Dorsal Wrist Approach: Expert Access to the Column of the Distal Radius
Key Takeaway
Learn more about Dorsal Wrist Approach: Expert Access to the Column of the Distal Radius and how to manage it. The dorsal approach to the wrist provides excellent exposure for extensor tendon repair, wrist fusion, and excision of the distal radius. It also facilitates open reduction and internal fixation of certain fractures and dislocations, offering access to the intermediate and radial columns of the distal radius. Volar approaches are often preferred for plate fixation of the distal radius.
Comprehensive Introduction and Patho-Epidemiology
The dorsal approach to the wrist represents a foundational surgical exposure in orthopedic surgery and hand surgery, providing unparalleled access to the dorsal aspect of the distal radius, the radiocarpal joint, the intercarpal joints, and the proximal metacarpal bases. Historically, the dorsal approach was the primary surgical corridor for the open reduction and internal fixation of distal radius fractures. During the late 20th century, dorsal plating was the standard of care for restoring articular congruity in comminuted distal radius fractures. However, early generation dorsal plates, such as the Pi plate, were historically associated with significant hardware prominence, extensor tendon tenosynovitis, and high rates of extensor pollicis longus rupture. These historical shortcomings temporarily shifted the global paradigm toward volar locking plates, even for fractures with predominant dorsal comminution, relying on fixed-angle constructs to cantilever the dorsal fragments.



While the advent of fixed-angle volar locking plates has undoubtedly revolutionized the management of distal radius fractures, the dorsal approach remains an indispensable technique in the orthopedic surgeon's armamentarium. Modern low-profile, fragment-specific dorsal implants have mitigated many of the historical complications, leading to a resurgence in the utilization of this approach for specific fracture patterns. The dorsal approach provides excellent exposure of all the extensor tendons that pass over the dorsal surface of the wrist. It allows direct visualization for synovectomy and repair of the extensor tendons in cases of rheumatoid arthritis, execution of total wrist arthrodesis, and excision of benign or malignant neoplastic lesions of the distal radius and carpus. The ability to directly visualize the articular surface of the radiocarpal and midcarpal joints is a distinct advantage over volar exposures, which often rely on indirect fluoroscopic assessment or arthroscopic assistance to confirm articular reduction.

Furthermore, the dorsal approach is the surgical corridor of choice for proximal row carpectomy, four-corner arthrodesis, dorsal stabilization of the wrist, and the management of complex carpal dislocations such as transscaphoid perilunate fracture-dislocations. Epidemiologically, the demand for dorsal wrist exposures is driven by high-energy trauma resulting in highly comminuted, intra-articular distal radius fractures with dorsal shear components, as well as degenerative conditions like advanced rheumatoid arthritis and scapholunate advanced collapse. The incidence of complex distal radius fractures requiring dorsal or combined approaches remains significant, particularly in the bimodal distribution of young males experiencing high-energy trauma and elderly females with osteoporotic bone sustaining low-energy falls.




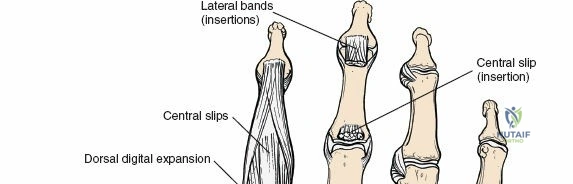
Mastery of this approach requires a profound understanding of the extensor retinaculum, the dorsal capsular ligaments, and the column theory of the distal radius. The increasing prevalence of high-velocity sporting injuries and motor vehicle collisions continues to sustain the necessity for profound anatomical and surgical competence regarding the dorsal wrist. Additionally, the rising aging population has led to a proportional increase in osteoporotic fractures that exhibit severe dorsal comminution, necessitating direct dorsal buttressing when volar constructs fail to provide adequate stability to the dorsal ulnar corner or the intermediate column.
Detailed Surgical Anatomy and Biomechanics
A comprehensive understanding of the dorsal wrist anatomy is critical for safe dissection and effective reconstruction. The dorsal aspect of the wrist is characterized by a thin soft tissue envelope, making it susceptible to hardware prominence and tendon irritation, but also allowing for relatively straightforward surgical exposure. The lack of a robust muscular cushion over the dorsal radius necessitates meticulous handling of the extensor retinaculum and the extensor tendons during any surgical intervention. The integumentary layer is highly mobile, relying on a delicate subdermal plexus for its vascular supply, which mandates full-thickness fasciocutaneous flaps during surgical dissection to prevent marginal skin necrosis.

Osteology and the Column Theory
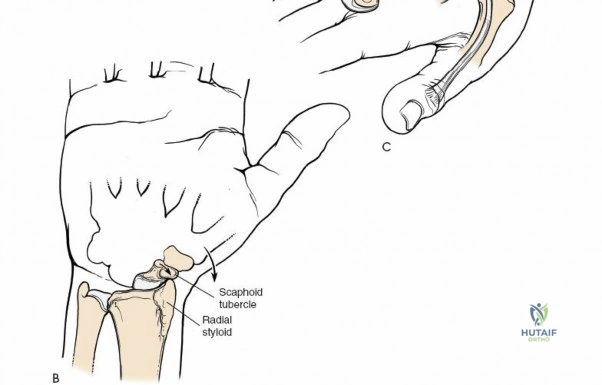
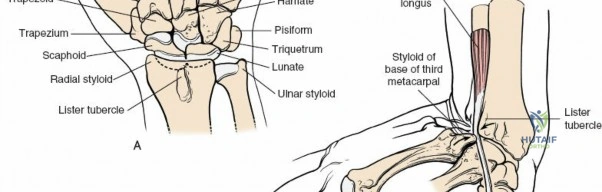
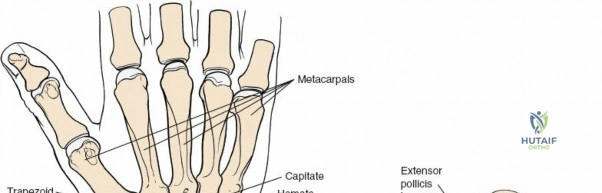
The distal radius is conceptualized biomechanically as a three-column structure, a model popularized by Rikli and Regazzoni. This biomechanical framework is essential for understanding load transmission and fracture fixation strategies. The radial column consists of the radial styloid and the scaphoid fossa. It acts as an osseous buttress against radial translation of the carpus and serves as the attachment site for the radioscaphocapitate and long radiolunate ligaments. The intermediate column comprises the lunate fossa and the sigmoid notch. This column is critical for load transmission from the carpus to the forearm and is frequently involved in intra-articular fractures, particularly dorsal die-punch fragments. The ulnar column consists of the distal ulna and the triangular fibrocartilage complex, serving as the axis of forearm rotation and providing stability to the distal radioulnar joint.


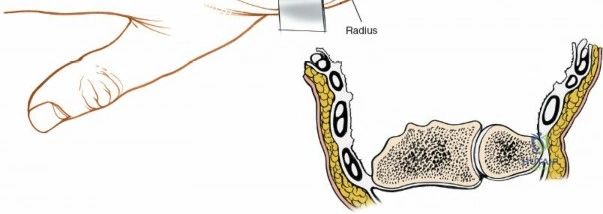
The dorsal approach provides direct, orthogonal access to the intermediate and radial columns, allowing for anatomic reduction of dorsal articular step-offs and restoration of the volar tilt. Lister's tubercle, a bony prominence on the dorsal radius, serves as a critical surgical landmark. It acts as a mechanical fulcrum for the extensor pollicis longus tendon, redirecting its line of pull toward the thumb. Biomechanically, the radiocarpal joint transmits approximately 80 percent of the axial load across the wrist, with the remaining 20 percent passing through the ulnocarpal articulation. Restoration of the articular congruity of the intermediate column is therefore paramount to preventing post-traumatic radiocarpal arthrosis, as even a 2-millimeter step-off can drastically alter contact pressures and accelerate degenerative changes.
Extensor Compartments and Retinaculum
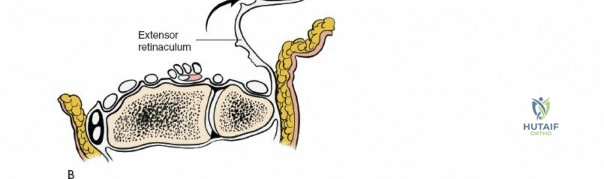
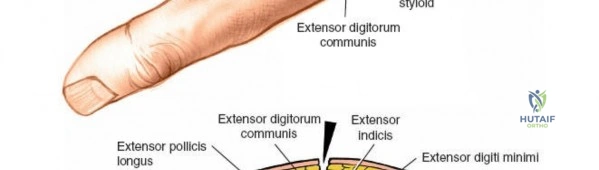
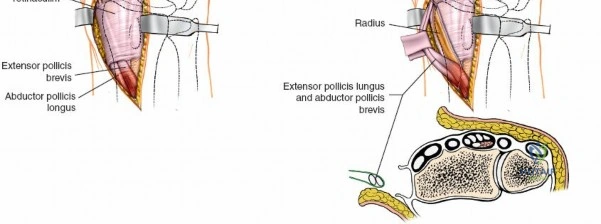
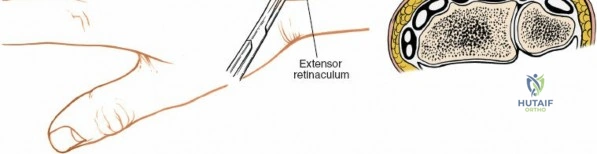
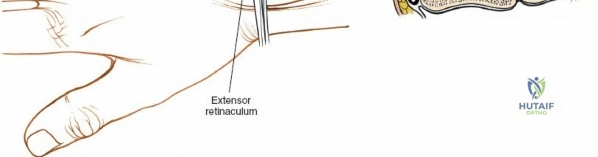
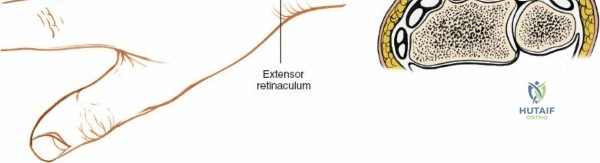
The extensor retinaculum is a dense fibrous band that prevents bowstringing of the extensor tendons during wrist extension. It is divided into six distinct fibro-osseous compartments by vertical septa that attach to the dorsal radius and ulna. The first compartment contains the abductor pollicis longus and extensor pollicis brevis. The second compartment houses the extensor carpi radialis longus and brevis, which are the primary wrist extensors. The third compartment, located immediately ulnar to Lister's tubercle, uniquely contains only the extensor pollicis longus.



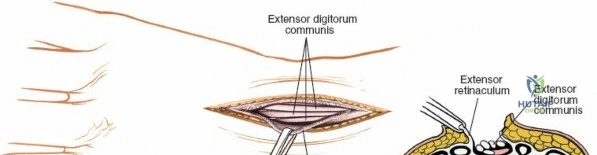
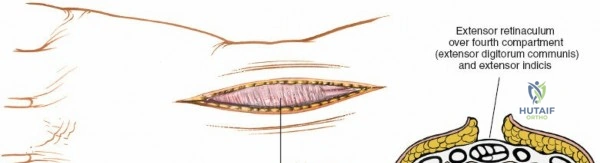
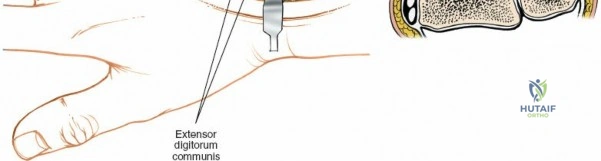
The fourth compartment is the largest, containing the extensor digitorum communis and the extensor indicis proprius. The fifth compartment contains the extensor digiti minimi, and the sixth compartment houses the extensor carpi ulnaris, which plays a pivotal role in the dynamic stability of the distal radioulnar joint. Surgical exposure typically involves releasing the third compartment to transpose the extensor pollicis longus, followed by subperiosteal elevation of the second and fourth compartments. This technique preserves the vertical septa and maintains the gliding tissue over the tendons, thereby minimizing the risk of postoperative adhesions and tendon attrition against newly placed osteosynthesis materials.
Neurovascular Structures and Capsular Ligaments
The sensory innervation of the dorsal wrist is provided by the superficial branch of the radial nerve radially and the dorsal sensory branch of the ulnar nerve ulnarly. These nerves run in the subcutaneous tissues and are highly susceptible to iatrogenic neuropraxia during initial incision and retraction. Deep to the extensor tendons lies the posterior interosseous nerve, which travels along the floor of the fourth extensor compartment. The posterior interosseous nerve provides terminal proprioceptive and nociceptive fibers to the dorsal wrist capsule and is frequently targeted for therapeutic denervation in chronic wrist pain syndromes, such as SLAC wrist or chronic scapholunate dissociation.

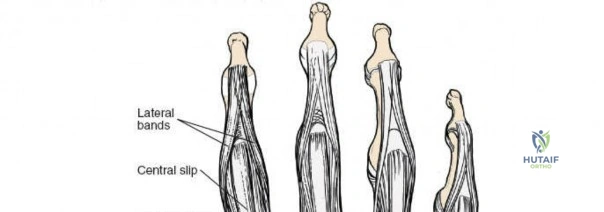
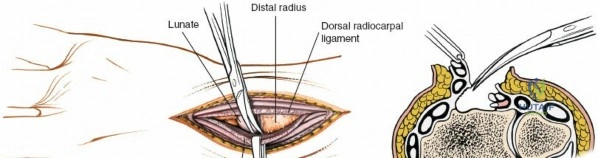
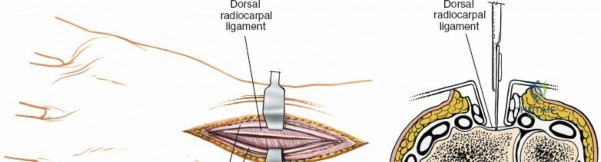
The dorsal capsular ligaments are critical for carpal stability and kinematic synchrony. Primarily, the dorsal radiocarpal ligament and the dorsal intercarpal ligament form a V-shaped configuration (often referred to as the dorsal V-ligament) that stabilizes the proximal carpal row and prevents volar intercalated segment instability. The dorsal radiocarpal ligament originates from the dorsal rim of the radius and inserts onto the lunate and triquetrum. The dorsal intercarpal ligament originates from the triquetrum and inserts onto the scaphoid and trapezium. Surgical capsulotomies must be meticulously designed—such as the Berger ligament-sparing capsulotomy—to split these ligaments along their fiber orientation or elevate them as a continuous flap, ensuring robust repair and preventing iatrogenic carpal instability.
Exhaustive Indications and Contraindications
The indications for the dorsal approach to the wrist are extensive, encompassing a wide array of traumatic, degenerative, and neoplastic conditions. Traumatic indications primarily involve distal radius fractures with significant dorsal comminution, dorsal shear fractures (AO Type B2), and dorsal die-punch fragments that cannot be adequately reduced or stabilized via a volar approach. While volar locking plates can cantilever dorsal fragments, highly comminuted dorsal cortices often lack the structural integrity to prevent secondary subsidence, mandating direct dorsal buttressing. Furthermore, the dorsal approach is the gold standard for the open reduction and internal fixation of acute scaphoid fractures via a dorsal percutaneous or mini-open technique, particularly for proximal pole fractures where the blood supply is tenuous and retrograde screw insertion is biomechanically advantageous.


In the realm of carpal instability, the dorsal approach is strictly mandated for the repair or reconstruction of the scapholunate interosseous ligament and the management of perilunate dislocations. The dorsal aspect of the scapholunate ligament is the thickest and most biomechanically significant portion, requiring direct dorsal visualization for anatomic repair or capsulodesis. Degenerative conditions, such as scapholunate advanced collapse (SLAC) and scaphoid nonunion advanced collapse (SNAC), necessitate dorsal exposure for salvage procedures including proximal row carpectomy and four-corner arthrodesis. Rheumatoid arthritis frequently requires a dorsal approach for extensive extensor tenosynovectomy, distal ulna resection (Darrach procedure or Sauvé-Kapandji procedure), and total wrist arthrodesis to correct severe volar subluxation and ulnar translation of the carpus.


Contraindications to the dorsal approach are relatively few but clinically significant. A volar shear fracture of the distal radius (Barton's fracture) is a direct contraindication for an isolated dorsal approach, as the volar fragments cannot be buttressed from the dorsum and require a volar buttress plate. Severe soft tissue compromise over the dorsal wrist, such as extensive burns, active local infection, or degloving injuries, precludes the use of this approach due to the high risk of wound breakdown, hardware exposure, and secondary tendon desiccation. Additionally, extreme caution must be exercised in patients with severe peripheral vascular disease or those on high-dose chronic corticosteroids, as the dorsal skin flap viability may be severely compromised.
Operative vs Non Operative Management
| Clinical Pathology | Operative Indication (Dorsal Approach) | Non Operative Management Strategy |
|---|---|---|
| Distal Radius Fracture | Dorsal comminution, dorsal die-punch, articular step-off > 2mm, loss of volar tilt > 10 degrees | Cast immobilization for non-displaced or stable extra-articular fractures |
| Scaphoid Fracture | Proximal pole fractures, displacement > 1mm, nonunion, intrasubstance comminution | Long-arm thumb spica casting for stable, non-displaced distal pole fractures |
| Scapholunate Instability | Acute complete tears, repairable SL ligament, DISI deformity, perilunate trauma | Proprioceptive therapy, dart-thrower's motion rehab for partial, dynamic tears |
| Rheumatoid Arthritis | Impending extensor tendon rupture, severe tenosynovitis, profound carpal subluxation | Disease-modifying antirheumatic drugs (DMARDs), local corticosteroid injections |
| SLAC/SNAC Wrist | Stage II or III requiring PRC or 4-corner arthrodesis, intractable pain | Activity modification, NSAIDs, custom rigid orthosis, intra-articular injections |
| Perilunate Dislocation | Acute presentation requiring open reduction, ligament repair, and K-wire stabilization | Rarely indicated; closed reduction is only a temporary measure prior to surgery |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is mandatory to ensure a successful outcome when utilizing the dorsal approach. High-quality orthogonal radiographs of the wrist (posteroanterior, lateral, and oblique views) are the initial step in evaluating the osseous architecture. For complex intra-articular fractures of the distal radius or carpus, a non-contrast computed tomography (CT) scan is highly recommended and considered the standard of care in modern orthopedic practice. Computed tomography provides a definitive assessment of articular step-offs, gap formations, and the exact location of die-punch fragments within the intermediate column that may be obscured by osseous overlap on plain radiographs.




Imaging and Templating
Three-dimensional (3D) CT reconstructions are increasingly utilized to conceptualize the fracture morphology and plan fragment-specific fixation trajectories. Preoperative templating should be performed using digital templating software to determine the appropriate implant size, screw lengths, and plate configuration. The surgeon must decide whether a standard dorsal spanning plate, a fragment-specific dual-plate construct (orthogonal plating), or a dedicated spanning internal fixation plate (distraction plate) is required. In cases of carpal instability or planned arthrodesis, the exact angles of Kirschner wire or headless compression screw trajectories should be mapped out to avoid violating adjacent uninjured articulations. Templating also aids in anticipating the need for bone grafting, whether autograft from the iliac crest or distal radius, or synthetic allograft substitutes.

Patient Positioning and OR Setup
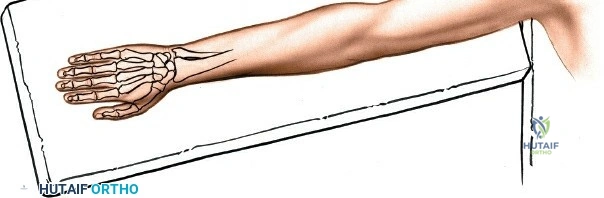
The patient is typically positioned supine on the operating table with the operative upper extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm to ensure a bloodless surgical field, typically inflated to 250 mmHg or 100 mmHg above the patient's systolic blood pressure. Regional anesthesia, such as a supraclavicular or axillary brachial plexus block, is heavily favored as it provides excellent intraoperative muscle relaxation and prolonged postoperative analgesia. The fluoroscopy unit (C-arm) should be positioned either parallel or perpendicular to the hand table, allowing for seamless transition between posteroanterior and lateral imaging without compromising the sterile field. The surgeon sits in the axilla facing the hand, with the surgical assistant positioned opposite, ensuring ergonomic access to the dorsal wrist.
Step-by-Step Surgical Approach and Fixation Technique
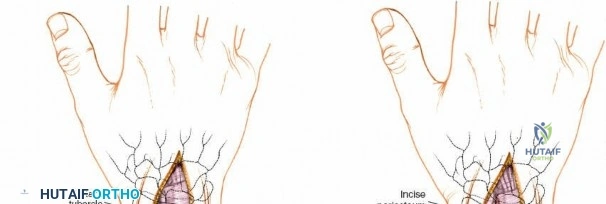
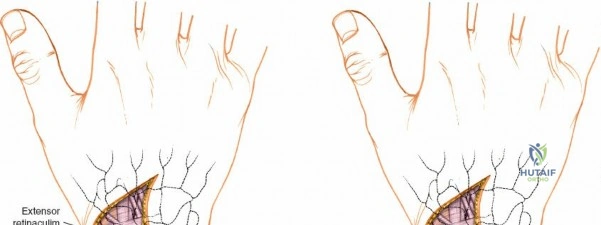
The surgical execution of the dorsal approach demands meticulous tissue handling and profound anatomical awareness. The procedure commences with an 8 to 10-centimeter longitudinal incision centered over Lister's tubercle, extending proximally along the distal radius and distally toward the base of the third metacarpal. While a straight incision is standard, a slight lazy-S or zigzag modification can be employed to cross the wrist crease obliquely, thereby minimizing the risk of a robust, restrictive scar contracture.


Superficial Dissection and Retinaculum Management
Following skin incision, dissection proceeds through the subcutaneous tissue. Extreme care is taken to identify, mobilize, and protect the superficial venous network and the terminal sensory branches of the superficial radial nerve and the dorsal ulnar sensory nerve. Retraction of these nerves should be gentle, utilizing vessel loops to prevent traction neuropraxia. The extensor retinaculum is then identified. The standard technique involves opening the third extensor compartment by incising the retinaculum longitudinally along the ulnar border of Lister's tubercle. The extensor pollicis longus (EPL) tendon is identified, mobilized, and transposed radially and subcutaneously.
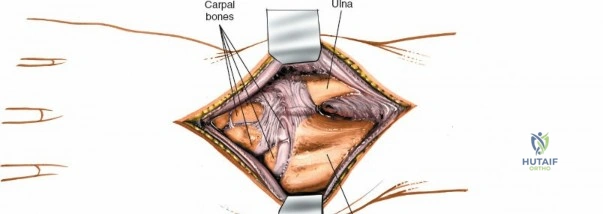
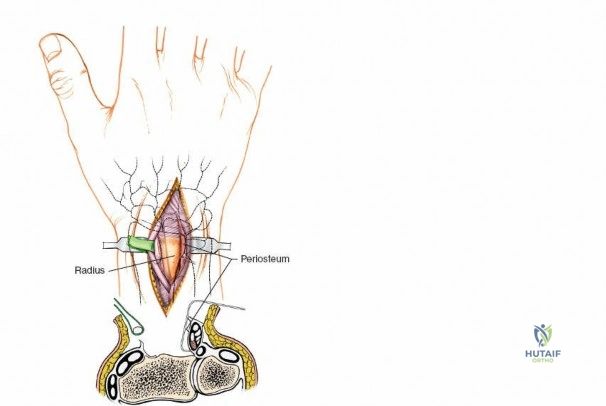
Once the EPL is transposed, the second and fourth extensor compartments are elevated subperiosteally from the dorsal radius. This subperiosteal elevation is a critical step; it preserves the floor of the compartments and the vertical septa, maintaining a smooth gliding surface for the extensor tendons and shielding them from direct contact with the underlying bone or future hardware. The posterior interosseous nerve, located on the floor of the fourth compartment, is identified and, if indicated for pain control, a neurectomy is performed by resecting a 1-centimeter segment of the nerve and burying the proximal stump into the interosseous membrane to prevent painful neuroma formation.
Capsulotomy and Articular Exposure
For procedures requiring access to the carpus or radiocarpal joint, a capsulotomy is performed. The ligament-sparing capsulotomy, popularized by Richard Berger, is the gold standard. This technique involves creating a distally based, V-shaped flap. The incision begins at the dorsal rim of the radius, runs distally along the dorsal intercarpal ligament, and then angles proximally along the dorsal radiocarpal ligament. This preserves the integrity of the intrinsic carpal ligaments. The capsular flap is reflected distally, exposing the scaphoid, lunate, and the articular surface of the distal radius. This exposure is paramount for visualizing articular step-offs, reducing die-punch fragments, and assessing scapholunate ligament integrity.
Reduction, Fixation, and Closure
Fracture reduction is achieved using a combination of manual traction, ligamentotaxis, and direct manipulation of fragments using dental picks or K-wire joysticks. Once anatomic reduction of the articular surface is confirmed visually and fluoroscopically, provisional fixation is achieved with 0.045-inch or 0.062-inch Kirschner wires. Definitive fixation is then applied using low-profile, fragment-specific dorsal plates. Modern constructs often utilize dual orthogonal plating (radial and intermediate column plates) to provide robust biomechanical stability while minimizing hardware prominence.
Following definitive fixation, the surgical site is copiously irrigated. The capsulotomy is meticulously repaired using non-absorbable or slowly absorbable sutures (e.g., 3-0 or 4-0 PDS) to restore carpal stability. The extensor retinaculum is then repaired; however, it is repaired deep to the extensor pollicis longus tendon. Leaving the EPL transposed in the subcutaneous tissue is a crucial maneuver to prevent tendon attrition and secondary rupture against the dorsal hardware. The subcutaneous tissues are approximated, and the skin is closed with non-absorbable monofilament sutures. A sterile dressing and a volar plaster splint are applied with the wrist in slight extension to relieve tension on the dorsal wound.
Com
