Arthroscopic Management of Triangular Fibrocartilage Complex Tears: Débridement and Foveal Repair
Key Takeaway
Arthroscopic management of triangular fibrocartilage complex (TFCC) tears requires precise portal placement and meticulous evaluation of the distal radioulnar joint. Central Palmer Class 1A lesions are treated with arthroscopic débridement, preserving a 2-mm peripheral rim to maintain biomechanical stability. Conversely, Class 1B foveal detachments necessitate transosseous or anchor-based repair to restore DRUJ kinematics. Concurrent ulnar styloid fractures and extensor carpi ulnaris tendon subluxations must be addressed simultaneously to ensure optimal functional outcomes.
Comprehensive Introduction and Patho-Epidemiology
The triangular fibrocartilage complex (TFCC) represents the primary static stabilizer of the distal radioulnar joint (DRUJ) and serves as a critical, load-bearing shock absorber for the ulnocarpal articulation. Functioning analogously to the meniscus of the knee, this intricate network of ligaments and fibrocartilage transmits approximately 20% of the axial compressive load from the carpus to the distal ulna, with the remaining 80% passing through the radiocarpal joint. The structural integrity of the TFCC is paramount for fluid, pain-free forearm rotation and gripping activities. Pathologic lesions of the TFCC are broadly categorized by the universally adopted Palmer classification system into acute traumatic injuries (Class 1) and chronic degenerative tears (Class 2), each presenting distinct clinical challenges and requiring highly specific surgical algorithms.
The epidemiology of TFCC pathology exhibits a bimodal distribution, reflecting both the traumatic and degenerative etiologies. Acute traumatic tears (Palmer Class 1) predominantly afflict younger, active individuals, particularly athletes engaged in racquet sports, gymnastics, or heavy manual labor. The classic mechanism of injury involves a sudden, high-energy axial load applied to an extended, pronated wrist, often combined with forced ulnar deviation. Conversely, degenerative tears (Palmer Class 2) are ubiquitous in the aging population, frequently presenting in the fifth to seventh decades of life. These lesions are intrinsically linked to ulnocarpal abutment syndrome, where a positive ulnar variance—either congenital or acquired secondary to distal radius fracture malunion—exerts chronic, repetitive shear stress across the central articular disc, leading to progressive attrition, perforation, and eventual chondromalacia of the ulnar head and lunate.
Over the past three decades, arthroscopic intervention has unequivocally supplanted open arthrotomy as the gold standard for both the definitive diagnosis and surgical management of TFCC pathology. The evolution of small-joint arthroscopy has provided surgeons with unprecedented, magnified visualization of the ulnocarpal joint, enabling precise identification of tear morphology that is frequently missed or underestimated by advanced imaging modalities. Central articular disc tears (Palmer Class 1A) are largely avascular and inherently lack healing potential, rendering them ideal candidates for meticulous arthroscopic débridement. In stark contrast, peripheral tears, particularly the biomechanically devastating ulnar-sided foveal detachments (Palmer Class 1B), occur within the well-vascularized periphery of the complex and demand rigid anatomical repair to restore DRUJ kinematics.
The overarching objective of surgical intervention is to alleviate ulnar-sided wrist pain while meticulously preserving or restoring the intricate biomechanics of the DRUJ. A paradigm shift in wrist arthroscopy has emphasized the critical distinction between superficial styloid attachments and deep foveal attachments. Failure to recognize and anatomically repair a deep foveal avulsion—often referred to as the "iceberg concept" of TFCC tears—will invariably result in persistent DRUJ instability, accelerated radioulnar arthrosis, and profound functional impairment. Consequently, modern orthopedic wrist surgeons must possess a masterful understanding of both arthroscopic resection techniques for central lesions and advanced transosseous or anchor-based repair techniques for peripheral detachments.
Detailed Surgical Anatomy and Biomechanics
A profound comprehension of the intricate microanatomy and biomechanics of the TFCC is an absolute prerequisite for successful arthroscopic management. The TFCC is not a singular structure but a heterogeneous complex comprising the central articular disc, the dorsal and volar radioulnar ligaments (RULs), the meniscus homologue, the ulnocarpal ligaments (ulnolunate and ulnotriquetral), and the extensor carpi ulnaris (ECU) tendon subsheath. The central articular disc is a biconcave, avascular fibrocartilaginous structure that articulates with the lunate and triquetrum distally and the ulnar head proximally. Its primary function is load distribution rather than stabilization. The true stabilizers of the DRUJ are the robust dorsal and volar radioulnar ligaments, which originate from the sigmoid notch of the radius and converge toward their ulnar insertions.
The vascular anatomy of the TFCC dictates its healing capacity and directly informs surgical decision-making. Microangiographic studies have definitively demonstrated that the blood supply to the TFCC is derived from the ulnar artery, the anterior interosseous artery, and the palmar and dorsal branches of the anterior interosseous artery. These vessels penetrate the peripheral margins of the complex, creating a vascularized zone that encompasses only the peripheral 10% to 20% of the articular disc. The central 80% and the radial attachment are completely avascular, nourished solely by synovial diffusion. Consequently, traumatic tears occurring in the central, avascular zone (Palmer 1A) are biologically incapable of healing, necessitating débridement. Conversely, tears at the ulnar periphery (Palmer 1B) possess robust vascularity and exhibit excellent healing potential when anatomically reduced and stabilized.
Biomechanically, the ulnar insertion of the radioulnar ligaments is highly complex and clinically critical. The RULs bifurcate into superficial and deep components. The superficial fibers attach to the tip and lateral aspect of the ulnar styloid, blending with the joint capsule. However, the deep fibers—collectively termed the ligamentum subcruentum—converge and insert into the fovea, a distinct anatomical depression located at the base of the ulnar styloid. Biomechanical sectioning studies have proven that the deep foveal fibers are the primary restraint to DRUJ translation in both pronation and supination. During forearm rotation, the dorsal and volar RULs experience dynamic tensioning; the dorsal RUL tightens in pronation, while the volar RUL tightens in supination. Disruption of the foveal attachment catastrophically uncouples the radius and carpus from the ulna, leading to multi-directional DRUJ instability.
The pathoanatomy of Palmer 1B lesions requires careful differentiation between superficial and deep disruptions. A patient may sustain a tear of the superficial fibers (styloid tip avulsion) while the deep foveal fibers remain intact, resulting in a clinically stable DRUJ that may only require conservative management or simple débridement of the unstable flap. However, a true foveal detachment—whether a purely ligamentous avulsion or an avulsion fracture of the styloid base—obliterates the critical stabilizing mechanism of the DRUJ. Furthermore, the ECU subsheath is intimately connected to the dorsal aspect of the TFCC. Severe traumatic forces that avulse the foveal attachment frequently propagate dorsally, tearing the ECU subsheath and leading to concomitant ECU tendon subluxation. The surgeon must evaluate and address both structures to achieve a comprehensive restoration of ulnar-sided wrist biomechanics.
Exhaustive Indications and Contraindications
The decision to proceed with arthroscopic débridement versus anatomical repair of the TFCC hinges upon a meticulous synthesis of the patient's clinical presentation, radiologic findings, and intraoperative arthroscopic assessment. Arthroscopic débridement is primarily indicated for Palmer Class 1A lesions—central, avascular tears that present with refractory ulnar-sided wrist pain, mechanical catching, or clicking, but crucially, exhibit a clinically and arthroscopically stable DRUJ. Débridement is also highly effective for symptomatic Palmer Class 2A and 2B degenerative tears, provided there is no advanced ulnocarpal abutment or severe chondromalacia that would necessitate a concurrent ulnar shortening osteotomy (USO) or the Wafer procedure. The goal of débridement is to excise the unstable, impinging flap of fibrocartilage while meticulously preserving the stabilizing peripheral rim.
Conversely, arthroscopic foveal repair is strictly indicated for Palmer Class 1B lesions characterized by a detachment of the deep radioulnar ligaments from the ulnar fovea, resulting in demonstrable DRUJ instability. Clinical indicators include a positive foveal sign, a positive DRUJ ballottement test with asymmetric translation compared to the contralateral wrist, and failure of a minimum of 6 to 12 weeks of conservative management (e.g., Muenster splinting, NSAIDs, corticosteroid injections). Intraoperatively, the indication for repair is confirmed by a positive "trampoline test" (loss of normal tension in the articular disc) or a positive "hook test" (the ability to easily retract the ulnar periphery of the TFCC radially with an arthroscopic probe).
Contraindications to isolated arthroscopic TFCC procedures must be rigorously respected to prevent catastrophic surgical failures. The most critical relative contraindication to an isolated foveal repair is the presence of a positive ulnar variance (ulna-plus variance). In an ulna-plus wrist, the prominent ulnar head exerts relentless shear and compressive forces against the repaired TFCC. Attempting an isolated soft-tissue repair in this biomechanically hostile environment will almost certainly result in suture cut-out, anchor pull-out, and recurrent tearing. In such scenarios, a concurrent ulnar shortening osteotomy is mandatory to decompress the ulnocarpal joint and protect the primary repair. Absolute contraindications include advanced radiocarpal or DRUJ osteoarthritis, active intra-articular infection, and severe medical comorbidities precluding anesthesia.
| Parameter | Indications | Contraindications |
|---|---|---|
| Arthroscopic Débridement (Palmer 1A) | - Symptomatic central flap tears - Mechanical catching/clicking - Stable DRUJ clinically and arthroscopically - Failed conservative management (3-6 months) |
- DRUJ instability (requires repair) - Advanced DRUJ osteoarthritis - Ulnocarpal abutment requiring bony decompression |
| Arthroscopic Foveal Repair (Palmer 1B) | - Acute or subacute foveal avulsion - Demonstrable DRUJ instability - Positive trampoline/hook test - Ulnar neutral or ulnar minus variance |
- Fixed, unaddressed positive ulnar variance - Fixed DRUJ subluxation/contracture - Complete loss of TFCC tissue quality - Active joint infection |
| Concurrent Ulnar Shortening Osteotomy | - Symptomatic ulnocarpal abutment - Positive ulnar variance > 2mm - Failed isolated TFCC repair - Degenerative Palmer Class 2C/2D tears |
- Negative ulnar variance - Advanced DRUJ arthritis (relative) - Non-compliant patient |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning for TFCC surgery begins with a masterful clinical examination designed to isolate ulnar-sided wrist pathology. The examiner must systematically palpate the ulnar fovea (the "fovea sign"), situated between the ulnar styloid, the flexor carpi ulnaris (FCU) tendon, and the volar surface of the ulnar head. Exquisite tenderness in this recess is highly sensitive for foveal disruption. The DRUJ ballottement test is performed by stabilizing the radius and translating the ulna dorsally and volarly; this must be assessed in neutral rotation, full pronation, and full supination. Asymmetric translation, particularly with a soft end-point, strongly correlates with deep radioulnar ligament insufficiency. Additionally, the ECU synergy test and evaluation for ECU tendon subluxation during active supination and ulnar deviation are critical, as ECU pathology frequently masks or accompanies TFCC tears.
Radiographic evaluation is paramount and must include meticulously positioned posteroanterior (PA), lateral, and zero-rotation PA views. The zero-rotation PA view, obtained with the shoulder abducted 90 degrees, elbow flexed 90 degrees, and forearm in neutral rotation, is the only reliable method for accurately measuring ulnar variance. The surgeon must template the degree of ulnar variance to determine if a concurrent ulnar shortening osteotomy is required. High-resolution 3-Tesla Magnetic Resonance Imaging (MRI), preferably utilizing a dedicated wrist coil, is the imaging modality of choice. MR arthrography, involving the injection of intra-articular gadolinium, significantly increases the sensitivity for detecting small central perforations and subtle foveal avulsions. The surgeon must scrutinize the coronal and axial sequences to evaluate the integrity of the ligamentum subcruentum and the presence of subchondral cystic changes in the ulnar head or lunate.
Patient positioning and operating room setup are critical elements that dictate the fluidity and safety of the arthroscopic procedure. The surgery is typically performed under regional anesthesia, utilizing a supraclavicular or axillary brachial plexus block, which provides excellent intraoperative analgesia and postoperative pain control. A pneumatic tourniquet is applied to the proximal brachium and inflated to 250 mmHg after exsanguination. The patient is positioned supine with the operative arm extended onto a radiolucent hand table. A dedicated wrist traction tower is assembled, and sterile finger traps are applied to the index and long fingers.
Traction is a fundamental component of wrist arthroscopy. Approximately 10 to 15 pounds of longitudinal traction is applied vertically to distract the radiocarpal and midcarpal joints, creating the necessary working space for arthroscopic instruments. Counter-traction is achieved via a padded strap placed across the distal humerus, securing the arm to the table. The surgeon must ensure that the traction vector aligns with the longitudinal axis of the forearm to prevent iatrogenic nerve traction injuries. Once traction is established, the bony landmarks—including the Lister tubercle, the extensor tendons, the ulnar head, and the ulnar styloid—are meticulously palpated and outlined with a sterile surgical marker to guide precise portal placement.
Step-by-Step Surgical Approach and Fixation Technique
Diagnostic Arthroscopy and Portal Placement
The procedure commences with the establishment of the standard radiocarpal portals. The 3-4 portal, located between the extensor pollicis longus (EPL) and the extensor digitorum communis (EDC), serves as the primary viewing portal. A #11 blade is used to incise the skin only, followed by blunt dissection with a small hemostat down to the radiocarpal capsule to avoid injuring the terminal branches of the posterior interosseous nerve or superficial extensor tendons. A 2.7-mm or 1.9-mm 30-degree arthroscope is introduced. A systematic diagnostic sweep is performed, evaluating the radioscaphocapitate ligament, the scapholunate interosseous ligament, the articular surfaces of the scaphoid and lunate, and finally, the TFCC.
The 6R portal, located radial to the ECU tendon, is established using an outside-in technique with an 18-gauge spinal needle under direct intra-articular visualization. This ensures the optimal trajectory for instrumentation without scoring the articular cartilage. The 6U portal, located ulnar to the ECU tendon, is frequently required for ulnocarpal instrumentation. Establishing the 6U portal demands extreme vigilance due to its intimate proximity to the dorsal sensory branch of the ulnar nerve (DSBUN). Blunt dissection down to the capsule is mandatory.
Arthroscopic Débridement of Central Tears (Class 1A)
For Palmer Class 1A lesions, a 2.0-mm or 2.9-mm full-radius suction shaver is introduced through the 6R portal. Hypertrophic synovitis, which frequently obscures the TFCC, is meticulously débrided. An arthroscopic probe is introduced to assess the tear morphology and perform the "trampoline test." A central flap tear will lack tension and frequently flip into the ulnocarpal joint, causing abutment.
The débridement is executed utilizing the shaver, arthroscopic punch forceps (biters), or a retrograde banana blade. The unstable, frayed margins of the central tear are systematically resected until a smooth, stable contour is achieved. The absolute critical mandate during this step is the preservation of the peripheral 2 millimeters of the TFCC. This peripheral rim contains the structurally vital dorsal and volar radioulnar ligaments. Over-resection into this peripheral zone will catastrophically compromise DRUJ stability, converting a stable Class 1A lesion into an iatrogenically unstable joint. Following débridement, the joint is thoroughly irrigated to evacuate all fibrocartilaginous debris.
Transosseous Foveal Repair (Nakamura Technique)
For Palmer Class 1B foveal detachments, the transosseous repair technique described by Nakamura provides an exceptionally robust, anatomical reattachment of the deep fibers.
The first step is the rigorous preparation of the foveal footprint. Viewing from the 3-4 portal, a small arthroscopic burr or shaver is introduced through the 6U or a direct foveal portal. The fovea is meticulously decorticated down to bleeding, healthy cancellous bone. This biological preparation is non-negotiable, as it stimulates the marrow elements necessary for ligament-to-bone healing.
Next, a 1.5-cm longitudinal incision is made over the ulnar border of the distal ulna, approximately 15 mm proximal to the tip of the ulnar styloid. The DSBUN is identified and carefully retracted. Using a specialized TFCC drill guide, a 1.2-mm Kirschner wire is advanced from the ulnar cortex, angled distally and radially, to emerge precisely at the center of the decorticated fovea. The trajectory is confirmed arthroscopically. The K-wire is then overdrilled with a 2.0-mm cannulated drill bit to create the transosseous tunnel.
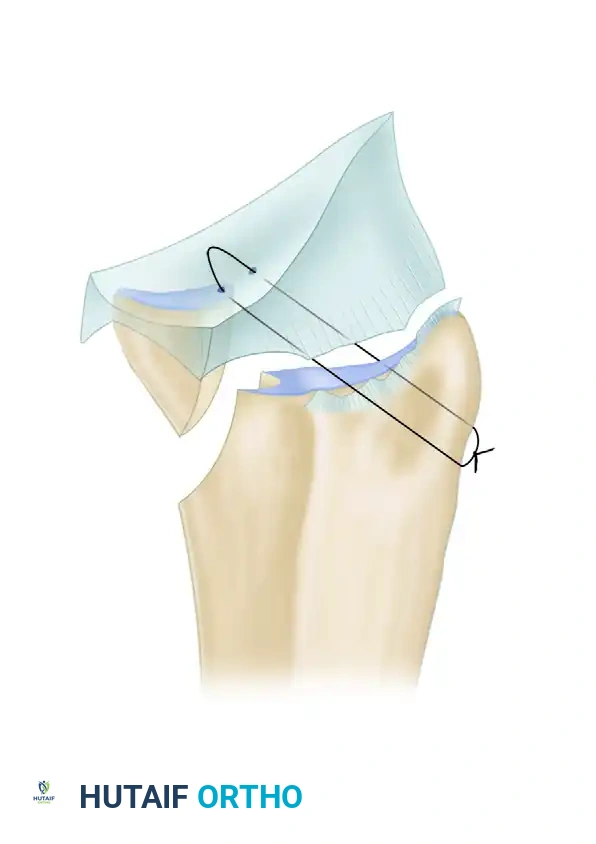
Suture passing is accomplished using an outside-in technique. A specialized suture lasso or a Tuohy needle is passed through the ulnar capsule, capturing a substantial bite of the detached volar radioulnar ligament and the peripheral TFCC rim. A non-absorbable, high-tensile strength suture (e.g., #2-0 FiberWire) is deployed into the joint and retrieved out through the transosseous tunnel using a wire loop or grasping device. This process is repeated to capture the dorsal radioulnar ligament, creating a horizontal mattress configuration across the TFCC periphery.
The final and most critical step is tensioning and securing the repair. The traction is released, and the forearm is placed in neutral rotation. The suture limbs, exiting the ulnar cortical tunnel, are tensioned. The surgeon arthroscopically verifies the reduction of the TFCC down to the foveal footprint and confirms the restoration of the "trampoline effect." The sutures are then tied securely over the ulnar cortical bone bridge or utilizing a low-profile titanium cortical button to prevent suture cut-through in osteopenic bone.
Complications, Incidence Rates, and Salvage Management
Despite the minimally invasive nature of arthroscopic TFCC surgery, the complex anatomy of the ulnocarpal joint renders the procedure susceptible to a spectrum of formidable complications. Neurological injury is the most frequently cited complication, with the dorsal sensory branch of the ulnar nerve (DSBUN) being exquisitely vulnerable during the establishment of the 6U portal and the ulnar approach for transosseous drilling. Incidence rates of DSBUN neuropraxia range from 2% to 5%, while frank transection or symptomatic neuroma formation occurs in less than 1% of cases. Prevention relies entirely on meticulous, blunt soft-tissue dissection and the avoidance of blind trocar insertion. If a painful neuroma develops, salvage management requires surgical exploration, neuroma excision, and burying the proximal nerve stump deep into the pronator quadratus muscle belly.
Iatrogenic DRUJ instability is a catastrophic complication that arises primarily from the over-resection of the central articular disc during a débridement procedure. If the surgeon inadvertently violates the peripheral 2-mm rim, the dorsal and volar radioulnar ligaments are compromised. The incidence of this technical error is difficult to quantify but is universally recognized as a hallmark of inadequate surgical experience. Salvage management for iatrogenic instability is highly complex and typically necessitates an open, anatomically based ligament reconstruction, such as the Adams-Berger procedure, utilizing a palmaris longus or plantaris tendon autograft routed through the radius and ulna to recreate the radioulnar ligaments.
Repair failure and recurrent tearing represent significant challenges, particularly following foveal reattachment. The primary etiology of repair failure is the failure to recognize and address a positive ulnar variance preoperatively. If an isolated foveal repair is performed in an ulna-plus wrist, the unrelenting biomechanical shear forces will inevitably lead to suture pull-out or anchor dislodgement, with failure rates approaching 30% to 40% in poorly selected patients. Salvage in these scenarios mandates a revision repair combined with a concurrent ulnar shortening osteotomy to definitively decompress the ulnocarpal joint.
Arthrofibrosis and profound rotational stiffness of the forearm are common postoperative sequelae, particularly following prolonged immobilization for foveal repairs. The incidence of clinically significant stiffness ranges from 10% to 15%. Strict adherence to phased rehabilitation protocols is essential to mitigate this risk. If severe stiffness persists beyond 6 months despite aggressive therapy, an arthroscopic capsular release and manipulation under anesthesia may be warranted.
| Complication | Incidence Rate | Prevention Strategy | Salvage Management |
|---|---|---|---|
| DSBUN Neuropraxia / Neuroma | 2% - 5% | Blunt dissection for 6U portal; protect nerve during ulnar drilling. | Observation for neuropraxia; Neuroma excision and deep muscle burying. |
| Iatrogenic DRUJ Instability | < 2% | Strictly preserve the peripheral 2mm rim during central débridement. | Open anatomic DRUJ reconstruction (e.g., Adams-Berger technique). |
| Repair Failure / Suture Pull-out | 5% - 10% (Higher if + variance missed) | Address positive ulnar variance with concurrent USO; use robust mattress sutures. | Revision repair + Ulnar Shortening Osteotomy; consider tendon graft. |
| Arthrofibrosis / Rotational Stiffness | 10% - 15% | Avoid over-tensioning the repair; adhere to early protected motion protocols. | Aggressive hand therapy; Arthroscopic capsular release if refractory. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following TFCC surgery must strike a delicate, scientifically grounded balance between protecting the healing soft tissues and preventing debilitating arthrofibrosis. The trajectory of rehabilitation is fundamentally dictated by the nature of the surgical intervention—a simple débridement allows for accelerated mobilization, whereas a structural foveal repair demands rigorous, phased protection of the healing ligament-to-bone interface.
For patients undergoing isolated arthroscopic débridement (Palmer Class 1A), the postoperative course is relatively expeditious. Immediately following the procedure, the wrist is immobilized in a bulky, volar short-arm splint. At the 10- to 14-day mark, the patient returns for portal suture removal. At this juncture, the splint is transitioned to a removable, custom-molded thermoplastic splint. Protected, active range-of-motion (ROM) exercises for wrist flexion, extension, pronation, and supination are initiated immediately. The patient is instructed to wear the splint between exercise sessions and during sleep for an additional 2 to 3 weeks. Strenuous pronation-supination under load, such as turning screwdrivers or wringing out towels, must be strictly avoided for the first 4 weeks. Unrestricted activity and return to heavy labor are typically permitted by 6 weeks postoperatively, contingent upon the restoration of painless grip strength.
Conversely, the rehabilitation following a transosseous foveal repair (Palmer Class 1B) is protracted and demands strict adherence to a four-phase protocol. Phase 1 (0 to 4 Weeks): The primary objective is absolute protection of the foveal repair. The patient is immobilized in a Muenster-style cast or a long-arm sugar-tong splint. This specific immobilization is critical as it locks the forearm in neutral rotation, completely eliminating the dynamic tensioning of the radioulnar ligaments that occurs during pronation and supination, while allowing limited elbow flexion and extension. Digital range of motion is aggressively encouraged to prevent intrinsic hand stiffness and manage edema.
Phase 2 (4 to 8 Weeks): The long-arm immobilization is discontinued, and the patient is transitioned to a custom short-arm Munster splint or a well-fitted wrist widget that provides DRUJ stability. Active-assisted range of motion (AAROM) for wrist flexion and extension is initiated. Gentle, gravity-eliminated pronation and supination are introduced under the strict supervision of a certified hand therapist. The patient is cautioned against pushing through pain at the extremes of rotation. Loaded rotation and power gripping remain strictly prohibited, as the ligament-to-bone healing is still in the fragile remodeling phase.
Phase 3 (8 to 12 Weeks): The protective splinting is gradually weaned and discontinued for activities of daily living. Progressive strengthening exercises are initiated, with a specific focus on rehabilitating the dynamic stabilizers of the ulnocarpal joint. Isotonic and isometric strengthening of the extensor carpi ulnaris (ECU) and the pronator quadratus (PQ) are emphasized, as these muscles play a synergistic role in unloading the TFCC and stabilizing the DRUJ. Proprioceptive neuromuscular facilitation (PNF) techniques are incorporated to restore the sensorimotor control of the wrist.
Phase 4 (12+ Weeks): This phase focuses on work conditioning and return-to-play criteria. Unrestricted heavy manual labor, racquet sports, or contact sports are typically delayed until 4 to 6 months postoperatively. Clearance for these activities is strictly contingent upon the clinical demonstration of symmetric, pain-free DRUJ stability, full restoration of the pronation-supination arc, and grip strength that is at least 85% of the contralateral, uninjured extremity.
Summary of Landmark Literature and Clinical Guidelines
The contemporary arthroscopic management of TFCC pathology is deeply rooted in decades of rigorous biomechanical research and evolving clinical classifications. The foundational bedrock of TFCC literature remains the seminal work by Palmer in 1989, which delineated the anatomical boundaries of the complex and established the universally utilized classification system dividing lesions into traumatic (Class 1) and degenerative (Class 2) etiologies. While the Palmer classification remains the standard for initial diagnosis, its limitations in guiding specific surgical treatments for peripheral tears prompted further academic evolution.
In recent years, the Atzei classification has emerged as a critical algorithm for the management of peripheral (Palmer 1B) tears. Atzei categorized ulnar-sided tears into five distinct classes based on the integrity of the superficial and deep foveal fibers, as assessed arthroscopically. Atzei Class 1 represents a tear of the superficial fibers with an intact foveal attachment (stable DRUJ), manageable by simple débridement or capsular suturing. Atzei Class 2 and 3 represent partial and complete foveal detachments, respectively, mandating anatomical foveal repair. This classification has fundamentally shifted the surgical mindset, emphasizing that not
