Scapholunate Instability: A Masterclass in Dorsal Ligament-Splitting Capsulotomy and Brunelli Tenodesis
Key Takeaway
This masterclass provides an exhaustive, real-time guide to Brunelli tenodesis for scapholunate instability. We meticulously detail preoperative planning, patient positioning, comprehensive surgical anatomy, and the step-by-step intraoperative execution of the dorsal ligament-splitting capsulotomy and FCR tendon reconstruction. Fellows will gain critical insights into neurovascular protection, precise instrument use, graft tensioning, and essential pearls for managing potential complications and ensuring optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
The Clinical Challenge of Scapholunate Dissociation
Welcome, colleagues and fellows, to an exhaustive exploration of one of the most formidable challenges in hand and wrist surgery: scapholunate dissociation (SLD). This pathology represents a profound symptomatic wrist dysfunction stemming from a partial or total rupture of the scapholunate interosseous ligament (SLIL) complex, inevitably accompanied by progressive carpal malalignment if left unaddressed. As orthopedic surgeons, our definitive goal is to restore the complex kinematics of the proximal carpal row. We achieve this through meticulous anatomical restoration and, when primary repair is no longer viable, through robust soft tissue reconstructions such as the modified Brunelli tenodesis. This procedure, utilizing a dorsal ligament-splitting capsulotomy, remains a cornerstone in our armamentarium for addressing dynamic and reducible static instability.
The clinical presentation of SLD can be highly variable, demanding a high index of suspicion from the treating surgeon. Patients often present with dorsal radial wrist pain, diminished grip strength, and a subjective sensation of "clunking" or giving way during loaded wrist extension. Scapholunate point tenderness—sharp pain elicited by palpating the interval just distal to Lister's tubercle—is a hallmark sign, indicating localized synovitis or structural failure. Furthermore, provocative maneuvers such as the scaphoid shift test (Watson's test) are critical. In a structurally deficient wrist, axial loading coupled with radial deviation forces the proximal pole of the scaphoid to subluxate dorsally out of the scaphoid fossa, producing a palpable and painful clunk upon release. Recognizing these subtle clinical nuances is the first step in preventing the devastating long-term sequelae of carpal instability.
Epidemiological Considerations and Injury Mechanisms
Scapholunate dissociation is the most common form of carpal instability, frequently resulting from high-energy traumatic events. Epidemiologically, it is predominantly seen in young, active individuals following violent trauma, such as a fall from a height onto an outstretched hand (FOOSH) or high-speed motor vehicle and motorcycle collisions. The classic mechanism involves extreme wrist hyperextension, ulnar deviation, and intercarpal supination, which sequentially loads and ruptures the palmar extrinsic ligaments, the SLIL complex, and finally the dorsal capsular structures. However, it is imperative to recognize that SLD can also present with an insidious onset. Patients may not recall a specific catastrophic traumatic event, but rather repetitive microtrauma or low-energy sprains that progressively attenuate the ligamentous restraints.
Beyond acute trauma, chronic inflammatory arthropathies play a significant role in the pathogenesis of spontaneous scapholunate failure. Conditions such as rheumatoid arthritis, calcium pyrophosphate deposition disease (CPPD/chondrocalcinosis), and advanced gout can cause enzymatic degradation and attritional rupture of the SLIL. In these scenarios, the ligamentous complex is destroyed not by a single supraphysiologic force, but by a relentless inflammatory cascade that compromises the viscoelastic properties of the collagen matrix. Understanding the exact etiology is crucial, as the biologic healing potential of a traumatically avulsed ligament vastly differs from one that has undergone chronic inflammatory degeneration, directly influencing our surgical decision-making and reconstructive strategy.
Natural History and the SLAC Wrist Progression
The natural history of an untreated complete scapholunate ligament rupture is a predictable and unforgiving progression toward degenerative arthritis, classically described as the Scapholunate Advanced Collapse (SLAC) wrist. Initially, partial injuries or "predynamic instability" may only be evident on arthroscopic evaluation, with normal resting radiographs. As the secondary stabilizers (such as the scaphotrapezial-trapezoid and scaphocapitate ligaments) undergo viscoelastic creep and attenuate over time, the wrist transitions into "dynamic instability," where a scapholunate gap (diastasis) is visible only under stress loading, such as a clenched-fist anteroposterior radiograph.

Once the secondary restraints completely fail, the scaphoid assumes a permanently flexed and pronated posture, while the lunate extends, leading to static instability and the classic Dorsal Intercalated Segment Instability (DISI) deformity. The abnormal joint contact mechanics between the flexed scaphoid and the elliptical scaphoid fossa of the distal radius lead to focal areas of high peak contact stress. This manifests as cartilage deterioration at the radial styloid and the scaphoid's proximal pole—the hallmark of SLAC Stage I. If left to its natural progression, the degenerative process marches proximally and ulnarly, encompassing the entire radioscaphoid joint (SLAC Stage II), and eventually involving the capitolunate articulation (SLAC Stage III) as the capitate migrates proximally into the widened scapholunate interval.
Detailed Surgical Anatomy and Biomechanics
The Scapholunate Interosseous Ligament Complex
Before we can execute a reconstructive masterclass, a profound, three-dimensional understanding of the periscaphoid anatomy is paramount. The scapholunate interosseous ligament (SLIL) complex is a C-shaped structure that serves as the primary stabilizer between the scaphoid and lunate. It is anatomically and biomechanically divided into three distinct regions: the dorsal scapholunate ligament, the palmar scapholunate ligament, and the proximal fibrocartilaginous membrane.
The dorsal scapholunate ligament is the thickest, most critical component of this complex. Composed of dense, transversely oriented collagen fibers, it acts as the primary restraint against translation and diastasis. Biomechanical studies have demonstrated that it boasts an average yield strength of 260 Newtons (N), making it the ultimate target for our soft tissue reconstructions. The palmar scapholunate ligament, in contrast, consists of longer, more obliquely oriented fibers. While it provides essential restraint against rotational instability, permitting the scaphoid to rotate smoothly relative to the lunate during wrist motion, it is significantly weaker, with a yield strength of approximately 118 N.
The proximal fibrocartilaginous membrane connects the adjacent convex articular borders of the scaphoid and lunate, essentially forming a watertight seal that separates the radiocarpal joint from the midcarpal joint. Structurally, it is the weakest link, failing at roughly 63 N. It is critical for fellows to recognize that while age-related central perforations of this proximal membrane are common and often visualized on arthrograms or MRI, an isolated tear of the membranous portion does not, in itself, confer mechanical instability. True carpal collapse requires the catastrophic failure of the robust dorsal and palmar ligamentous components.
Secondary Carpal Stabilizers and the Radiocarpal Articulation
The stability of the proximal carpal row is not solely reliant on the SLIL complex; it is heavily dependent on a sophisticated network of secondary extrinsic ligaments. On the dorsal aspect, the dorsal intercarpal (DIC) ligament and the dorsal radiocarpal (DRC) ligament form a crucial "V" shaped stabilizing complex. The DIC, originating from the triquetrum and inserting on the scaphoid and trapezium, acts as a secondary checkrein against scaphoid flexion. When we perform our dorsal capsulotomy, preserving the integrity of the DIC is essential to prevent iatrogenic destabilization.
Palmar secondary stabilizers include the radioscaphocapitate (RSC) ligament, the long radiolunate (LRL) ligament, and the scaphocapitate (SC) and scaphotriquetral (STq) ligaments. The RSC ligament acts as a fulcrum around which the scaphoid rotates; if the SLIL is compromised, the scaphoid flexes over the intact RSC ligament. The geometry of the osseous articulation also dictates inherent stability. The scaphoid fossa of the distal radius is elliptical, whereas the lunate fossa is more spherical. A deeper scaphoid fossa provides greater osseous constraint, mitigating the sheer forces that attempt to drive the scaphoid into subluxation under axial load.
Biomechanical Cascade of Scapholunate Failure
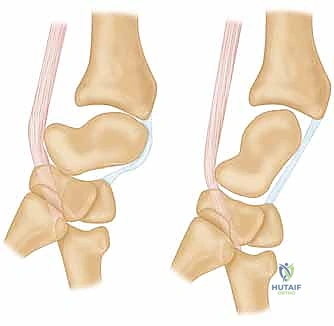
To comprehend the rationale behind the modified Brunelli tenodesis, one must understand the complex kinematics of the wrist under axial load. The proximal carpal row acts as an intercalated segment, devoid of direct tendinous insertions, relying entirely on ligamentous linkages and articular geometry to dictate its motion. When the wrist is subjected to an axial compressive force, the scaphoid, due to its oblique orientation, naturally tends to rotate into flexion and pronation. Conversely, the triquetrum, driven by the helicoidal shape of the hamate, is forced into extension.
In a healthy wrist, these opposing moments—scaphoid flexion and triquetral extension—are transmitted through the intact SLIL and lunotriquetral (LTq) ligaments to the lunate. The lunate acts as the central keystone, balancing these forces to maintain a stable, coapted proximal row that efficiently transfers load to the radius.

However, when the SLIL complex is completely disrupted, this delicate equilibrium is shattered. The scaphoid, uncoupled from the lunate, succumbs to the flexion forces, resulting in rotatory subluxation. The lunate, now tethered only to the extending triquetrum, is dragged into pathological extension, creating the classic DISI deformity.


As the diastasis widens, the capitate is driven proximally into the interval, acting like a wedge that further drives the scaphoid into flexion and dorsal subluxation over the dorsal rim of the radius. This biomechanical collapse is the fundamental pathology we aim to reverse with our tenodesis.
Exhaustive Indications and Contraindications
Staging Scapholunate Instability
Accurate staging of SLD is the absolute prerequisite for selecting the appropriate surgical intervention. We rely heavily on the classification system modified by Garcia-Elias et al., which categorizes the injury based on ligament integrity, reparability, and carpal alignment:
* Stage 1: Partial SLIL rupture (usually palmar or membranous). The dorsal SL ligament is intact. The scaphoid is stable. Best managed with arthroscopic debridement or thermal shrinkage.
* Stage 2: Complete SLIL rupture, but the dorsal ligament is primarily reparable. Carpal alignment is normal. Managed with direct anatomic repair and dorsal capsulodesis.
* Stage 3: Complete SLIL rupture, dorsal ligament is non-reparable (attritional or retracted), but the scaphoid remains normally aligned (dynamic instability).
* Stage 4: Complete SLIL rupture, non-reparable, with reducible rotatory subluxation of the scaphoid and reducible DISI.
* Stage 5: Complete SLIL rupture with irreducible malalignment. The secondary ligaments have contracted.
* Stage 6: SLAC wrist with established degenerative chondral changes.
Patient Selection Criteria for Reconstruction
The modified Brunelli tenodesis (often referred to as the three-ligament tenodesis) is the gold standard for Stage 3 and Stage 4 SLD. The ideal candidate is a symptomatic patient with a chronic, non-reparable scapholunate tear who demonstrates reducible carpal malalignment without evidence of advanced radiocarpal or midcarpal osteoarthritis.
The procedure aims to reconstruct the palmar scaphoid-trapezium-trapezoid (STT) ligament, the dorsal SL ligament, and the dorsal radiocarpal ligament using a strip of the flexor carpi radialis (FCR) tendon. It is crucial that the patient has adequate bone stock in the scaphoid to accommodate a 3.0mm to 3.5mm drill hole without catastrophic fracture. Furthermore, the patient must be compliant, as the postoperative rehabilitation protocol is lengthy and demands strict adherence to immobilization and progressive loading phases to protect the maturing tenodesis.
Absolute and Relative Contraindications
Recognizing when not to perform a soft tissue reconstruction is just as vital as mastering the technique itself. Attempting a Brunelli tenodesis in a poorly selected patient will inevitably lead to construct failure, persistent pain, and accelerated arthrosis.
| Contraindication Type | Specific Condition | Rationale / Consequence |
|---|---|---|
| Absolute | Established SLAC Wrist (Stage II/III) | Realigning an arthritic joint increases contact pressures on denuded cartilage, severely exacerbating pain. Requires salvage (e.g., PRC or 4-corner fusion). |
| Absolute | Irreducible Carpal Malalignment (Stage 5) | If the scaphoid or lunate cannot be manually or fluoroscopically reduced due to severe soft tissue contracture, the tenodesis will fail under excessive tension. |
| Absolute | Scaphoid Proximal Pole Avascular Necrosis | Drilling a tunnel through an avascular or fragmented proximal pole will result in scaphoid fracture and failure of graft incorporation. |
| Relative | Advanced Age / Low Functional Demand | The extensive surgery and prolonged rehab may outweight the benefits. Palliative denervation or limited fusion may be more appropriate. |
| Relative | Heavy Manual Laborers | High-demand workers may stretch out the soft tissue reconstruction over time. A partial wrist fusion (e.g., STT or SC fusion) might offer more durable stability, albeit at the cost of motion. |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging Modalities and Templating
Surgical success begins long before the first incision, relying on meticulous preoperative imaging. Standard posteroanterior (PA), lateral, and clenched-fist PA radiographs are mandatory to assess the scapholunate gap (Terry Thomas sign), the cortical ring sign of the flexed scaphoid, and the radiolunate angle indicating DISI.
However, advanced imaging is critical for confirming the diagnosis and ruling out contraindications. High-resolution Magnetic Resonance Imaging (MRI), particularly with intra-articular contrast (MR arthrography), provides unparalleled visualization of the SLIL complex remnants and the integrity of the articular cartilage.



MRI allows us to assess the viability of the scaphoid proximal pole and identify subtle chondral defects over the dorsal rim of the radius that might preclude a soft-tissue reconstruction. Preoperative templating involves measuring the scaphoid dimensions to select the appropriate drill bit (usually 3.0mm or 3.2mm) and interference screw or suture anchor sizes. Ensuring the scaphoid waist is wide enough to safely accommodate the tunnel without compromising structural integrity is a critical templating step.
Operating Room Setup and Patient Positioning
The patient is positioned supine on the operating table with the operative extremity extended on a radiolucent hand table. A well-padded proximal arm tourniquet is applied. I prefer to use a specialized wrist traction tower or lead hand to maintain position, though an assistant's hands are often required for dynamic reduction maneuvers during the procedure.
The fluoroscopy unit (C-arm) must be brought in from the foot or the opposite side of the table, positioned perpendicular to the limb to allow seamless transition between PA and lateral views without compromising the sterile field. The monitor should be directly in the surgeon's line of sight.
Anesthetic Considerations and Tourniquet Management
Regional anesthesia, specifically an axillary or supraclavicular brachial plexus block, is the modality of choice. It provides excellent intraoperative muscle relaxation, which is vital for reducing the chronically subluxated carpus, and offers superior postoperative pain control. General anesthesia is reserved for patients with contraindications to regional blocks. The limb is exsanguinated with an Esmarch bandage, and the tourniquet is inflated to 250 mmHg (or 100 mmHg above systolic pressure). Given that this complex reconstruction can easily exceed two hours, meticulous tourniquet time management is required, with a planned let-down if the ischemic time approaches 120 minutes.
Step-by-Step Surgical Approach and Fixation Technique
The Dorsal Ligament-Splitting Capsulotomy
The surgical approach is paramount to preserving the delicate vascularity and secondary stabilizers of the carpus. We utilize a longitudinal dorsal incision, centered over Lister's tubercle, extending roughly 4 cm proximally and 4 cm distally.
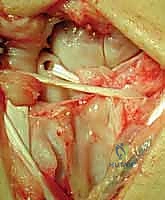
The extensor retinaculum is exposed, and the third extensor compartment is opened to transpose the extensor pollicis longus (EPL) tendon radially. The floor of the third compartment is incised, allowing elevation of the second compartment (ECRL and ECRB) radially and the fourth compartment (EDC) ulnarly. At this juncture, the terminal branch of the posterior interosseous nerve (PIN), located on the floor of the fourth compartment, is identified and prophylactically resected to provide partial wrist denervation and reduce postoperative pain.
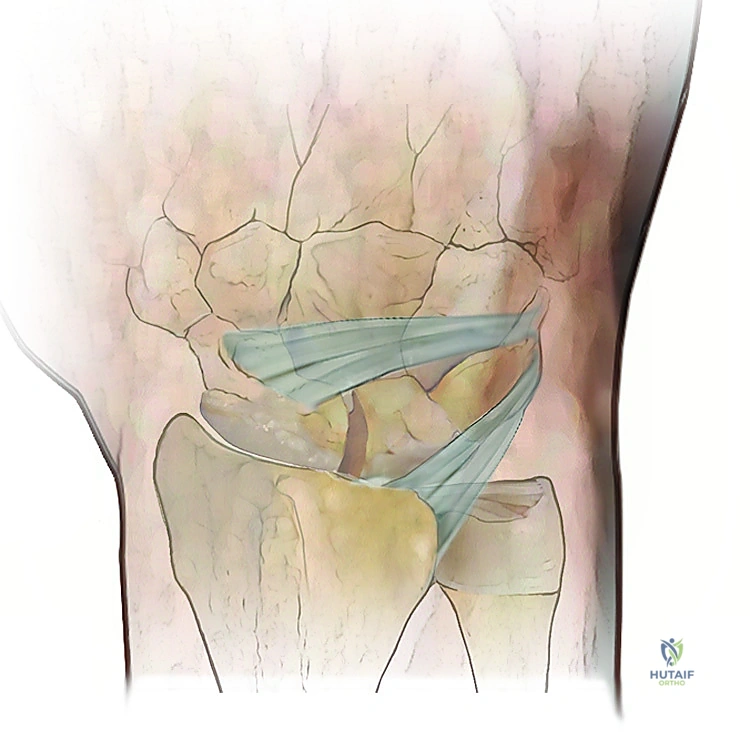
We then proceed with a dorsal ligament-splitting capsulotomy, as popularized by Berger. This technique respects the orientation of the dorsal intercarpal (DIC) and dorsal radiocarpal (DRC) ligaments. An inverted T-shaped or V-shaped incision is made, elevating capsular flaps that can be meticulously repaired later to restore dorsal stability.

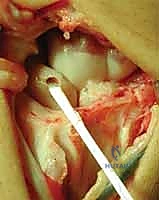
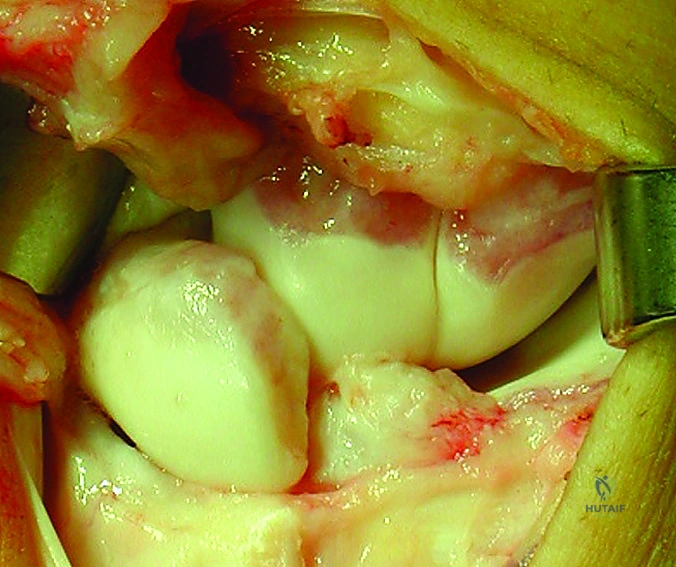
Joint Inspection and Preparation of the Scapholunate Interval
Upon entering the radiocarpal and midcarpal joints, the catastrophic nature of the SLD is immediately apparent. The joint is thoroughly irrigated, and the hypertrophic synovium is meticulously debrided. The articular surfaces of the scaphoid fossa, lunate fossa, and proximal scaphoid are inspected. If full-thickness chondral loss is identified, the tenodesis is aborted in favor of a salvage procedure.
The remnants of the torn SLIL are debrided to bleeding bone using a curette or motorized shaver. Using a combination of manual traction, ulnar deviation, and extension, the scaphoid and lunate are anatomically reduced. This reduction is temporarily secured using multiple 0.045-inch or 0.062-inch Kirschner wires (K-wires) driven from the scaphoid into the lunate, and from the scaphoid into the capitate. Fluoroscopy is used to confirm the restoration of the scapholunate gap (<2mm) and the correction of the DISI deformity (radiolunate angle <15 degrees).
The Modified Brunelli Tenodesis Procedure
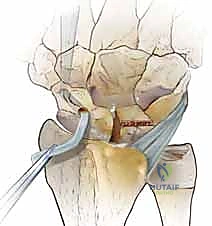
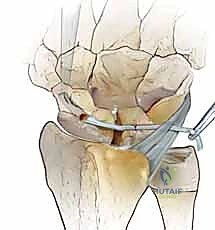
With the carpus reduced and pinned, we prepare the osseous tunnel. A guide pin is driven from the dorsal non-articular proximal pole of the scaphoid, aiming volarly and distally to exit at the palmar tuberosity of the scaphoid. This trajectory is critical; it must remain entirely intraosseous without breaching the radiocarpal or STT articular surfaces. A 3.0mm or 3.2mm cannulated drill is then used to over-drill the guide pin, creating the trans-scaphoid tunnel.
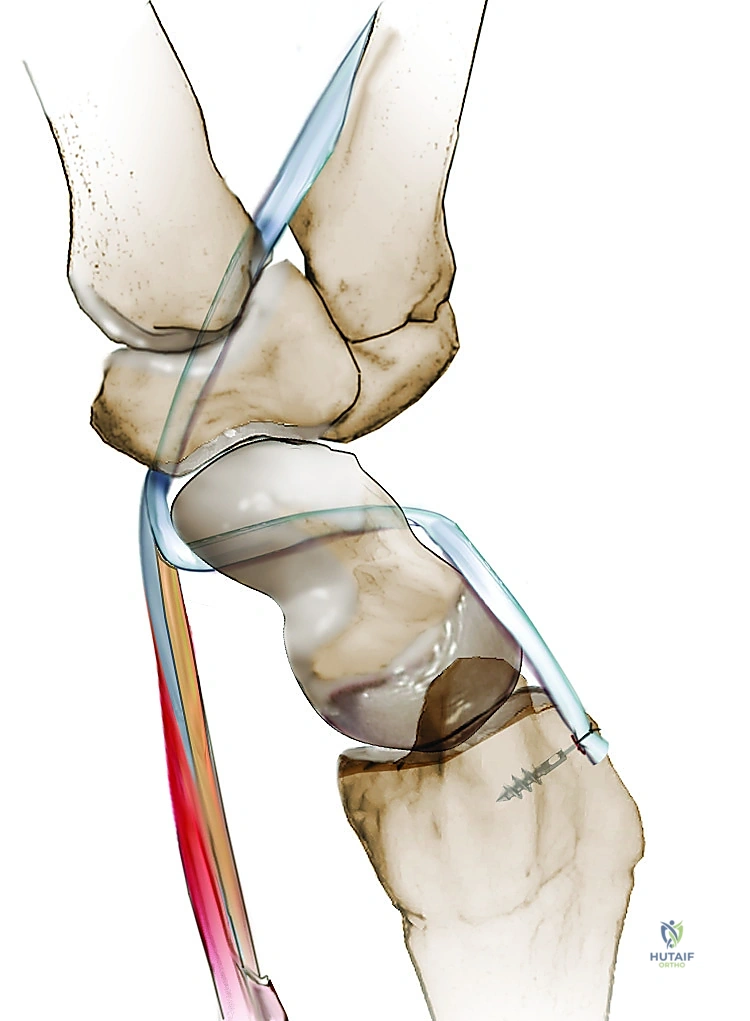
Attention is then turned to the volar aspect of the wrist. A 3 cm longitudinal incision is made over the distal flexor carpi radialis (FCR) tendon. The FCR sheath is opened, and a distally based strip comprising roughly one-third to one-half of the tendon's width is harvested, leaving its insertion on the base of the second metacarpal intact.
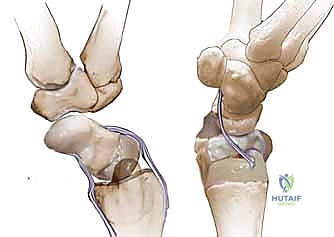
A curved tendon passer or a wire loop is passed from dorsal to volar through the scaphoid tunnel. The harvested FCR strip is retrieved and pulled dorsally through the scaphoid. This volar-to-dorsal passage reconstructs the palmar STT ligament complex, providing a crucial volar tether that resists scaphoid flexion.
Fixation, Tensioning, and Closure
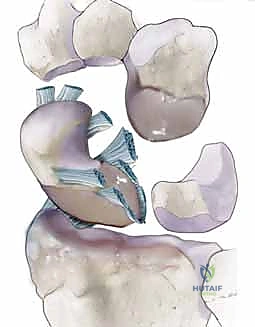
Once the tendon exits the dorsal proximal pole of the scaphoid, it is routed ulnarly across the scapholunate interval to the dorsal aspect of the lunate, effectively recreating the critical dorsal SL ligament.
A trough is prepared on the dorsal lunate, and a suture anchor (typically 2.5mm or 3.0mm) is inserted. The FCR tendon graft is pulled taut to maintain the reduction of the scapholunate interval.
The graft is then secured to the lunate anchor using high-strength non-absorbable sutures. To further augment the construct and recreate the dorsal radiocarpal ligament, the remaining tail of the FCR graft is routed proximally and ulnarly, and sutured to the dorsal rim of the radius or the DIC ligament.
The dorsal capsular flaps are meticulously imbricated and repaired over the tenodesis construct to provide a final layer of dorsal restraint.

The EPL tendon is left transposed in the subcutaneous tissues to prevent attrition over the hardware or capsular repair. The extensor retinaculum is repaired, and the skin is closed in a standard fashion. A bulky, sterile compression dressing and a volar-dorsal plaster splint are applied with the wrist in slight extension.
Complications, Incidence Rates, and Salvage Management
Intraoperative and Early Postoperative Complications
Despite meticulous technique, the modified Brunelli tenodesis is fraught with potential complications. Intraoperatively, the
Clinical & Radiographic Imaging Archive