Mastering Triangular Fibrocartilage Complex (TFCC) Repair: An Intraoperative Guide

Key Takeaway
This masterclass guides fellows through the intricate world of Triangular Fibrocartilage Complex (TFCC) repair. We delve into detailed wrist anatomy, preoperative planning, and a granular, step-by-step intraoperative execution of arthroscopic and open techniques. Emphasizing critical decision-making, complication avoidance, and comprehensive rehabilitation, this session equips surgeons with the expertise to manage challenging ulnar-sided wrist pathologies effectively.
Comprehensive Introduction and Patho-Epidemiology
Ulnar-sided wrist pain has historically been referred to as the "black box" of orthopedic hand surgery, representing a complex diagnostic and therapeutic challenge for even the most seasoned clinicians. At the epicenter of this anatomical labyrinth lies the Triangular Fibrocartilage Complex (TFCC), a multifaceted, dynamic unit that serves as the primary stabilizer of the distal radioulnar joint (DRUJ) and the pivotal shock absorber for the ulnar carpus. When this critical structure is compromised, patients frequently experience a precipitous decline in grip strength, profound rotational instability, and debilitating pain that severely curtails their functional independence and occupational capacities.
The epidemiological burden of TFCC injuries is substantial, encompassing both acute traumatic events in young, active demographics and insidious degenerative cascades in older populations. Traumatic ruptures are frequently observed in athletes participating in racquet sports, gymnastics, and contact athletics, often resulting from a fall on an outstretched hand (FOOSH) involving forced extension and pronation. Conversely, degenerative tears exhibit a strong correlation with advancing age and positive ulnar variance, where chronic ulnocarpal impaction inexorably compromises the structural integrity of the fibrocartilaginous disc.
Understanding the TFCC requires a paradigm shift from viewing it as a static cartilaginous spacer to recognizing it as a sophisticated, tension-bearing ligamentous network. It functions analogously to the meniscus of the knee but is subjected to far more complex, multidirectional torsional loads during physiological forearm rotation. The intricate interplay between the TFCC, the surrounding osseous architecture, and the dynamic muscular stabilizers dictates the mechanical harmony of the wrist. Disruption of this harmony not only precipitates immediate localized pain but also initiates a predictable sequence of kinematic derangements, ultimately culminating in DRUJ arthrosis if left unaddressed.
Our objective in this definitive guide is to systematically deconstruct the complexities of TFCC pathology. Through meticulous clinical evaluation, precise advanced imaging, and masterful surgical execution, orthopedic surgeons can reliably restore anatomical stability, alleviate debilitating symptoms, and facilitate a robust functional return. This chapter will provide an exhaustive, evidence-based roadmap for navigating the intraoperative nuances of TFCC repair, ensuring optimal outcomes in these technically demanding cases.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional comprehension of the TFCC's surgical anatomy is an absolute prerequisite for safe and efficacious operative intervention. The TFCC is not a singular entity but a composite structure strategically interposed between the distal ulna and the ulnar carpus.
The TFCC: Structure and Attachments
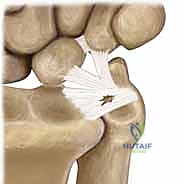
The TFCC is a heterogeneous cartilaginous and ligamentous complex originating distally from the sigmoid notch of the radius. This origin is a concave articular surface located on the medial aspect of the distal radius. From this radial footprint, the complex extends ulnarly to insert into the base of the ulnar styloid and the fovea—a deep, critical depression at the base of the styloid.

The structural integrity of the TFCC is heavily reliant on its peripheral ligamentous thickenings, specifically the dorsal and volar radioulnar ligaments. These robust fibrous bands are the primary restraints against abnormal translation of the DRUJ. They function synergistically to limit both rotational excursion and axial migration of the ulna relative to the radius, ensuring congruity during the complex arc of forearm pronation and supination.
Furthermore, the TFCC is intimately tethered to the ulnar carpus via the ulnocarpal ligament complex. This complex comprises the ulnolunate, ulnotriquetral, and ulnar collateral ligaments, which function as a cohesive, tension-sharing unit. The central, horizontal portion of the articular disc is markedly thinner and composed of obliquely oriented collagen fibers designed to resist multidirectional shear stresses, though it lacks the tensile strength of the peripheral ligaments.
Vascularity and Healing Potential
The vascular topography of the TFCC is perhaps the most critical anatomical variable dictating our surgical decision-making. The blood supply is derived primarily from the ulnar artery via its radiocarpal branches, supplemented by the dorsal and palmar branches of the anterior interosseous artery. These vessels arborize and penetrate the TFCC in a radial fashion, creating distinct zones of vascularity.
Histological and microangiographic studies have unequivocally demonstrated that these vessels perfuse only the peripheral 10% to 40% of the complex. This well-vascularized periphery is often termed the "red zone." In stark contrast, the central articular disc and its radial attachment are entirely avascular, relying solely on synovial diffusion for nutrition.
This dichotomous vascularity forms the biological rationale for our treatment algorithms. Peripheral tears within the vascularized zone possess a robust intrinsic healing capacity and are therefore prime candidates for anatomical surgical repair. Conversely, traumatic or degenerative lesions localized to the avascular central zone exhibit virtually no healing potential; thus, attempting a primary suture repair in this region is biologically futile, and these lesions are universally managed with meticulous arthroscopic debridement to stable margins.
Neurovascular Risks and Muscular Intervals
Navigating the ulnar aspect of the wrist requires hyper-vigilance regarding several critical neurovascular and musculotendinous structures. The ulnar nerve and artery pass through Guyon's canal just volar to the operative field, demanding respect during volar portal placement or open approaches.
Of paramount concern to the arthroscopist is the dorsal ulnar sensory nerve (DUSN). This nerve branches from the main ulnar nerve approximately 5 cm proximal to the wrist crease and courses subcutaneously over the dorsal-ulnar aspect of the wrist. It is notoriously susceptible to iatrogenic injury during the establishment of the 6R and 6U arthroscopic portals. Injury to the DUSN can result in devastating, recalcitrant neuromas or debilitating sensory deficits that overshadow the primary TFCC repair.
Additionally, the Extensor Carpi Ulnaris (ECU) tendon and its distinct subsheath lie in immediate proximity to the dorsal TFCC. The ECU subsheath is intimately blended with the dorsal radioulnar ligament. Iatrogenic disruption of this subsheath during portal placement or capsular repair can precipitate ECU subluxation, a condition that perfectly mimics TFCC pathology and leads to persistent post-operative ulnar-sided pain and snapping.
Relevant Osteology and Ulnar Variance
The osseous landmarks of the ulnar wrist serve as our navigational beacons. The distal radius provides the sigmoid notch for the TFCC's origin, while Lister's tubercle serves as a critical dorsal reference point for establishing the 3-4 portal. The distal ulna features the ulnar head, which articulates with the sigmoid notch, and the ulnar styloid, the primary insertion site for the superficial TFCC fibers.
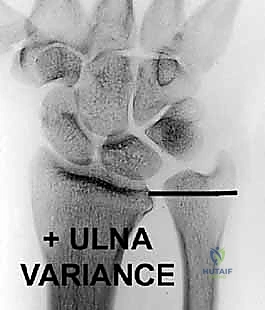
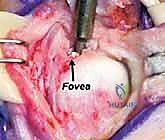
The fovea, nestled at the base of the ulnar styloid, is the true isometric center of rotation for the DRUJ and the critical insertion point for the deep fibers (ligamentum subcruentum) of the TFCC. Ulnar variance—the relative length of the distal ulna compared to the distal radius—plays a monumental role in TFCC biomechanics. Neutral variance dictates that the radius and ulna are flush.
Positive ulnar variance, where the ulna projects further distally, pathologically increases the axial load transmitted through the TFCC to the ulnar head. This morphological variant is the primary culprit in ulnocarpal impaction syndrome and significantly accelerates the degenerative cascade within the central articular disc. Conversely, negative ulnar variance unloads the TFCC but can predispose the wrist to Kienböck's disease due to altered radiocarpal load distribution.
Pathogenesis and Palmer Classification System
The pathogenesis of TFCC lesions is broadly dichotomized into acute traumatic events and chronic degenerative processes. The Palmer classification system, introduced in 1989, remains the universally accepted nomenclature for categorizing these injuries and guiding surgical strategy.
Traumatic Lesions (Palmer Class 1)
Traumatic TFCC disruptions (Class 1) typically afflict younger, active patients following a distinct mechanical insult. The classic mechanism involves a forceful extension and pronation moment applied to an axially loaded wrist, such as a FOOSH injury. Alternatively, extreme traction forces applied to the ulnar aspect of the wrist or violent resisted torque can precipitate traumatic avulsions.
- Class 1A (Central Tear): These are linear or stellate tears located in the avascular central horizontal portion of the articular disc, typically 2 to 3 mm medial to the radial attachment. Because they reside in the "white zone," they are incapable of healing and are treated with arthroscopic debridement.
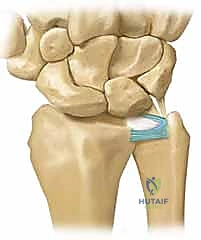
- Class 1B (Ulnar Avulsion): This represents a detachment of the TFCC from its peripheral ulnar insertion. This can occur as a pure soft-tissue avulsion from the fovea/styloid or in conjunction with an ulnar styloid basal fracture. Because this disrupts the primary stabilizers of the DRUJ, clinical instability is common. The robust blood supply in this region makes Class 1B lesions the classic indication for primary surgical repair.
- Class 1C (Distal Avulsion): These rare lesions involve the disruption of the volar ulnocarpal ligaments (ulnolunate and ulnotriquetral). They result in ulnar carpal instability and volar sag of the carpus, requiring complex open or arthroscopic reconstruction.
- Class 1D (Radial Avulsion): This involves the detachment of the TFCC from the sigmoid notch of the radius. It can present as an isolated disc tear or a catastrophic global avulsion involving the radioulnar ligaments, leading to profound DRUJ instability requiring transosseous reattachment.
Degenerative Lesions (Palmer Class 2)
Degenerative TFCC lesions (Class 2) represent an inevitable, age-related histological deterioration, frequently exacerbated by positive ulnar variance and chronic ulnocarpal impaction. The natural history follows a predictable, progressive cascade of attrition.
- Type 2A: Characterized by superficial wear and thinning of the central TFCC without full-thickness perforation.
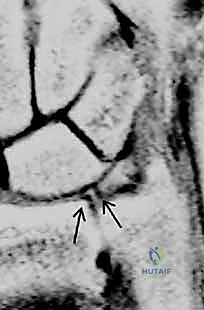
- Type 2B: Progression of TFC wear accompanied by early chondromalacia on the proximal pole of the lunate or the articular surface of the ulnar head.
- Type 2C: The hallmark of advanced degeneration, featuring a full-thickness, fibrillated perforation of the central articular disc.
- Type 2D: Central perforation with progressive chondromalacia, now complicated by an attritional tear of the lunatotriquetral (LT) interosseous ligament, leading to localized carpal instability.
- Type 2E: The end-stage of the degenerative cascade, encompassing all previous findings plus widespread ulnocarpal and DRUJ osteoarthritis. Management at this stage typically mandates salvage procedures such as a Darrach or Sauvé-Kapandji procedure, rather than isolated TFCC intervention.
Clinical Evaluation: History and Physical Examination
The diagnostic algorithm for TFCC pathology hinges on a meticulous, high-index-of-suspicion clinical evaluation. The myriad of overlapping structures in the ulnar wrist necessitates precise, localized examination techniques.
Patient History and Presentation
Patients with acute Class 1 injuries invariably recount a specific traumatic event, frequently describing a distinct "pop" or tearing sensation at the moment of impact. The predominant symptom is sharp, localized ulnar-sided wrist pain that is profoundly exacerbated by rotational activities, such as turning a doorknob, wringing out a towel, or lifting a heavy pan.
In contrast, patients with Class 2 degenerative lesions present with an insidious onset of dull, aching pain. This pain is often chronic, progressive, and associated with mechanical symptoms such as clicking, catching, or a sensation of grinding (crepitus) during forearm rotation. A thorough occupational and recreational history is vital, as repetitive axial loading and ulnar deviation (e.g., in carpenters or tennis players) strongly correlate with degenerative impaction syndromes.
Physical Examination and Provocative Testing
The physical examination must be systematic. Inspection may reveal localized ulnar swelling or a prominent ulnar head, suggesting DRUJ subluxation. Palpation is directed at isolating the exact point of maximal tenderness. The "Fovea Sign" is elicited by applying deep pressure in the soft spot between the ulnar styloid and the flexor carpi ulnaris tendon; exquisite pain here is highly sensitive and specific for foveal disruptions (Class 1B) or ulnocarpal ligament injuries.
Provocative testing is essential for assessing structural integrity. The TFCC Compression Test (or Ulnocarpal Stress Test) is performed by placing the wrist in ulnar deviation and applying an axial load while passively pronating and supinating the forearm. Elicitation of pain or a palpable mechanical click strongly suggests central TFCC pathology or ulnocarpal impaction.
Assessing DRUJ instability is the most critical component of the exam. The examiner stabilizes the distal radius and applies alternating dorsal and volar translational forces to the ulnar head. This "ballottement" test must be performed in neutral rotation, full pronation, and full supination, and strictly compared to the contralateral, uninjured wrist. A positive "piano key" sign—where the dorsally prominent ulna springs back after volar depression—indicates gross incompetence of the radioulnar ligaments.
Exhaustive Indications and Contraindications
Surgical decision-making in TFCC pathology requires a nuanced understanding of the patient's physiological demands, the specific morphological type of the tear, and the presence of concomitant osseous or ligamentous injuries.
Indications for Operative Intervention
Operative intervention is generally reserved for patients who have failed a rigorous trial of conservative management, including immobilization (Muenster cast or sugar-tong splint), NSAIDs, targeted physical therapy, and judicious corticosteroid injections. However, certain acute presentations warrant early surgical consideration.
Acute, traumatic peripheral tears (Palmer 1B, 1C, 1D) associated with demonstrable clinical DRUJ instability are prime indications for early surgical repair. Delaying intervention in these cases often leads to retraction of the ligamentous remnants, fibrosis, and a significantly lower success rate for anatomical restoration. Furthermore, TFCC tears occurring concomitantly with displaced distal radius fractures must be addressed; if the DRUJ remains unstable following rigid internal fixation of the radius, the TFCC must be explored and repaired.
For degenerative lesions (Palmer 2C, 2D), arthroscopic debridement is indicated when mechanical symptoms (catching, locking) are debilitating and refractory to conservative care. If these degenerative lesions are driven by symptomatic positive ulnar variance (ulnocarpal impaction), the TFCC debridement must be coupled with an ulnar shortening osteotomy or a wafer procedure to decompress the ulnar compartment and halt the degenerative cascade.
Contraindications to Surgical Repair
Contraindications to primary TFCC repair must be strictly respected to avoid catastrophic surgical failures.
| Contraindication Type | Specific Condition | Rationale |
|---|---|---|
| Absolute | Active localized or systemic infection | High risk of septic arthritis and systemic dissemination. |
| Absolute | End-stage DRUJ/Ulnocarpal Osteoarthritis (Palmer 2E) | Soft tissue repair will fail in the presence of advanced arthrosis; requires salvage arthroplasty or arthrodesis. |
| Absolute | Palmer Class 1A (Central) Tears | Avascular zone precludes biological healing; repair attempts will fail. Debridement is the standard of care. |
| Relative | Chronic (>6 months), retracted foveal tears | Severe tissue retraction and poor tissue quality may preclude primary repair, necessitating tendon graft reconstruction. |
| Relative | Uncorrected positive ulnar variance | Repairing a TFCC under excessive axial load without addressing the bony variance will inevitably lead to suture pull-out and re-rupture. |
| Relative | Medical comorbidities precluding anesthesia | Patient safety supersedes elective orthopedic intervention. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative preparation is the bedrock of successful TFCC surgery. The margin for error in wrist arthroscopy is measured in millimeters, demanding flawless setup and comprehensive imaging review.
Advanced Imaging and Pre-Operative Assessment
While standard posteroanterior, lateral, and oblique radiographs are mandatory to assess ulnar variance, DRUJ congruity, and rule out fractures, Magnetic Resonance Imaging (MRI) is the gold standard for soft-tissue evaluation. A high-resolution 3-Tesla MRI, preferably with intra-articular contrast (MR Arthrography), provides unparalleled visualization of the TFCC's intricate anatomy.
The surgeon must systematically review the MRI to identify the tear location (central vs. peripheral), assess the integrity of the radioulnar ligaments, and evaluate the foveal attachment. Furthermore, the MRI is scrutinized for concomitant pathology, such as lunatotriquetral ligament tears, chondral defects on the ulnar head, or ECU tendon subluxation, all of which will alter the surgical algorithm.
Operating Room Setup and Patient Positioning
The patient is positioned supine on the operating table with the operative extremity extended on a radiolucent hand table. Regional anesthesia (supraclavicular or axillary block) is preferred, providing excellent intraoperative muscle relaxation and post-operative analgesia. A well-padded pneumatic tourniquet is applied to the proximal arm.

Standard wrist arthroscopy requires vertical traction to distract the radiocarpal and midcarpal joints. The hand is secured in a sterile traction tower using Chinese finger traps applied to the index and middle fingers. Approximately 10 to 15 pounds of longitudinal traction is applied. The wrist should be positioned in neutral flexion/extension and slight ulnar deviation to optimize visualization of the TFCC and the ulnar compartment.
Equipment and Instrumentation
The arthroscopic equipment must be specifically tailored for the small joints of the wrist. A 2.7-mm or 1.9-mm arthroscope with a 30-degree angle of inclination is standard. A dedicated small-joint fluid management system is utilized, maintaining a low inflow pressure (typically 30-40 mmHg) to prevent massive fluid extravasation into the forearm compartments, a potentially limb-threatening complication.
Instrumentation includes a graduated arthroscopic probe, small-joint shavers (2.0 mm and 2.9 mm), radiofrequency ablation wands, and specialized TFCC repair sets (including outside-in spinal needles, inside-out suture shuttles, and all-inside anchor delivery systems). Fluoroscopy must be readily available in the operating room to verify anchor placement and confirm DRUJ reduction.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a TFCC repair is a highly technical endeavor requiring ambidextrous proficiency and an intimate knowledge of arthroscopic anatomy.
Diagnostic Arthroscopy and Portal Placement
The procedure commences with the establishment of standard radiocarpal portals. The 3-4 portal, located immediately distal to Lister's tubercle and between the 3rd and 4th extensor compartments, serves as the primary viewing portal. The 4-5 portal, or the 6R portal (radial to the ECU tendon), is established under direct intra-articular visualization using a spinal needle to ensure optimal trajectory and avoid iatrogenic cartilage injury.

Once access is gained, a systematic diagnostic tour is performed. The "Trampoline Test" is executed by pressing the arthroscopic probe against the central TFCC. A healthy TFCC will exhibit taut, resilient rebound (like a trampoline). A loss of this tension, resulting in a soft, boggy feel, is highly indicative of a peripheral detachment. The "Hook Test" involves placing the probe under the ulnar border of the TFCC and pulling radially; excessive laxity confirms a foveal avulsion.

Debridement Techniques for Central Lesions
For Palmer Class 1A or 2C central lesions, the goal is to excise the unstable, avascular flaps that are causing mechanical impingement, while meticulously preserving the critical peripheral stabilizing rim. Using a combination of a 2.0 mm or 2.9 mm oscillating shaver and a radiofrequency wand through the 4-5 or 6R portal, the torn edges are debrided back to a stable, smooth contour.
The surgeon must exercise extreme caution to avoid over-resection. Resecting more than the central 2-3 mm of the disc can inadvertently compromise the dorsal and volar radioulnar ligaments, iatrogenically converting a stable wrist into an unstable one. Following debridement, the DRUJ must be dynamically tested to ensure stability has not been compromised.
Arthroscopic Repair Techniques for Peripheral Tears
Peripheral tears (Class 1B) located in the vascularized zone are repaired using various suture techniques. For simple capsular detachments, an "outside-in" technique is frequently employed. A small incision is made just volar to the ECU tendon. Two spinal needles, loaded with PDS or non-absorbable suture, are passed through the wrist capsule and the peripheral rim of the TFCC under direct arthroscopic visualization.
The sutures are retrieved through the working portal, tied extracapsularly, and the knot is buried deep to the extensor retinaculum. Alternatively, "all-inside" techniques utilize specialized suture-passing devices to place horizontal mattress sutures directly through the TFCC and capsule, minimizing the risk of DUSN entrapment and reducing surgical time.

Open Repair and Foveal Reattachment
When arthroscopic evaluation reveals a deep foveal avulsion (often termed a "proximal" 1B tear or an Atzei Class 2/3 lesion), simple capsular suturing is biomechanically insufficient. The deep fibers (ligamentum subcruentum) must be anatomically reattached to the fovea to restore true DRUJ stability.

This can be achieved via an arthroscopically assisted technique or a formal open approach. In the arthroscopic method, the fovea is debrided of fibrous tissue down to bleeding bone using a burr through the distal radioulnar (DRUJ) portal. A transosseous tunnel is drilled from the ulnar cortex into the fovea. Sutures are passed through the TFCC, shuttled down the osseous tunnel, and tied over a cortical button on the ulnar shaft.
Alternatively, knotless suture anchors can be placed directly into the fovea under arthroscopic or fluoroscopic guidance. The sutures are passed through the deep TFCC fibers and tensioned, drawing the complex firmly down to its anatomical footprint.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, TFCC repair carries a distinct profile of potential complications. A comprehensive understanding of these risks is essential for informed patient consent and prompt intraoperative or postoperative mitigation.
Intraoperative Complications
The most devastating intraoperative complication is iatrogenic injury to the Dorsal Ulnar Sensory Nerve (DUSN). This typically occurs during the blind establishment of ulnar-sided portals (6R, 6U) or during the extracapsular tying of outside-in sutures. To mitigate this, blunt dissection with a hemostat down to the capsule is mandatory before introducing the trocar.

Cartilage scuffing of the ulnar head, lunate, or triquetrum is another frequent technical error, usually resulting from aggressive instrument insertion
Clinical & Radiographic Imaging Archive


