Principles and Techniques of Wrist Arthroscopy: Equipment, Positioning, and Indications
Key Takeaway
Wrist arthroscopy has evolved into an indispensable diagnostic and therapeutic modality in hand and upper extremity surgery. This comprehensive guide details the essential equipment, precise patient positioning, and broad surgical indications required for successful outcomes. From managing triangular fibrocartilage complex (TFCC) tears and carpal instability to assisting in the reduction of intraarticular distal radius fractures, mastering these foundational principles is critical for the modern orthopedic surgeon.
Comprehensive Introduction and Patho-Epidemiology
Historical Context and Evolution
Over the past three decades, wrist arthroscopy has transitioned from a purely diagnostic tool—initially met with skepticism due to the tight confines of the carpus—to a highly sophisticated therapeutic modality. Pioneered in the late 1970s and popularized in the 1980s by visionaries such as Chen, Whipple, and Poehling, the technique has fundamentally altered the algorithm for managing complex wrist pathology. It is now unequivocally considered the gold standard for evaluating intraarticular pathology of the radiocarpal, midcarpal, and distal radioulnar joints. The complex, multi-articulated nature of the wrist demands meticulous attention to detail regarding equipment selection, patient positioning, and portal placement. Mastery of these foundational elements is paramount for the orthopedic surgeon to safely navigate the tight confines of the carpus, minimize iatrogenic chondral injury, and optimize clinical outcomes.
Epidemiological Considerations in Wrist Pathology
The epidemiology of wrist pathology amenable to arthroscopic intervention spans a broad demographic, ranging from acute traumatic injuries in young athletes to degenerative and inflammatory conditions in the aging population. Acute traumatic events, frequently resulting from a fall on an outstretched hand (FOOSH), account for a massive proportion of intraarticular distal radius fractures, scapholunate (SL) ligament tears, and triangular fibrocartilage complex (TFCC) injuries. Studies indicate that up to 40% of displaced distal radius fractures present with concomitant, clinically significant TFCC tears, while SL interosseous ligament injuries are seen in nearly 30% of such fractures. Furthermore, chronic repetitive microtrauma in manual laborers and specific athletic cohorts (e.g., gymnasts, racquet sports players) frequently precipitates ulnar impaction syndrome and degenerative TFCC attrition.
The Paradigm Shift in Carpal Evaluation
Historically, the evaluation of chronic wrist pain relied heavily on clinical examination, standard radiography, and fluoroscopic arthrography, which often yielded high false-negative rates for intrinsic ligamentous and chondral lesions. The advent of high-resolution magnetic resonance imaging (MRI) and MR arthrography significantly improved diagnostic sensitivity; however, these modalities still fall short in assessing the dynamic stability of the carpus and the precise grading of partial ligament tears. Arthroscopy provides dynamic, magnified, and brilliantly illuminated visualization of the intrinsic carpal ligaments and articular surfaces, far surpassing the sensitivity of any non-invasive imaging modality. This paradigm shift has enabled surgeons to identify subtle pre-dynamic instabilities and early chondral wear patterns, allowing for proactive interventions that alter the natural history of conditions like Scapholunate Advanced Collapse (SLAC) and Scaphoid Nonunion Advanced Collapse (SNAC).
Detailed Surgical Anatomy and Biomechanics
Osseous Architecture and Articular Congruity
The wrist is not a single joint but a highly complex amalgamation of the radiocarpal, midcarpal, and distal radioulnar joints (DRUJ), comprising the distal radius, distal ulna, and eight carpal bones. The radiocarpal joint is formed by the articulation of the scaphoid and lunate with the elliptical, bi-concave distal radius (scaphoid and lunate fossae), while the triquetrum articulates with the TFCC. The midcarpal joint represents the articulation between the proximal carpal row (scaphoid, lunate, triquetrum) and the distal carpal row (trapezium, trapezoid, capitate, hamate). The osseous architecture is inherently unstable; the proximal row acts as an intercalated segment with no direct tendon attachments, relying entirely on osseous morphology, capsular constraints, and intrinsic/extrinsic ligaments for stability. Understanding the precise articular congruity and the three-dimensional topography of these fossae is critical for navigating the arthroscope without causing iatrogenic scuffing of the delicate hyaline cartilage.
Ligamentous Anatomy of the Radiocarpal and Midcarpal Joints
The ligamentous stabilizers of the wrist are broadly classified into intrinsic (interosseous) and extrinsic ligaments. The extrinsic volar ligaments are robust and provide the primary restraint to carpal translation. Key structures include the radioscaphocapitate (RSC) ligament, the long radiolunate (LRL) ligament, and the short radiolunate (SRL) ligament. The space of Poirier, a relative weak point between the RSC and LRL ligaments at the level of the capitolunate articulation, is the classic site for perilunate dislocations. Dorsally, the dorsal radiocarpal (DRC) and dorsal intercarpal (DIC) ligaments form a critical V-shaped stabilizing complex. The intrinsic ligaments, notably the scapholunate interosseous ligament (SLIL) and the lunotriquetral interosseous ligament (LTIL), are essential for synchronous carpal kinematics. The SLIL is composed of volar, membranous, and dorsal bands, with the dorsal band being the thickest and most biomechanically critical for preventing dorsal intercalated segment instability (DISI). Conversely, the volar band of the LTIL is the primary stabilizer against volar intercalated segment instability (VISI).
The Triangular Fibrocartilage Complex (TFCC)
The TFCC is the primary stabilizer of the DRUJ and the ulnar carpus, functioning as a sophisticated shock absorber that transmits approximately 20% of the axial load across the wrist. It is a complex, heterogeneous structure comprising the articular disc (central portion), the volar and dorsal radioulnar ligaments (ligamentum subcruentum), the meniscus homologue, the ulnocarpal ligaments (ulnolunate and ulnotriquetral), and the extensor carpi ulnaris (ECU) tendon subsheath. The central articular disc is avascular and relies on synovial diffusion for nutrition, rendering central tears (Palmer Type 1A) incapable of primary healing and thus ideal candidates for arthroscopic débridement. In contrast, the peripheral attachments (ulnar, volar, and dorsal) are highly vascularized, making peripheral tears (Palmer Types 1B, 1C, 1D) amenable to arthroscopic or arthroscopically assisted structural repair.
Neurovascular Topography and Portal Safety Zones
Safe arthroscopic portal placement dictates an intimate knowledge of the dorsal neurovascular topography. The superficial sensory branch of the radial nerve (SBRN) emerges from beneath the brachioradialis approximately 9 cm proximal to the radial styloid, arborizing extensively over the first, second, and third extensor compartments. The dorsal sensory branch of the ulnar nerve (DSBUN) branches from the main ulnar nerve approximately 5 cm proximal to the ulnar head, passing dorsally deep to the ECU tendon to supply the ulnar dorsum of the hand. The extensor tendons themselves serve as the primary landmarks for portal placement. The major arterial supply, including the radial artery passing through the anatomic snuffbox and the dorsal carpal arch, must be meticulously avoided. The concept of "safe zones" relies on placing portals perfectly between the extensor compartments using blunt dissection techniques to gently retract these critical neurovascular structures.
Exhaustive Indications and Contraindications
Diagnostic and Therapeutic Indications
The applications for wrist arthroscopy have expanded exponentially, driven by advancements in small-joint instrumentation and a deeper biomechanical understanding of carpal kinematics. Arthroscopy remains the definitive modality for the diagnosis and treatment of TFCC lesions, allowing for precise classification (Palmer system) and targeted intervention ranging from simple débridement of central avascular tears to complex all-inside capsular repairs for peripheral instability. In the realm of carpal instability, arthroscopy provides dynamic visualization to grade SL and LT tears via the Geissler classification. Management ranges from thermal shrinkage and débridement for partial tears (Geissler Grades I-II) to arthroscopically assisted percutaneous pinning or open repair for complete, unstable tears (Geissler Grades III-IV).
Furthermore, arthroscopically assisted reduction of intraarticular distal radius fractures is invaluable for evaluating and restoring articular congruity, clearing fracture hematoma, and managing associated soft-tissue injuries. Bone excision procedures, such as the arthroscopic wafer procedure for ulnar impaction syndrome, radial styloidectomy for early-stage SNAC, and proximal row carpectomy (PRC), have become increasingly commonplace. Inflammatory arthritides, septic arthritis, and post-traumatic stiffness also represent robust indications for arthroscopic synovectomy, lavage, and arthrolysis.
Absolute and Relative Contraindications
While wrist arthroscopy is minimally invasive, it is not without risk, and careful patient selection is mandatory. Absolute contraindications include active superficial soft tissue infections (e.g., cellulitis) over the portal sites, which risk seeding the sterile intraarticular space. Severe distortion of the bony anatomy due to massive trauma, advanced degenerative joint disease with complete obliteration of the joint space, or severe capsular contracture that precludes safe joint distraction and instrument insertion also represent absolute contraindications.
Relative contraindications include complex regional pain syndrome (CRPS), where any surgical intervention may exacerbate the sympathetically mediated pain cycle. Bleeding diatheses and severe medical comorbidities must be optimized pre-operatively. Additionally, performing a purely diagnostic arthroscopy without a clear therapeutic plan or in the setting of vague, non-localized wrist pain in a patient with significant psychiatric overlays is generally discouraged.
| Category | Indications for Wrist Arthroscopy | Contraindications for Wrist Arthroscopy |
|---|---|---|
| Trauma / Fractures | Intraarticular distal radius fractures (step-off >2mm); Scaphoid fractures (percutaneous fixation assistance); Acute TFCC tears (Palmer 1B). | Massive crush injuries with severe architectural distortion; Compartment syndrome of the forearm/hand. |
| Ligamentous / Instability | Scapholunate (SL) tears (Geissler I-IV); Lunotriquetral (LT) tears; Midcarpal instability. | Complete obliteration of the radiocarpal space preventing distraction. |
| Degenerative / Structural | Ulnar impaction syndrome (Wafer procedure); Early SNAC/SLAC (Styloidectomy); Dorsal ganglion excision. | End-stage pancarpal arthritis (where arthrodesis is definitively indicated). |
| Inflammatory / Infectious | Rheumatoid arthritis (Synovectomy); Septic arthritis (Lavage and débridement). | Active overlying cellulitis or superficial skin infection at portal sites (Absolute). |
| Miscellaneous | Undiagnosed chronic wrist pain (after exhaustive non-operative management and advanced imaging); Adhesion release. | Uncontrolled Complex Regional Pain Syndrome (CRPS); Severe, uncorrectable coagulopathy. |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and Pre-Operative Templating
Thorough pre-operative planning begins with a meticulous clinical examination correlated with high-quality orthogonal radiographs. Advanced imaging, particularly high-resolution 3-Tesla MRI or MR arthrography, is routinely employed to map the exact location and extent of TFCC pathology, intrinsic ligament tears, and occult chondral lesions. For intraarticular fractures, computed tomography (CT) with 3D reconstructions is critical for templating fracture fragment geometry and planning the trajectory of arthroscopically assisted percutaneous fixation. The surgeon must mentally map the portal placements relative to the specific pathology identified on imaging to ensure optimal trajectory and avoid "fighting the scope" during the procedure.
Essential Equipment and Instrumentation
The tight confines of the radiocarpal and midcarpal joints necessitate specialized, low-profile equipment. Utilizing standard knee or shoulder arthroscopy equipment in the wrist significantly increases the risk of iatrogenic scuffing of the articular cartilage. A short-barrel arthroscope with a diameter of 2.5 to 2.7 mm and a 30-degree lens-offset angle is considered the standard workhorse. Smaller scopes ranging from 1.7 to 2.0 mm are highly beneficial for navigating extremely tight joints, evaluating the DRUJ, or assessing pediatric patients.
Fluid management is critical. While gravity feed is usually satisfactory for routine diagnostic procedures, automated infusion pumps provide superior, consistent irrigation and allow for the aggressive use of motorized suction-cutting tools. However, strict pressure monitoring is imperative. The wrist capsule is small and relatively non-compliant. Excessive hydrostatic pressure can lead to rapid fluid extravasation into the forearm compartments, precipitating acute compartment syndrome. Pressures should generally not exceed 30 to 40 mm Hg. Manual instruments, including a 1.5 mm four-jaw shallow probe, 2.0 to 2.5 mm basket forceps, full-radius motorized shavers, and bipolar radiofrequency (RF) wands, must be readily available on the back table.
Anesthesia and Tourniquet Control
Wrist arthroscopy can be performed under regional block anesthesia (e.g., supraclavicular or axillary brachial plexus block) or general anesthesia. Regional anesthesia is frequently preferred as it provides excellent intraoperative muscle relaxation and prolonged postoperative analgesia. General anesthesia may be indicated if multiple complex procedures are anticipated, if bone grafting from a distant site (e.g., iliac crest) is required, or to ensure absolute patient immobility during delicate intraarticular work. The use of a well-padded pneumatic arm tourniquet is highly recommended to maintain a bloodless field, which is critical given the small volume of the joint space. The tourniquet is typically inflated to 250 mm Hg (or 100 mm Hg above the patient's systolic blood pressure) after thorough exsanguination of the limb using an Esmarch bandage.
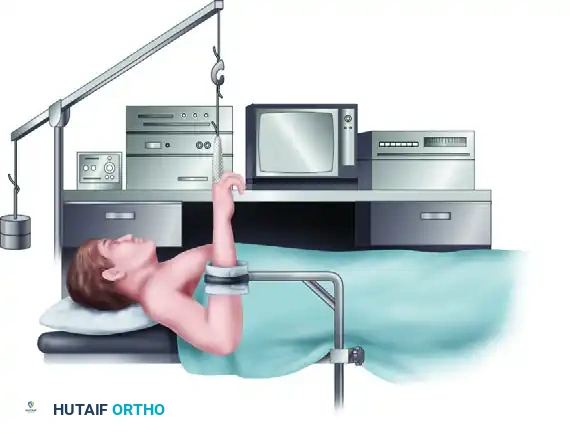
The Vertical Traction Setup
The most common configuration for wrist arthroscopy is the vertical traction setup, which utilizes the principle of ligamentotaxis to open the radiocarpal and midcarpal spaces. The patient is positioned supine with the operative shoulder abducted to 90 degrees and supported on a radiolucent hand table. The elbow is flexed to 90 degrees, directing the hand and fingers vertically toward the ceiling. Sterile fingertraps (wire mesh or nylon) are applied to the index and long fingers. Applying traps to the ring or small fingers is generally avoided to prevent ulnar nerve traction neurapraxia.
The fingertraps are connected to a specialized robotic traction tower, a ceiling hook, or an overhead pole and pulley system. Traction weights ranging from 4 to 7 lbs (approximately 2 to 3 kg) are applied. A padded forearm or wrist stabilizer (counterweight strap) is placed across the proximal forearm to provide counter-traction and stabilize the limb in space. This setup ensures consistent joint distraction, allowing for the safe introduction of the arthroscope and instruments without traumatizing the articular surfaces.
The Horizontal Setup
An alternative positioning technique is the horizontal setup, where the elbow is extended, and the hand is placed flat on the hand table. This position is particularly advantageous for the arthroscopically assisted reduction of intraarticular distal radius fractures and certain complex carpal reconstructive procedures. Biomechanically, it allows the surgeon to freely pronate and supinate the forearm, facilitating the reduction of specific fracture fragments. Furthermore, it allows for unimpeded, orthogonal fluoroscopic imaging (C-arm) without the radiopaque elements of the traction tower obstructing the radiographic view. Traction in this position is usually maintained manually by an assistant or via a specialized horizontal distraction frame that applies longitudinal traction while keeping the hand in a pronated, horizontal plane.
Step-by-Step Surgical Approach and Fixation Technique
Radiocarpal Portal Establishment
Precise portal placement is the cornerstone of safe and effective wrist arthroscopy. Portals are named based on their relationship to the dorsal extensor compartments. The procedure begins with the establishment of the 3-4 Portal, the primary viewing portal. It is located between the 3rd compartment (Extensor Pollicis Longus - EPL) and the 4th compartment (Extensor Digitorum Communis - EDC), palpable as a soft spot approximately 1 cm distal to Lister's tubercle.
Crucially, a scalpel must never be used to blindly incise the capsule. The skin is incised superficially (epidermis and dermis only) using a #15 blade. A blunt hemostat is then introduced to spread the subcutaneous tissues down to the capsule, gently pushing away the superficial sensory branches of the radial nerve. The capsule is then punctured with a blunt trocar to enter the joint. Once the arthroscope is introduced and intraarticular placement is confirmed via visualization of the scaphoid and radius, the 4-5 Portal (primary working portal) is established under direct intraarticular visualization. Located between the EDC and the 5th compartment (Extensor Digiti Minimi - EDM), this portal allows optimal access to the TFCC and ulnar carpus. The 6R Portal (radial to the ECU tendon) and 6U Portal (ulnar to the ECU tendon) are subsequently established as needed for peripheral TFCC repairs or as outflow tracts, with extreme care taken at the 6U portal to protect the dorsal sensory branch of the ulnar nerve.
Midcarpal Portal Establishment
Evaluation of the midcarpal joint is mandatory for assessing intrinsic ligament integrity (SL and LT ligaments) and dynamic carpal stability. The Radial Midcarpal (MCR) Portal is located approximately 1 cm distal to the 3-4 portal, situated in the palpable depression between the scaphoid, lunate, and capitate. Using the same "nick and spread" technique, the trocar is directed slightly proximally to match the slope of the capitate head. This portal provides an unparalleled view of the scapholunate interval from the distal perspective. The Ulnar Midcarpal (MCU) Portal is located approximately 1 cm distal to the 4-5 portal, in line with the axis of the fourth metacarpal. It is utilized to evaluate the lunotriquetral interval and the triquetrohamate articulation.
Distal Radioulnar Joint (DRUJ) Portals
When pathology of the DRUJ is suspected, such as proximal TFCC tears or isolated DRUJ arthritis, dedicated DRUJ portals are required. The Proximal DRUJ Portal is located just proximal to the dorsal radioulnar ligament, between the radius and the ulnar head. The Distal DRUJ Portal is located just distal to the ulnar head, allowing visualization of the undersurface of the TFCC. These portals are technically demanding due to the extremely tight confines of the DRUJ and the proximity of the ulnar neurovascular bundle, often requiring the use of a 1.9 mm or 2.0 mm arthroscope.
Diagnostic Sweep and Systematic Joint Evaluation
A systematic, reproducible diagnostic sweep is essential to ensure no pathology is missed. In the radiocarpal joint, the sweep begins radially, evaluating the volar radioscaphocapitate and long radiolunate ligaments. The arthroscope is then swept to assess the articular surfaces of the scaphoid fossa and the proximal scaphoid pole. Moving ulnarly, the scapholunate interosseous ligament is probed for tension and step-off. The lunate fossa and proximal lunate are inspected, followed by the lunotriquetral ligament. Finally, the arthroscope is directed toward the ulnar carpus to meticulously evaluate the TFCC, assessing the articular disc for central perforations and probing the peripheral attachments for loss of tension or "trampoline effect." A similar systematic sweep is performed in the midcarpal joint, confirming the integrity of the intrinsic ligaments and the articular surfaces of the distal carpal row.
Therapeutic Interventions and Fixation Techniques
Following the diagnostic sweep, therapeutic interventions are executed. For Palmer Type 1B TFCC tears, an outside-in or all-inside capsular repair is performed using specialized suture passing devices, securing the avulsed complex back to the ulnar capsule and ECU subsheath. In the setting of Geissler Grade II or III scapholunate tears, arthroscopic thermal shrinkage using a bipolar RF wand can be employed to tighten the attenuated volar and membranous portions of the ligament, often combined with percutaneous Kirschner wire (K-wire) fixation across the scaphoid and lunate to protect the repair during healing. For intraarticular distal radius fractures, the arthroscope is used to guide the manipulation of specific osteochondral fragments using a freer elevator or bone tamp introduced through a working portal, ensuring anatomic reduction (<1 mm step-off) prior to the application of a volar locking plate or percutaneous screws.
Complications, Incidence Rates, and Salvage Management
Neurologic and Vascular Injuries
Despite its minimally invasive nature, wrist arthroscopy carries a distinct complication profile, with overall complication rates reported between 2% and 5% in the literature. Neurologic injury is the most frequently encountered complication, predominantly involving the superficial sensory branch of the radial nerve (SBRN) during the establishment of the 1-2 or 3-4 portals, and the dorsal sensory branch of the ulnar nerve (DSBUN) during 6U portal placement. These injuries typically manifest as transient neurapraxias secondary to aggressive retraction or thermal injury from RF devices, though complete transections have been reported. Vascular injuries are exceedingly rare but can occur if the radial artery is violated during radial-sided portal placement.
Iatrogenic Chondral and Soft Tissue Damage
Iatrogenic scuffing or gouging of the delicate hyaline cartilage is a significant risk, particularly for inexperienced surgeons or when using inappropriately large instruments (e.g., 4.0 mm shavers) in a tight radiocarpal space. Meticulous portal placement, adequate joint distraction, and the use of 2.5 mm or smaller instruments are critical preventative measures. Tendon lacerations, most commonly involving the Extensor Pollicis Longus (EPL) or the Extensor Digitorum Communis (EDC), can occur if a scalpel is plunged too deeply during portal creation or if motorized shavers are used indiscriminately without direct visualization of the cutting window.
Infection, Stiffness, and Hardware Complications
Postoperative septic arthritis is rare (incidence <0.5%) but represents a catastrophic complication requiring immediate arthroscopic lavage, extensive débridement, and targeted intravenous antibiotic therapy. Postoperative stiffness and complex regional pain syndrome (CRPS) are more common, often resulting from excessive tourniquet times, inadequate postoperative pain control, or delayed initiation of rehabilitation. Hardware complications, such as prominent suture knots causing subcutaneous irritation following TFCC repairs or pin-tract infections from percutaneous K-wires, require vigilant postoperative monitoring and timely hardware removal when indicated.
| Complication | Estimated Incidence | Etiology / Risk Factors | Prevention and Salvage Management |
|---|---|---|---|
| SBRN / DSBUN Neurapraxia | 1.5% - 3.0% | Blind scalpel incision; Aggressive retractor use; Thermal injury from RF wands. | Prevention: Strict "nick and spread" technique; Avoid 6U portal if possible. Salvage: Observation, Gabapentin; Neurolysis or neuroma excision if persistent. |
| Iatrogenic Cartilage Scuffing | 2.0% - 4.0% | Inadequate joint distraction; Use of oversized instruments; Poor portal trajectory. | Prevention: Minimum 4-7 lbs vertical traction; Use 2.5mm scopes/shavers. Salvage: Chondroplasty of loose flaps; Microfracture for full-thickness gouges. |
| Tendon Laceration (EPL/EDC) | < 1.0% | Deep scalpel plunging; Blind use of motorized shavers. | Prevention: Direct visualization of shaver window at all times. Salvage: Immediate open primary tendon repair or tendon transfer. |
| Fluid Extravasation / Compartment Syndrome | < 0.5% | High-pressure infusion pumps (>40 mmHg); Prolonged surgical time; Capsular defects. | Prevention: Gravity flow preferred; Strict pump pressure monitoring. Salvage: Immediate cessation of fluid; Emergent forearm and hand fasciotomies. |
| Septic Arthritis | < 0.5% | Break in sterile technique; Pre-existing superficial skin infection. | Prevention: Meticulous prep and drape; Pre-operative prophylactic antibiotics. Salvage: Emergent arthroscopic I&D; IV antibiotics based on cultures. |
Phased Post-Operative Rehabilitation Protocols
Phase I: Immediate Post-Operative Period (Weeks 0-2)
Postoperative management is highly tailored to the specific pathology treated and the structural integrity of any repairs performed. For purely diagnostic arthroscopies, simple débridements, or arthroscopic ganglionectomies, the patient is placed in a bulky soft dressing or a removable volar splint. The primary goals during Phase I are edema control, pain management, and the prevention of tendon adhesions. Immediate, aggressive active range of motion (ROM) of the digits, elbow, and shoulder is instituted in the recovery room. Wrist ROM exercises, including gentle flexion, extension, pronation, and supination, are typically initiated within 3 to 5 days postoperatively as pain allows.
Conversely, for patients who have undergone structural repairs (e.g., TFCC peripheral repair, SL ligament thermal shrinkage and pinning), rigid immobilization is mandatory. These patients are placed in a well-molded Muenster-style cast or a sugar-tong splint that completely restricts forearm pronation and supination while allowing full elbow flexion and extension. Digital ROM is heavily emphasized to prevent intrinsic stiffness.
Phase II: Intermediate Rehabilitation (Weeks 2-6)
For simple débridement cases, Phase II focuses on achieving full active and passive wrist ROM and initiating light isometric strengthening. Modalities such as fluidotherapy and ultrasound may be utilized to manage residual stiffness.
For repair cases, the rigid immobilization is typically maintained until the 4-to-6-week mark. At this juncture, casts or percutaneous K-wires are removed, and the patient is transitioned to a custom-molded removable thermoplastic splint. Supervised therapy begins with gentle, active-assisted ROM. For SL ligament repairs, rehabilitation heavily emphasizes the "dart-thrower's motion" (extension/radial deviation to flexion/ulnar deviation), as biomechanical studies have demonstrated that this specific plane of motion minimizes strain on the healing scapholunate interosseous ligament while promoting functional recovery.
Phase III: Advanced Strengthening and Return to Play (Weeks 6-12+)
Phase III involves the progressive weaning of splint use and the initiation of dynamic strengthening and proprioceptive re-education. For TFCC repairs, strengthening of the ECU and pronator quadratus is emphasized to provide dynamic stability to the DRUJ. Work-hardening programs and sport-specific plyometric drills are integrated between weeks 8 and 12. Return to heavy manual labor or contact sports is generally permitted between 3 and 4 months postoperatively, contingent upon the restoration of at least 80% of contralateral grip strength and the absence of pain under mechanical load.
Summary of Landmark Literature and Clinical Guidelines
Foundational Studies in Wrist Arthroscopy
The evolution of wrist arthroscopy is deeply rooted in several landmark anatomical and clinical studies. Palmer's 1989 seminal paper on the anatomy and biomechanics of the TFCC established the universally accepted classification system for TFCC lesions, fundamentally differentiating between traumatic (Class 1) and degenerative (Class 2) tears, and dictating the modern algorithmic approach to treatment. Similarly, Geissler's 1996 publication on the arthroscopic classification of carpal instability provided surgeons with a reproducible, dynamic grading scale for scapholunate and lunotriquetral interosseous ligament tears, shifting the diagnostic gold standard away from static arthrography. Whipple's early textbook on wrist arthroscopy detailed the precise neurovascular topography of the dorsal wrist, establishing the safe zones for portal placement that remain the standard of care today.
Modern Evidenced-Based Practice Guidelines
Contemporary clinical guidelines, supported by the American Academy of Orthopaedic Surgeons (AAOS) and the American Society for Surgery of the Hand (ASSH), strongly endorse wrist arthroscopy for specific indications. Level I and II evidence supports the superiority of arthroscopically assisted reduction of intraarticular distal radius fractures over fluoroscopy alone in achieving anatomic articular congruity and identifying concomitant soft-tissue injuries. Furthermore,
