar Translocation | Proximal Row Carpectomy | < 2% | Prevention: Absolute preservation of the volar RSC ligament during excision. Management: Total Wrist Arthrodesis. |
| Postoperative Stiffness | Both (PRC and 4CA) | 10% - 25% | Prevention: Early, controlled mobilization; precise capsular repair. Management: Aggressive hand therapy, dynamic splinting, rarely surgical release. |
Salvage Strategies
When motion-preserving procedures fail—whether due to symptomatic nonunion, progressive radiocapitate arthritis, or deep periprosthetic infection—the ultimate salvage strategy is a Total Wrist Arthrodesis. This involves the complete fusion of the distal radius to the remaining carpal bones and the third metacarpal utilizing a robust dorsal spanning plate. While Total Wrist Arthrodesis sacrifices all radiocarpal and midcarpal motion, it provides highly reliable, durable pain relief and a stable platform for power grip, making it an excellent definitive option for heavy manual laborers or patients with end-stage, intractable pain following failed SLAC reconstruction.
Phased Post-Operative Rehabilitation Protocols
Acute Post-Operative Phase
The immediate postoperative rehabilitation protocol is designed to protect the surgical repair while minimizing edema and preventing stiffness in the uninvolved digits. Regardless of whether a PRC or 4CA was performed, the patient's wrist is immobilized in a bulky, compressive soft dressing reinforced with a rigid volar orthosis or a short-arm sugar-tong splint. The wrist is positioned in approximately 10 to 15 degrees of extension. Strict elevation of the extremity above the level of the heart is mandated for the first 48 to 72 hours to mitigate swelling. Active range of motion (AROM) of the fingers, thumb, elbow, and shoulder is initiated on postoperative day one. Digital tendon gliding exercises are crucial to prevent adhesions, particularly in the extensor compartments adjacent to the surgical site.
Intermediate Mobilization Phase
The intermediate phase diverges based on the specific surgical procedure and the rigidity of the fixation. For a Proximal Row Carpectomy, the initial splint is typically discontinued at 2 to 3 weeks postoperatively. At this juncture, supervised active and active-assisted range of motion exercises for the wrist are initiated. A removable custom thermoplastic splint is fabricated to be worn between exercise sessions and at night. For a Four-Corner Arthrodesis utilizing rigid internal fixation (such as a dorsal circular plate or headless compression screws), gentle AROM may also commence at 2 to 4 weeks. However, if less rigid fixation (such as K-wires) was employed, strict cast immobilization must be maintained for a minimum of 6 to 8 weeks until definitive radiographic evidence of trabecular bridging across the arthrodesis sites is confirmed.
Advanced Strengthening and Return to Activity
The advanced phase focuses on restoring functional strength, proprioception, and endurance. For PRC patients, progressive strengthening exercises utilizing light weights and resistance bands typically commence at 6 weeks postoperatively. Patients generally achieve their maximal, final range of motion between 3 to 6 months. For 4CA patients, strengthening is deferred until solid clinical and radiographic union is unequivocally established, often taking 8 to 12 weeks. Heavy lifting, impact loading, and the use of vibratory tools are strictly prohibited until the fusion mass is completely consolidated. Both procedures reliably preserve approximately 50% to 60% of the contralateral, normal wrist arc of motion. However, 4CA generally provides superior preservation of grip strength (approximately 70% to 80% of normal) compared to PRC, making it the preferred choice for patients with high physical demands.
Summary of Landmark Literature and Clinical Guidelines
Foundational Studies in SLAC Management
The modern management of SLAC wrist is deeply rooted in foundational orthopaedic literature. H. Kirk Watson's seminal paper in 1984 definitively characterized the predictable pattern of scapholunate advanced collapse, forever altering the diagnostic and therapeutic approach to carpal arthritis. Subsequent landmark studies by Krakauer, Bishop, and Cooney from the Mayo Clinic provided rigorous, long-term outcome data validating both Proximal Row Carpectomy and Four-Corner Arthrodesis as highly effective motion-preserving options. These studies established the critical importance of preserving the radiolunate joint and highlighted the distinct biomechanical advantages of each procedure. The literature clearly dictates that the presence of capitolunate arthritis is the absolute dividing line in surgical decision-making, strictly contraindicating PRC in favor of midcarpal arthrodesis.
Comparative Outcomes of Motion-Preserving Procedures
Extensive systematic reviews and meta-analyses comparing PRC and 4CA have consistently demonstrated that both procedures offer excellent, comparable relief of pain and high rates of patient satisfaction. Range of motion outcomes are generally equivalent, though some studies suggest a slight advantage in flexion-extension arc for PRC. Grip strength preservation consistently favors 4CA. The complication profiles, however, differ significantly. 4CA is associated with hardware-related complications and a definitive risk of nonunion, necessitating meticulous surgical technique and rigid fixation. Conversely, PRC avoids the risk of nonunion and hardware failure but carries the long-term specter of radiocapitate osteoarthritis. Ultimately, clinical guidelines recommend a highly individualized approach, synthesizing the patient's specific radiographic stage, anatomical variations, functional requirements, and the surgeon's technical proficiency to optimize outcomes in the management of SLAC wrist.
