Arthroscopic Wafer Procedure & TFCC Debridement
Key Takeaway
The combined arthroscopic wafer distal ulnar resection and TFCC debridement is a minimally invasive technique for treating ulnocarpal impaction syndrome with central TFCC tears. By resecting the distal ulna through the TFCC defect, surgeons decompress the ulnocarpal joint while preserving the distal radioulnar joint ligaments. This guide details the step-by-step arthroscopic technique, biomechanical principles, and the modified Sauvé-Kapandji procedure for chronic derangement.
Comprehensive Introduction and Patho-Epidemiology
Ulnocarpal impaction syndrome (UIS), also frequently referred to as ulnar abutment syndrome, is a progressive, degenerative condition characterized by excessive load transmission across the ulnar aspect of the wrist. This pathological loading cascade leads to the systematic deterioration of the triangular fibrocartilage complex (TFCC), the chondral surfaces of the ulnar head, and the proximal ulnar carpus, specifically the lunate and triquetrum. Historically recognized as a primary source of ulnar-sided wrist pain, UIS is most commonly associated with a positive ulnar variance, which may be congenital, developmental, or acquired following distal radius fractures that heal with radial shortening or dorsal angulation. The insidious nature of this condition often results in delayed diagnosis, allowing the mechanical abutment to cause irreversible chondromalacia and complex, degenerative tears of the TFCC (Palmer Class 2 lesions).
The epidemiology of ulnocarpal impaction syndrome demonstrates a bimodal distribution, affecting both young, active individuals engaged in repetitive axial loading activities (such as gymnastics, racquet sports, and heavy manual labor) and an older demographic presenting with progressive degenerative changes secondary to prior trauma or age-related ligamentous laxity. Acquired positive ulnar variance is particularly prevalent in patients who have sustained Colles-type distal radius fractures treated non-operatively or with inadequate restoration of radial length. Furthermore, dynamic ulnar variance—where the ulna becomes relatively longer during forceful grip and forearm pronation—can precipitate symptomatic impaction even in patients whose resting static radiographs demonstrate neutral or slightly negative ulnar variance.
The patho-epidemiological progression of UIS follows a predictable sequence, initially described by Palmer. The cascade begins with central wear and fraying of the articular disc of the TFCC (Palmer 2A), progressing to full-thickness central perforations (Palmer 2B). As the ulnar head continues to abut the proximal carpal row, chondromalacia of the lunate and/or triquetrum develops (Palmer 2C). Left untreated, the continuous mechanical shear forces lead to disruption of the lunotriquetral (LT) ligament (Palmer 2D) and eventually culminate in end-stage ulnocarpal and distal radioulnar joint (DRUJ) osteoarthritis (Palmer 2E). Understanding this continuum is critical for the orthopedic surgeon, as the stage of the disease dictates whether a joint-preserving arthroscopic wafer procedure is viable or if a more extensive reconstructive salvage operation, such as a modified Sauvé-Kapandji procedure, is warranted.
The Combined Arthroscopic “Wafer” Distal Ulnar Resection and Triangular Fibrocartilage Complex Débridement, extensively popularized by Tomaino and Weiser, has revolutionized the management of early-to-mid-stage UIS. By resecting the distal 2 to 3 mm of the ulnar dome directly through a central TFCC defect, the surgeon effectively decompresses the ulnocarpal joint while avoiding the inherent morbidities of a formal diaphyseal ulnar shortening osteotomy (USO). This minimally invasive approach eliminates the need for internal fixation, circumvents the risk of diaphyseal nonunion, and allows for the simultaneous diagnostic evaluation and concurrent management of intra-articular pathology, making it an indispensable technique in the modern hand and wrist surgeon's armamentarium.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy of the ulnar aspect of the wrist is paramount for executing both the arthroscopic wafer procedure and complex DRUJ reconstructions safely. The triangular fibrocartilage complex (TFCC) is not a single structure but a complex network of ligaments and cartilaginous tissues that stabilize the DRUJ and cushion the ulnar carpus. The primary components include the central articular disc, the dorsal and volar radioulnar ligaments (DRUL and VRUL), the meniscus homologue, the ulnocarpal ligaments (ulnolunate and ulnotriquetral), and the extensor carpi ulnaris (ECU) tendon subsheath. The central articular disc is essentially avascular, receiving its limited blood supply only from the peripheral 10% to 20% of the surrounding capsular attachments. This avascularity explains why central tears (Palmer Class 2) possess no intrinsic healing capacity and must be managed with meticulous débridement rather than primary repair.
The peripheral attachments of the TFCC are the critical stabilizers of the distal radioulnar joint. The superficial fibers of the DRUL and VRUL attach to the base of the ulnar styloid, while the deep, stout foveal fibers attach to the fovea at the base of the ulnar head. These deep foveal attachments are the primary axis of forearm rotation and provide the majority of DRUJ stability. During an arthroscopic wafer procedure, the surgeon must operate strictly within the central, avascular zone of the articular disc. Iatrogenic violation of the peripheral DRUL or VRUL, or aggressive burring near the fovea, will inevitably result in catastrophic, iatrogenic DRUJ instability, transforming a simple decompression into a complex reconstructive nightmare.
The biomechanical rationale for ulnar decompression is deeply rooted in the landmark studies conducted by Palmer and Werner. Their in vitro biomechanical models established that in a physiologically normal wrist with neutral ulnar variance, the distal radius absorbs approximately 80% of the axial load transmitted across the radiocarpal joint, while the distal ulna absorbs the remaining 20%. However, the radioulnar load distribution is exquisitely sensitive to alterations in ulnar length. An increase in ulnar variance of merely 2.5 mm shifts the load distribution dramatically, increasing the ulnar load transmission from 20% to 42%. Conversely, a decrease in ulnar variance by 2.5 mm reduces the ulnar load transmission to a mere 4.3%. This exponential relationship underscores the mechanical efficacy of resecting just 2 to 3 mm of the ulnar head during a wafer procedure.
Kinematically, the DRUJ is a highly unconstrained articulation, relying heavily on its soft tissue envelope for stability throughout the arc of forearm rotation. During pronation, the radius crosses over the ulna, and the ulnar head translates dorsally within the sigmoid notch; during supination, the ulnar head translates volarly. Furthermore, forearm pronation dynamically increases positive ulnar variance by approximately 1 to 2 mm due to the proximal migration of the radius. This dynamic kinematic shift explains why patients with ulnocarpal impaction syndrome classically experience exacerbation of their symptoms during activities requiring forceful grip in terminal pronation. Surgical intervention, whether through a wafer resection or a Sauvé-Kapandji arthrodesis, must account for these dynamic forces to ensure complete decompression and functional restoration.
Exhaustive Indications and Contraindications
The decision-making algorithm for treating ulnocarpal impaction syndrome requires a nuanced evaluation of the patient's symptoms, structural anatomy, and the integrity of the distal radioulnar joint. The arthroscopic wafer procedure is an elegant, joint-preserving operation, but its success is entirely dependent on strict adherence to its specific indications. The ideal candidate is a patient presenting with classic ulnar-sided wrist pain, point tenderness over the ulnocarpal joint, and a positive ulnocarpal stress test (pain reproduced with the wrist in maximum ulnar deviation, extension, and forearm pronation). Radiographically, the patient should demonstrate a positive ulnar variance of less than 3 mm. Crucially, the DRUJ must be stable, congruent, and free of advanced osteoarthritic changes.
Conversely, attempting an arthroscopic wafer procedure in the presence of absolute contraindications will lead to predictable surgical failure and exacerbated patient morbidity. Positive ulnar variance exceeding 3 to 4 mm is a strict contraindication; attempting to resect more than 3 mm of the ulnar head arthroscopically risks violating the deep foveal attachments of the TFCC, leading to iatrogenic DRUJ instability, and often fails to adequately decompress the joint. In these cases, a formal diaphyseal ulnar shortening osteotomy (USO) is the gold standard. Furthermore, the presence of DRUJ arthritis or fixed DRUJ instability precludes both the wafer procedure and USO, necessitating a salvage procedure such as the Darrach resection, the hemiresection interposition arthroplasty (Bowers), or the modified Sauvé-Kapandji procedure.
Advanced imaging, specifically high-resolution magnetic resonance imaging (MRI) or MR arthrography, plays a pivotal role in refining surgical indications. MRI is invaluable for assessing the integrity of the peripheral TFCC, evaluating the cartilage of the ulnar head and sigmoid notch, and detecting early subchondral cystic changes in the lunate or triquetrum. If an MRI reveals a peripheral, vascular zone TFCC tear (Palmer Class 1B) in conjunction with positive ulnar variance, the surgeon must plan for an ulnar shortening osteotomy to decompress the joint, followed by primary arthroscopic or open repair of the peripheral tear. Debriding a peripheral tear during a wafer procedure is contraindicated, as it destroys the stabilizing structures of the DRUJ.
To assist in clinical decision-making, the following table delineates the strict indications and contraindications for the Arthroscopic Wafer Procedure versus the Modified Sauvé-Kapandji Procedure.
| Clinical Parameter | Arthroscopic Wafer Procedure | Modified Sauvé-Kapandji Procedure |
|---|---|---|
| Ulnar Variance | Positive variance < 3 mm | Positive variance > 3 mm (or severe deformity) |
| TFCC Pathology | Central, avascular tear (Palmer 2C/2D) | Irreparable destruction / End-stage degeneration |
| DRUJ Articular Cartilage | Intact, congruent, no osteoarthritis | Severe osteoarthritis / Post-traumatic destruction |
| DRUJ Stability | Stable (intact DRUL/VRUL/foveal fibers) | Chronic, fixed instability or painful subluxation |
| Patient Demographics | High-demand, heavy laborers, athletes | Low-to-moderate demand, older or salvage patients |
| Contraindications | Variance > 3mm, DRUJ arthritis, instability | Active infection, inadequate proximal bone stock |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning and flawless operating room setup are the cornerstones of successful wrist arthroscopy and complex reconstructive procedures. Planning begins with obtaining high-quality, standardized radiographs. The measurement of ulnar variance is highly dependent on radiographic technique; therefore, a "zero-rotation" posteroanterior (PA) view is mandatory. This is achieved by positioning the patient's shoulder abducted to 90 degrees, the elbow flexed to 90 degrees, and the forearm in neutral rotation, with the hand resting flat on the cassette. A pronated grip view should also be obtained to assess for dynamic ulnar variance, which may unmask occult impaction in a patient with static neutral variance.
Templating for an arthroscopic wafer procedure involves measuring the exact amount of positive variance on the zero-rotation PA radiograph and planning for a 2 to 3 mm resection. The surgeon must visualize the resection trajectory, ensuring the planned cut remains parallel to the articular surface of the radius and does not violate the sigmoid notch. For the modified Sauvé-Kapandji procedure, templating is even more critical. The surgeon must plan the level of the ulnar neck osteotomy, ensuring a precise 10 mm gap will be created to prevent postoperative radioulnar impingement, while leaving sufficient ulnar head bone stock for rigid lag screw fixation to the sigmoid notch.
Patient positioning and anesthesia require careful coordination with the surgical team. The procedure is typically performed under regional anesthesia, utilizing an ultrasound-guided supraclavicular or axillary brachial plexus block, supplemented with intravenous sedation or general anesthesia depending on patient anxiety and the anticipated duration of the surgery. The patient is positioned supine on the operating table with the operative arm extended on a specialized, radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. After standard sterile skin preparation and draping, the limb is exsanguinated using an Esmarch bandage, and the tourniquet is inflated to 250 mm Hg.
The traction setup is arguably the most critical aspect of the physical preparation for wrist arthroscopy. Sterile fingertraps are applied securely to the index and middle fingers. The arm is then suspended using a dedicated wrist arthroscopy tower. Longitudinal traction of 4.5 to 5.5 kg (10 to 12 lb) is applied. This specific weight range is non-negotiable; inadequate traction prevents sufficient joint distraction, leading to poor visualization and a high risk of iatrogenic scuffing of the delicate articular cartilage during trocar insertion. Conversely, excessive traction (>15 lbs) places the patient at significant risk for iatrogenic neuropraxia of the digital or superficial radial nerves, as well as profound ligamentous distraction. A countertraction strap is carefully applied across the distal biceps and secured to the operating table to maintain the distraction vector.
Step-by-Step Surgical Approach and Fixation Technique
Portal Placement and Diagnostic Arthroscopy
Accurate portal placement is the foundation of a safe and effective wrist arthroscopy. Prior to incision, the radiocarpal joint must be adequately distended to push the capsule away from the articular surfaces. Distension is achieved by injecting 5 to 10 mL of sterile saline solution either through the anatomic snuffbox or directly into the anticipated 3-4 portal site. The viewing portal is established at the 3-4 portal, located precisely between the extensor pollicis longus (EPL) and the extensor digitorum communis (EDC) tendons. A longitudinal skin incision is made, and a mosquito hemostat is used to bluntly dissect the subcutaneous tissues down to the capsule, meticulously sweeping away the terminal branches of the superficial radial nerve. A 2.7-mm or 1.9-mm, 30-degree arthroscope is introduced with a blunt trocar to avoid chondral injury.
Once intra-articular visualization is achieved, outflow must be established to maintain a clear visual field and prevent excessive fluid extravasation into the soft tissues. An 18-gauge needle or a dedicated outflow cannula is inserted into the radiostyloid-scaphoid joint space. Working portals are then established under direct intra-articular visualization using an outside-in technique with a spinal needle. The 4-5 portal (between the EDC and extensor digiti minimi [EDM]) and the 6R portal (radial to the extensor carpi ulnaris [ECU] tendon) are created. A systematic diagnostic sweep of the radiocarpal joint is performed, evaluating the articular surfaces of the scaphoid, lunate, and radius, and probing the intrinsic scapholunate and lunotriquetral ligaments.
TFCC Debridement and Preparation
The transition from diagnostic arthroscopy to therapeutic intervention begins with the management of the TFCC. In the setting of ulnocarpal impaction syndrome, the surgeon will typically encounter a central, degenerative tear of the articular disc (Palmer 2C or 2D). Because this central region is avascular and incapable of healing, it must be excised. Using a 2.0-mm or 2.9-mm motorized shaver or an arthroscopic punch introduced through the 4-5 or 6R portal, the surgeon carefully excises the frayed, degenerative margins of the central disc.
The goal of this débridement is twofold: to eliminate mechanical catching and to create a sufficient "window" to fully expose the underlying chondromalacic ulnar head. However, the surgeon must exercise extreme caution. The peripheral margins of the TFCC must be meticulously preserved. Aggressive resection extending into the dorsal or volar periphery will compromise the DRUL and VRUL, leading to iatrogenic DRUJ instability. The resection must be strictly confined to the central horizontal portion of the disc, leaving a robust peripheral rim intact.
Arthroscopic Wafer Resection
With the ulnar head exposed through the central TFCC window, the bony resection commences. The objective is to resect 2 to 3 mm of the distal ulna, effectively converting a positive ulnar variance to a neutral or slightly negative variance. Through the 6R portal, a 2.0-mm or 2.9-mm shielded arthroscopic burr is introduced. The resection trajectory begins on the radial side of the ulnar head. The surgeon removes the articular cartilage and subchondral bone to a depth equal to the width of the burr, providing a reliable intraoperative gauge for the depth of resection.
This resection must occur strictly beneath the margin of the sigmoid notch at the medial (ulnar) edge of the lunate fossa of the radius. The burr is gradually swept medially, toward the base of the ulnar styloid, carefully removing the ulnar head dome. To achieve adequate decompression, the surgeon must perform a "sub-TFCC resection." This involves placing the burr beneath the remaining intact peripheral triangular fibrocartilage, removing the ulnar head proximal to (beneath) the TFCC, extending to the base of the ulnar styloid. Once the resection appears visually adequate, traction is temporarily released. The surgeon passively pronates and supinates the wrist while viewing through the arthroscope to dynamically verify that there is no residual impingement between the ulnar head and the carpus throughout the full arc of motion.
Advanced Reconstruction: The Modified Sauvé-Kapandji Procedure
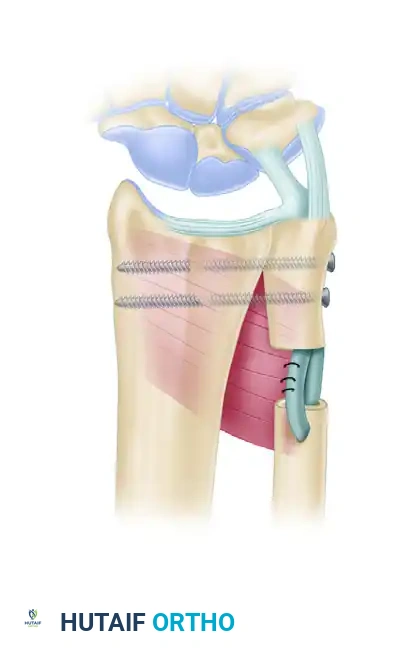
For patients presenting with chronic posttraumatic derangement of the DRUJ, severe DRUJ osteoarthritis, or fixed DRUJ instability, the arthroscopic wafer procedure is insufficient. These complex cases require a robust reconstructive salvage procedure. The classic Sauvé-Kapandji procedure involves an arthrodesis of the DRUJ combined with a proximal ulnar pseudarthrosis to restore forearm rotation. However, to address the frequent complication of painful instability of the proximal ulnar stump, the Modified Sauvé-Kapandji Procedure (described by Lamey and Fernandez) incorporates soft-tissue stabilization.
The approach utilizes a dorsal longitudinal incision over the DRUJ, operating through the fifth extensor compartment. The distal ulna and the DRUJ are exposed. The articular cartilage of the ulnar head and the corresponding sigmoid notch of the radius are aggressively decorticated down to bleeding subchondral bone to ensure a robust arthrodesis bed. An ulnar neck osteotomy is then performed. A segment of the ulnar neck is resected to create a gap measuring exactly 10 mm. This specific gap distance is critical; less than 10 mm risks bony impingement during forearm rotation, while more than 15 mm exacerbates proximal stump instability. The ulnar head is reduced into the sigmoid notch in neutral rotation and rigidly fixed using two 3.5-mm or 2.7-mm cortical lag screws.
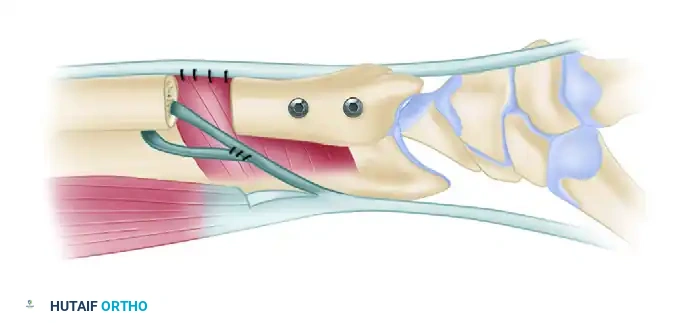
To prevent heterotopic ossification and stabilize the proximal ulnar segment, soft tissue interposition and tenodesis are meticulously performed. The pronator quadratus muscle is mobilized and interposed directly into the 10-mm nonunion gap, acting as a highly vascularized biological spacer. To address the dynamic instability of the proximal stump, a distally based slip of the flexor carpi ulnaris (FCU) tendon is harvested. This slip is routed through a transverse drill hole in the proximal ulnar segment to tether and stabilize it against the radius. Finally, the interposed pronator quadratus is sutured to the tendon sheath of the extensor carpi ulnaris (ECU) muscle, completing a robust soft tissue envelope.
Complications, Incidence Rates, and Salvage Management
While both the arthroscopic wafer procedure and the modified Sauvé-Kapandji procedure yield high rates of patient satisfaction when properly indicated, they are not without significant risks. Complications can arise from technical errors during surgery, poor patient selection, or inherent biomechanical failures of the construct. Recognizing these complications early and understanding the appropriate salvage pathways is essential for the operating surgeon.
In the arthroscopic wafer procedure, the most frequent complication is inadequate resection of the ulnar head. Because the volar-ulnar aspect of the ulnar head is notoriously difficult to visualize arthroscopically, surgeons often under-resect this quadrant. This leaves a residual bony prominence that continues to abut the triquetrum during forearm pronation, leading to persistent, recalcitrant pain. Radiographically, this presents as the "scallop sign," where the central dome is resected but the peripheral margins remain proud. Iatrogenic DRUJ instability is a less common but far more devastating complication, resulting from overzealous burring that violates the deep foveal attachments of the TFCC.
For the modified Sauvé-Kapandji procedure, complications are primarily related to the created pseudarthrosis. Despite the FCU tenodesis, dynamic convergence of the proximal ulnar stump toward the radius during heavy lifting or forceful grip can still occur, causing painful radioulnar impingement. Nonunion of the DRUJ arthrodesis is another critical failure point, often resulting from inadequate decortication of the subchondral sclerotic bone or insufficient lag screw compression.
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|
| Inadequate Resection (Wafer) | 5% - 10% | Dynamic intra-op testing without traction; rigorous sub-TFCC burring. | Revision arthroscopic resection or formal Open Ulnar Shortening Osteotomy. |
| Iatrogenic DRUJ Instability (Wafer) | < 2% | Confine resection to central 2-3mm; preserve peripheral TFCC rim strictly. | Open TFCC foveal repair or DRUJ ligamentous reconstruction (e.g., Adams-Berger). |
| Proximal Stump Instability (S-K) | 10% - 15% | Precise 10mm gap creation; robust FCU tenodesis and PQ interposition. | Revision soft-tissue stabilization; conversion to single-bone forearm (extreme salvage). |
| DRUJ Nonunion (S-K) | 3% - 5% | Aggressive decortication to bleeding bone; rigid, bi-cortical lag screw fixation. | Revision arthrodesis with autologous bone grafting and locking plate fixation. |
| Neuropraxia (Superficial Radial Nerve) | 2% - 4% | Blunt subcutaneous dissection during 3-4 and 4-5 portal placement. | Observation; gabapentinoids. Usually resolves spontaneously within 6-12 weeks. |
Phased Post-Operative Rehabilitation Protocols
Arthroscopic Wafer Procedure Rehabilitation
The postoperative rehabilitation following an arthroscopic wafer procedure is designed to balance the need for early mobilization to prevent stiffness with the necessity of protecting the healing capsular and portal incisions. The protocol is generally accelerated compared to open procedures due to the lack of osseous fixation.
- Days 1-10 (Immediate Post-Op Phase): The patient's wrist is immobilized in a bulky soft compressive dressing reinforced with a volar short-arm resting splint. The primary goals during this phase are edema control and the prevention of digital stiffness. Immediate, aggressive active range of motion (ROM) of the fingers and thumb is strongly encouraged. Elevation of the limb above the heart is mandatory.
- Weeks 2-4 (Early Mobilization Phase): At the first postoperative visit (typically day 10-14), the bulky splint is removed, and the portal sutures are extracted. The patient is transitioned to a custom-molded, removable thermoplastic wrist orthosis. Under the direct supervision of a certified hand therapist (CHT), gentle, active wrist flexion, extension, pronation, and supination are initiated. The orthosis is worn at all times except during hygiene and therapy sessions.
- Weeks 4-8 (Strengthening Phase): As pain and swelling subside, passive ROM exercises are introduced to regain terminal arcs of motion. Progressive isometric and isotonic strengthening exercises for the wrist and forearm musculature are incorporated. Heavy lifting, forceful gripping, and weight-bearing through the wrist remain strictly restricted until 8 weeks postoperatively to allow the resected cancellous bone bed of the ulnar head to fibrocartilaginous heal.
- Return to Play/Work: Most patients achieve maximal medical improvement and are cleared to return to unrestricted activities, heavy manual labor, and contact sports between 10 and 12 weeks postoperatively, provided they have achieved symmetrical grip strength and pain-free terminal rotation.
Modified Sauvé-Kapandji Procedure Rehabilitation
Rehabilitation following a modified Sauvé-Kapandji procedure is significantly more conservative, as the protocol must protect both the DRUJ arthrodesis site and the delicate soft-tissue tenodesis of the proximal ulnar stump.
- Weeks 1-4 (Immobilization Phase): Immediately postoperatively, the patient is placed in a Muenster-style cast or a long-arm cast. This rigid immobilization is critical to entirely restrict forearm pronation and supination, thereby protecting the lag screw fixation at the DRUJ and allowing the FCU tenodesis and pronator quadratus interposition to heal without shear forces. Digital ROM is encouraged.
- Weeks 4-8 (Transitional Phase): The long-arm cast is removed, and the patient is transitioned to a short-arm cast or a rigid custom thermoplastic splint. Serial radiographs are obtained to confirm the maintenance of hardware position and assess the early progression of the DRUJ arthrodesis. Gentle, active-assisted forearm rotation is initiated, but passive stretching is avoided to prevent stretching the proximal stump tenodesis.
- Weeks 8-12 (Consolidation Phase): Once definitive radiographic union of the DRUJ arthrodesis is confirmed (typically around 8-10 weeks), the splint is discontinued. Progressive strengthening of the forearm and wrist begins. The therapist and surgeon must closely monitor the patient for any clinical signs of proximal stump instability (clunking or pain proximal to the arthrodesis) during loaded rotation. Full unrestricted activity is rarely permitted before 16 weeks.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for ulnocarpal impaction syndrome is deeply rooted in several landmark biomechanical and clinical studies that have shaped modern orthopedic guidelines. The foundational understanding of wrist biomechanics was established by Palmer and Werner in 1984. Their seminal cadaveric studies definitively mapped the load transmission across the radiocarpal and ulnocarpal joints, proving mathematically that minor alterations in ulnar variance exponentially alter force distribution. This work provided the absolute biological rationale for all ulnar-shortening and decompression procedures.
The open wafer procedure was initially described by Feldon et al. in 1992, who reported an 85% good-to-excellent outcome rate in patients with positive ulnar variance and intact DRUJ ligaments. Feldon's work proved that partial resection of the ulnar head was clinically equivalent to diaphyseal shortening osteotomy for mild impaction, without the associated risks of nonunion or hardware irritation.
Building upon Feldon's open technique, Tomaino and Weiser revolutionized the approach by describing the Combined Arthroscopic Wafer Procedure. Their clinical series demonstrated that performing the resection arthroscopically through a central TFCC defect yielded equivalent biomechanical decompression while significantly reducing postoperative morbidity, accelerating rehabilitation, and allowing for the simultaneous treatment of concomitant intrinsic ligament tears. Modern clinical guidelines now strongly recommend the arthroscopic wafer procedure as the first-line surgical intervention for Palmer Class 2C/2D lesions with less than 3 mm of positive variance.
Finally, the management of end-stage DRUJ pathology was refined by Lamey and Fernandez in 1998. Recognizing the high failure rates of the classic Sauvé-Kapandji procedure due to proximal stump instability, they introduced the Modified Sauvé-Kapandji Procedure. By incorporating the pronator quadratus interposition and the
