Mastering Limited Wrist Arthrodesis: An Intraoperative Guide to Four-Corner, STT, and LT Fusions

Key Takeaway
Welcome to the operating theater, fellows. Today, we're performing limited wrist arthrodesis, a crucial salvage procedure for debilitating wrist pain. This masterclass will guide you through the intricate steps of Four-Corner, Scaphoid-Trapezium-Trapezoid (STT), and Lunotriquetral (LT) fusions. We'll cover comprehensive anatomy, meticulous intraoperative execution, critical pearls, and effective complication management, ensuring you master these motion-sparing techniques.
Comprehensive Introduction and Patho-Epidemiology
Limited wrist arthrodesis represents a cornerstone in the armamentarium of the reconstructive hand and upper extremity surgeon. These procedures are not mere temporizing measures; they are sophisticated, motion-sparing salvage operations engineered to eradicate pain while preserving functional kinematics in the face of progressive carpal collapse. The fundamental philosophy underlying these techniques is the selective ablation of arthritic or irreducibly unstable articulations, coupled with the preservation of unaffected joints—most critically, the radiolunate articulation. By fusing specific carpal bones, we alter the load-bearing mechanics of the wrist, transferring forces away from degenerative foci and restoring a stable, albeit modified, intercalated segment.
The pathogenesis of conditions necessitating limited wrist arthrodesis typically follows a predictable, biomechanically driven cascade of degeneration. The most common etiology is Scapholunate Advanced Collapse (SLAC), a sequela of untreated scapholunate interosseous ligament (SLIL) incompetence. When the SLIL fails, the scaphoid flexes and pronates, while the lunate extends, resulting in a Dorsal Intercalated Segment Instability (DISI) deformity. This uncoupling disrupts the synchronous kinematics of the proximal carpal row. The flexed scaphoid presents a smaller, incongruous radius of curvature to the elliptical scaphoid fossa of the distal radius, drastically increasing contact stresses. Over time, this abnormal loading invariably leads to progressive articular cartilage degradation, beginning at the radial styloid and advancing across the radioscaphoid joint, before ultimately involving the capitolunate articulation.
Similarly, Scaphoid Nonunion Advanced Collapse (SNAC) follows a parallel degenerative trajectory. In the setting of an ununited scaphoid fracture, the distal pole flexes with the distal carpal row, while the proximal pole remains attached to the lunate, often extending. The incongruity at the radioscaphoid joint and the midcarpal joint leads to a predictable pattern of arthrosis. Other etiologies, such as chronic perilunate dislocations, midcarpal instability, and crystalline arthropathies like Calcium Pyrophosphate Deposition (CPPD) disease, can also precipitate these degenerative patterns. It is paramount to recognize that the radiolunate joint is uniquely spared in these non-inflammatory conditions. The spherical nature of the lunate fossa and the congruent proximal articular surface of the lunate allow for concentric load distribution, protecting this joint from the shear forces that decimate the radioscaphoid articulation. This anatomical idiosyncrasy is the biological foundation upon which procedures like the four-corner arthrodesis are built.
Epidemiologically, the burden of post-traumatic wrist osteoarthritis is significant, predominantly affecting young, active, and working-age populations. The natural history of untreated SLAC and SNAC wrists is progressive deterioration, with patients typically presenting with debilitating radial-sided wrist pain, weakness in grip strength, and a diminishing arc of motion 5 to 10 years following the initial traumatic insult. Understanding this patho-epidemiology is critical for the orthopaedic surgeon; early recognition of carpal instability can allow for soft-tissue reconstruction, but once the threshold of irreversible articular wear is crossed, limited arthrodesis becomes the definitive reconstructive pathway.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of carpal anatomy and its complex biomechanical interplay is the prerequisite for executing any limited wrist arthrodesis. The carpus is an intricate, highly constrained mechanism composed of eight bones arranged in two functional rows, lacking any direct tendinous insertions. Its stability and kinematics are entirely dependent on articular congruity and a robust network of intrinsic and extrinsic ligaments. The proximal row (scaphoid, lunate, triquetrum) functions as an intercalated segment, moving passively in response to forces transmitted from the distal row (trapezium, trapezoid, capitate, hamate) and the surrounding musculotendinous units.
The ligamentous anatomy of the wrist can be broadly categorized into volar and dorsal complexes. Volarly, the robust extrinsic ligaments, such as the radioscaphocapitate (RSC), long radiolunate (LRL), and short radiolunate (SRL) ligaments, provide critical static stability. The RSC ligament is particularly important; during a scaphoid excision for a four-corner fusion, meticulous care must be taken not to violate this volar structure, as it acts as a crucial sling preventing ulnar translation of the carpus. Dorsally, the anatomy is defined by the dorsal radiocarpal (DRC) ligament and the dorsal intercarpal (DIC) ligament. These structures form a lateral "V" configuration that stabilizes the proximal row against volar subluxation. Surgical approaches must respect these ligaments; a ligament-sparing capsulotomy, such as the Berger approach, meticulously splits the capsule in line with these fibers to preserve their stabilizing function postoperatively.
Neurovascular considerations are paramount during dorsal approaches to the carpus. The dorsal extensor retinaculum is divided into six compartments. The surgical interval of choice for central carpal exposure is typically between the third compartment, containing the Extensor Pollicis Longus (EPL), and the fourth compartment, containing the Extensor Digitorum Communis (EDC) and Extensor Indicis Proprius (EIP). Transposition of the EPL is routinely performed to prevent postoperative tendon rupture secondary to attrition against underlying hardware or irregular bone contours. Radially, the superficial branch of the radial nerve (SBRN) and the lateral antebrachial cutaneous nerve present significant hazards; their injury can result in intractable neuromas. Proximally, the posterior interosseous nerve (PIN) traverses the floor of the fourth extensor compartment to innervate the dorsal capsule. While deliberate neurectomy of the PIN is sometimes performed as an adjunct for pain relief, inadvertent damage should be avoided during initial dissection.
Biomechanically, limited wrist arthrodeses fundamentally alter force transmission across the radiocarpal and midcarpal joints. In a normal wrist, approximately 80% of the axial load is transmitted through the radius, with the scaphoid bearing roughly 50% and the lunate 30%. By excising the scaphoid and fusing the capitate, hamate, lunate, and triquetrum (four-corner fusion), the load transmission is entirely redirected through the radiolunate articulation. Remarkably, biomechanical studies have demonstrated that the radiolunate joint is capable of accommodating this increased load without rapid degeneration, provided the lunate is anatomically reduced out of its extended (DISI) posture prior to fusion. Failure to correct lunate extension results in dorsal impingement and abnormal stress concentration on the dorsal rim of the lunate fossa, precipitating early failure and persistent pain.
Exhaustive Indications and Contraindications
The decision to proceed with a limited wrist arthrodesis hinges on a meticulous clinical evaluation and rigorous radiographic staging. The classic presentation is a patient with chronic, activity-related wrist pain, localized predominantly to the dorsal-radial aspect, accompanied by a measurable loss of grip strength and range of motion. Physical examination must be systematic. The Finger Extension Test is highly sensitive for active radiocarpal or midcarpal pathology; resisted active extension of the fingers with the wrist in passive flexion exacerbates pain by loading the inflamed dorsal capsule and degenerative joints. Palpation of the anatomic snuffbox and the triscaphe (STT) joint provides precise localization of arthrosis, differentiating between radioscaphoid wear and isolated STT joint degeneration.
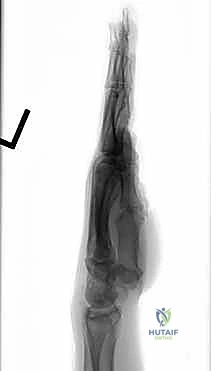
Radiographic evaluation is the definitive roadmap for surgical decision-making. A standard series including posteroanterior (PA), lateral, oblique, and scaphoid views is mandatory. The Watson and Ballet classification for SLAC wrist remains the gold standard for staging. Stage I involves arthrosis limited to the radial styloid-scaphoid articulation. Stage II exhibits progressive wear involving the entire radioscaphoid fossa. Stage III is characterized by proximal migration of the capitate with arthrosis between the capitate and the lunate. Crucially, in all three stages, the radiolunate joint remains pristine. A four-corner arthrodesis with scaphoid excision is the procedure of choice for Stage II and Stage III SLAC/SNAC wrists. Isolated STT fusion is indicated for localized STT arthrosis or as an alternative for early Stage II SLAC wrists to stabilize the scaphoid, though it has largely been supplanted by proximal row carpectomy or four-corner fusion due to a higher complication profile. Lunotriquetral (LT) fusion is reserved for chronic, symptomatic LT instability that has failed soft-tissue reconstruction, presenting with ulnar-sided wrist pain and a positive LT shuck test.
Contraindications must be rigorously respected to prevent catastrophic surgical failures. The absolute prerequisite for a four-corner or STT fusion is a pristine, cartilaginous radiolunate joint. Any evidence of radiolunate arthrosis, which is common in inflammatory arthritides like rheumatoid arthritis or severe advanced crystalline arthropathy, strictly contraindicates these limited fusions, mandating a total wrist arthrodesis instead. Furthermore, significant ulnar variance or concurrent distal radioulnar joint (DRUJ) pathology must be identified; while not absolute contraindications to limited carpal fusion, they require simultaneous surgical management (e.g., ulnar shortening osteotomy or Darrach procedure) to achieve a comprehensive, pain-free result.
| Parameter | Indications for Limited Wrist Arthrodesis | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Four-Corner Fusion | SLAC Stage II/III; SNAC Stage II/III; Chronic perilunate dislocation; Midcarpal instability. | Radiolunate joint arthrosis; Inflammatory arthritis (e.g., Rheumatoid); Active infection. | Severe osteopenia; Non-compliant patient; Heavy manual laborer (consider total fusion). |
| STT Fusion | Isolated STT osteoarthritis; Early SLAC (controversial); Kienböck's disease (stage IIIa, to unload lunate). | Radioscaphoid arthrosis; Scapholunate advanced collapse (Stage II+); Radiolunate arthrosis. | Advanced age; Pre-existing severe limitation in wrist flexion/extension. |
| LT Fusion | Chronic, symptomatic LT instability failing conservative/soft-tissue repair; Isolated LT arthrosis. | Diffuse carpal arthrosis; Ulnar impaction syndrome (unless treated concurrently). | Significant midcarpal arthrosis; Uncorrected positive ulnar variance. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning separates the master surgeon from the technician. The process begins with a comprehensive review of advanced imaging. While high-quality plain radiographs are sufficient for staging SLAC/SNAC wrists, a computed tomography (CT) scan is invaluable for assessing bone stock, identifying occult cystic changes within the lunate or capitate, and precisely evaluating the extent of STT or LT joint involvement. Magnetic resonance imaging (MRI) is rarely necessary for degenerative conditions but can be useful if avascular necrosis (e.g., Kienböck's or Preiser's disease) is suspected as the primary etiology.
Templating is a critical step, particularly when utilizing rigid internal fixation such as dorsal circular plates. Using digital templating software on scaled PA radiographs, the surgeon must determine the appropriate plate size that will adequately capture the capitate, hamate, lunate, and triquetrum without impinging on the dorsal rim of the radius during wrist extension. The position of the screws must be planned to ensure robust purchase in the dense subchondral bone while avoiding penetration into the preserved radiolunate or midcarpal articulations. If Kirschner wires (K-wires) or headless compression screws are chosen, the trajectory of the hardware should be mapped to optimize compression across the decorticated joint surfaces while maintaining the corrected anatomic alignment of the lunate.
Patient positioning and operating room setup must be standardized to facilitate seamless execution. The patient is placed supine with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. It is imperative that the hand table allows for unimpeded, multi-planar fluoroscopic imaging throughout the procedure. The C-arm should be positioned parallel to the table, entering from the distal or lateral aspect, allowing the surgeon to obtain perfect PA and lateral views without physically manipulating the patient's arm out of the sterile field.
Anesthesia typically involves a regional brachial plexus block (axillary or supraclavicular) combined with intravenous sedation or general anesthesia. The regional block provides excellent intraoperative muscle relaxation, essential for reducing chronic carpal deformities, and affords profound postoperative analgesia, facilitating early discharge and significantly improving patient satisfaction. Prior to inflation of the tourniquet, the limb is exsanguinated with an Esmarch bandage. The surgeon must verify that all specialized equipment, including high-speed burrs, specific plate sets, variable-pitch headless screws, and K-wires of varying diameters (0.045 and 0.062 inches), are readily available in the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
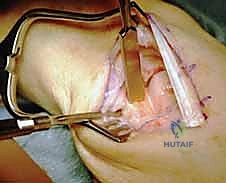
Dorsal Approach and Capsulotomy
The procedure commences with a dorsal longitudinal incision, approximately 6 to 8 centimeters in length, centered slightly ulnar to Lister's tubercle.
Careful subcutaneous dissection is performed to identify and protect the dorsal sensory branches of the radial and ulnar nerves, as well as the superficial venous network. The dorsal extensor retinaculum is exposed. The third extensor compartment is incised longitudinally, and the Extensor Pollicis Longus (EPL) tendon is mobilized and retracted radially. The septum separating the third and fourth compartments is then released, allowing the Extensor Digitorum Communis (EDC) and Extensor Indicis Proprius (EIP) tendons to be retracted ulnarly. This exposes the dorsal radiocarpal capsule.
A ligament-sparing capsulotomy is then executed. The Mayo (Berger) approach is preferred: an initial incision is made in line with the dorsal intercarpal (DIC) ligament, starting from the triquetrum and extending radially toward the scaphoid. A second incision connects to the first, reflecting the capsule proximally as a radially based triangular flap, following the fibers of the dorsal radiocarpal (DRC) ligament. This meticulous exposure preserves the intrinsic stabilizing structures of the wrist.

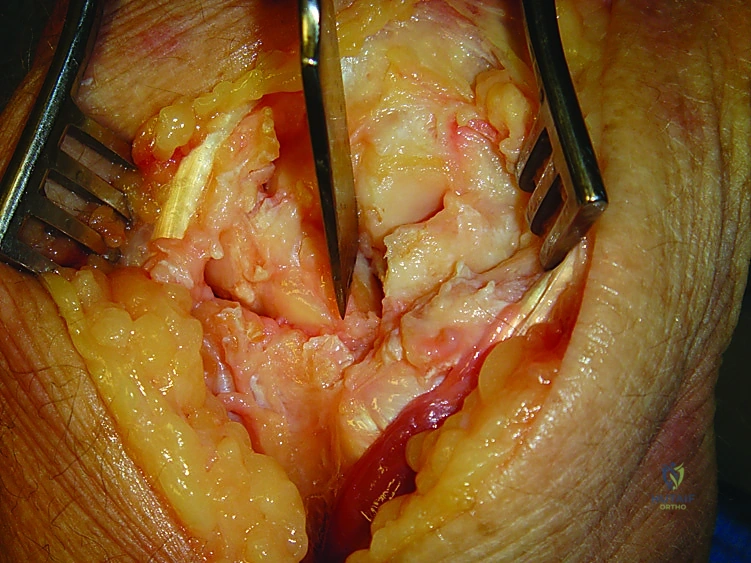
Upon entering the joint, the absolute first step is the direct visual inspection of the radiolunate articulation. The lunate fossa and the proximal lunate must demonstrate pristine, glistening hyaline cartilage. If significant eburnation or full-thickness cartilage loss is encountered, the limited arthrodesis is aborted, and the surgeon must pivot to a total wrist fusion.
Scaphoid Excision and Joint Preparation
Once the radiolunate joint is confirmed to be viable, attention is turned to the scaphoid. Complete excision is mandatory in a four-corner fusion to decompress the radial column and eliminate the pain generator.
The scaphoid is often fragmented in advanced SNAC wrists or severely sclerotic in SLAC wrists. A threaded K-wire can be inserted into the scaphoid to act as a joystick. Using a combination of a scalpel, small osteotomes, and a rongeur, the scaphoid is excised piecemeal.

Extreme caution must be exercised during the volar dissection to avoid violating the radioscaphocapitate (RSC) ligament, which lies immediately palmar to the scaphoid waist. Disruption of the RSC ligament will lead to catastrophic ulnar translation of the carpus postoperatively.
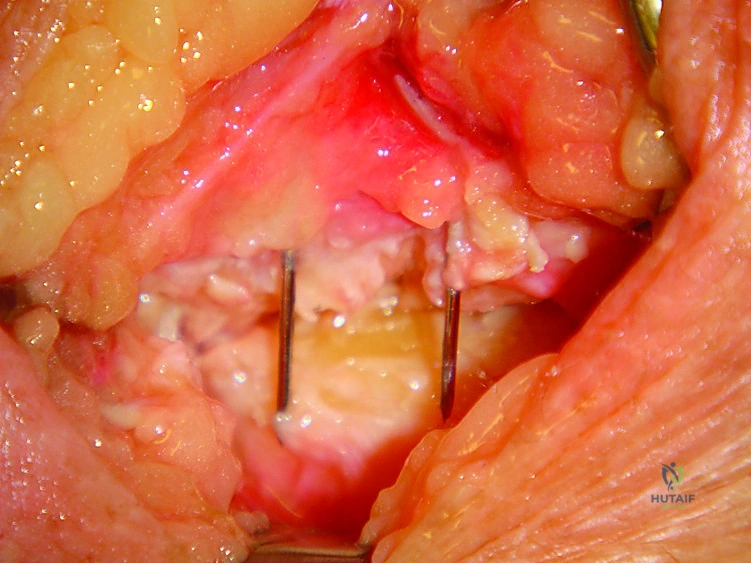
Following scaphoid excision, the articulations between the capitate, hamate, lunate, and triquetrum (the CHLT complex) must be meticulously prepared for arthrodesis.

Using a high-speed burr under continuous saline irrigation to prevent thermal necrosis, the articular cartilage and subchondral bone plate are removed down to healthy, bleeding cancellous bone.
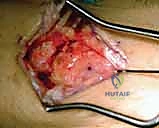
The decortication must be thorough, encompassing the capitolunate, capitohamate, triquetrohamate, and lunotriquetral joints. The goal is to create broad, flat, highly vascularized surfaces that will interdigitate securely.
Four-Corner Arthrodesis Execution
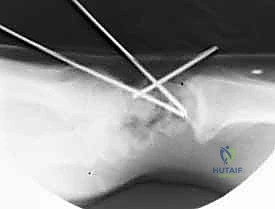
With the joints prepared, the critical step of carpal reduction is performed. In SLAC/SNAC wrists, the lunate is typically fixed in a DISI (extended) posture. It is imperative to reduce the lunate out of extension to achieve a neutral capitolunate alignment. A 0.062-inch K-wire is driven dorsally into the lunate to serve as a joystick, flexing the lunate into a neutral position relative to the radius. Simultaneously, the capitate is translated dorsally and reduced onto the lunate.

Autologous cancellous bone graft is essential for achieving a high union rate. This graft is typically harvested from the distal radius through the same dorsal incision, utilizing a small cortical window at the level of Lister's tubercle.

The cancellous bone is densely packed into the interstices of the decorticated CHLT joints.
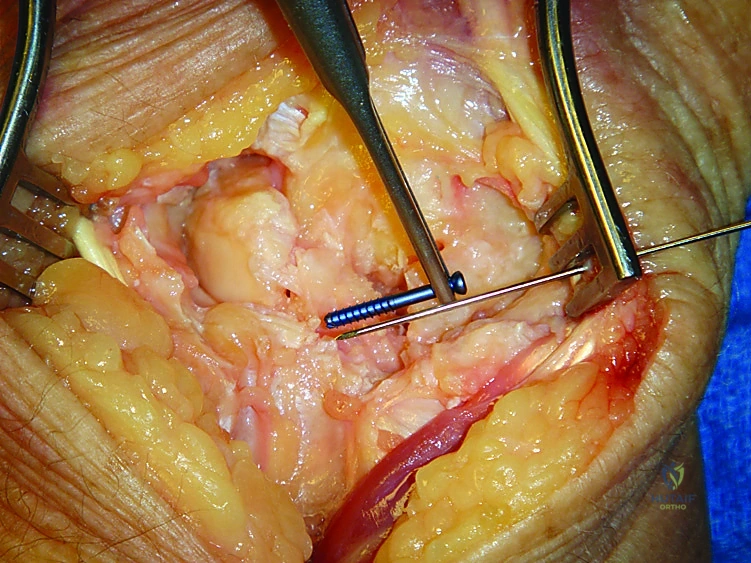
Fixation can be achieved via multiple modalities. If utilizing Kirschner wires, a minimum of two 0.045-inch or 0.062-inch K-wires are driven from the capitate into the lunate, and additional wires are passed transversely from the triquetrum into the lunate and capitate.

Alternatively, dorsal circular plates specifically designed for four-corner fusions provide rigid, low-profile fixation.

The plate is centered over the four-corner junction. The lunate screw is placed first to capture the reduced lunate, followed by the capitate screw to compress the capitolunate joint. Screws are then sequentially placed into the hamate and triquetrum.

Intraoperative fluoroscopy is utilized continuously to verify hardware placement, ensure no screws have penetrated the radiolunate joint, and confirm the restoration of the carpal height and alignment.
Scaphotrapeziotrapezoid (STT) Arthrodesis Execution
For an isolated STT fusion, a more radial dorsal incision is utilized, taking extreme care to protect the superficial radial nerve. The STT joint is exposed by incising the capsule radially to the EPL tendon.

The articular surfaces of the distal scaphoid, trapezium, and trapezoid are decorticated using a high-speed burr or small rongeurs.
It is critical not to alter the scaphoid's length or relationship to the radius during this decortication. The scaphoid must be pinned in its anatomic position—typically 45 degrees of flexion relative to the longitudinal axis of the radius.

Distal radius bone graft is packed into the decorticated spaces. Fixation is most commonly achieved with multiple K-wires or headless compression screws driven from the trapezium and trapezoid proximally into the scaphoid.
Lunotriquetral (LT) Arthrodesis Execution
LT fusion targets isolated ulnar-sided instability. The approach is slightly more ulnar, utilizing the 4-5 or 5-6 extensor compartment interval. The dorsal radioulnar and dorsal intercarpal ligaments are carefully elevated to expose the LT joint.
The LT interosseous ligament is excised, and the opposing articular surfaces of the lunate and triquetrum are thoroughly decorticated down to bleeding bone.

The triquetrum is reduced anatomically onto the lunate, correcting any volar intercalated segment instability (VISI) deformity. Bone graft is interposed, and compression is achieved using two parallel headless compression screws or K-wires directed from the ulnar aspect of the triquetrum into the lunate.

Following rigid fixation of any of these limited arthrodeses, the dorsal capsule is meticulously repaired to restore dorsal stability. The extensor retinaculum is repaired over the EDC tendons, leaving the EPL transposed subcutaneously. The skin is closed, and a bulky plaster splint is applied in neutral wrist extension.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, limited wrist arthrodeses carry a distinct profile of potential complications. The most formidable complication is nonunion, which occurs at varying rates depending on the specific joints fused and the fixation method utilized. In four-corner fusions, the capitolunate joint is the most frequent site of nonunion, occurring in approximately 3% to 10% of cases. Nonunions are often poorly tolerated, presenting with persistent pain, swelling, and progressive hardware failure. The etiology of nonunion is multifactorial, including inadequate decortication, thermal necrosis from aggressive burring, insufficient bone grafting, or failure to achieve rigid mechanical stability.
Hardware-related complications are particularly prevalent when utilizing dorsal circular plates. Impingement of the plate on the dorsal rim of the distal radius during wrist extension can cause significant pain and restrict the postoperative arc of motion. This incidence can be as high as 15% to 20% in some series, often necessitating secondary procedures for hardware removal once osseous union is confirmed. Furthermore, prominent K-wires can cause skin irritation, pin-tract infections, or iatrogenic tendon ruptures if they migrate or are left protruding too far dorsally.
Complex Regional Pain Syndrome (CRPS) is a devastating complication that can follow any wrist surgery, characterized by disproportionate pain, autonomic dysfunction, and severe stiffness. Its incidence following limited wrist arthrodesis is estimated between 2% and 5%. Early recognition and aggressive multimodal management, including sympathetic nerve blocks and intensive hand therapy, are critical to prevent permanent disability. If a limited arthrodesis ultimately fails due to intractable nonunion, progressive radiolunate arthrosis, or persistent unexplained pain, the definitive salvage procedure is conversion to a total wrist arthrodesis.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Nonunion (Capitolunate) | 3% - 10% | Inadequate decortication; poor bone graft; smoking; unstable fixation. | Revision arthrodesis with structural bone graft; Conversion to Total Wrist Arthrodesis if bone loss is severe. |
| Hardware Impingement | 10% - 20% (with plates) | Oversized dorsal plate; inadequate countersinking; improper distal radius clearance. | Hardware removal post-union; Dorsal radial rim ostectomy. |
| Progressive Radiolunate Arthrosis | 2% - 5% | Failure to correct DISI lunate deformity; unrecognized pre-existing cartilage wear. | Conversion to Total Wrist Arthrodesis. |
| CRPS Type I | 2% - 5% | Undefined; associated with severe perioperative pain and prolonged immobilization. | Aggressive hand therapy; Gabapentinoids; Stellate ganglion blocks; Vitamin C prophylaxis. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following limited wrist arthrodesis is a delicate balance between protecting the fragile healing osseous fusion mass and preventing irreversible capsular contracture and tendon adhesions. The protocol must be tailored to the specific procedure performed and the rigidity of the internal fixation utilized.
Phase I: Immobilization and Edema Control (Weeks 0-4)
Immediately postoperatively, the wrist is immobilized in a bulky, rigid plaster splint. At the first postoperative visit (typically 10-14 days), sutures are removed, and the patient is transitioned to a custom-molded thermoplastic short-arm cast or a rigid splint. During this phase, strict elevation and active range of motion of the digits, elbow, and shoulder are mandated to control edema and prevent proximal stiffness. If rigid plate fixation was utilized, the immobilization phase may be shorter (approximately 4 weeks) compared to K-wire fixation, which typically requires 6 to 8 weeks of rigid protection.
Phase II: Early Protected Motion (Weeks 4-8)
Once early radiographic signs of consolidation are evident and the initial immobilization period is complete, the patient is transitioned to a removable splint. A supervised hand therapy program is initiated, focusing on gentle, active range of motion of the wrist, emphasizing
