Mastering Complete Wrist Arthrodesis: An Intraoperative Guide to Plate & Rod Fixation
Key Takeaway
This masterclass guides fellows through complete wrist arthrodesis, detailing patient selection, advanced imaging, and meticulous surgical planning. We cover two primary techniques: plate osteosynthesis for robust fixation and rod osteosynthesis for compromised bone. Fellows will master precise joint preparation, bone graft harvesting, hardware application, and vital neurovascular considerations, ensuring optimal outcomes for end-stage wrist arthritis.
Comprehensive Introduction and Patho-Epidemiology
Complete wrist arthrodesis represents a definitive, albeit motion-sacrificing, surgical intervention designed to reliably eradicate the debilitating pain associated with end-stage radiocarpal and intercarpal arthritis. While the modern orthopedic surgeon possesses an extensive armamentarium of motion-preserving procedures—ranging from proximal row carpectomy (PRC) to limited intercarpal fusions and total wrist arthroplasty—total wrist fusion remains the gold standard salvage procedure. It is the ultimate recourse when conservative measures have been exhausted, or when the destruction of the carpal architecture is too profound to support limited reconstructive efforts. The primary objective is unequivocal: to achieve a solid, stable, and completely pain-free wrist arthrodesis in a biomechanically functional position. This outcome is particularly critical for high-demand laborers, younger patients with post-traumatic arthritis, and individuals who rely heavily on their upper extremities for ambulation aids or transfers.
The pathophysiology of wrist arthritis is a complex cascade of biomechanical failure and cartilage degradation. The wrist is not a single hinge but a highly intricate, codependent system of articulations that rely on precise geometric alignment and ligamentous integrity to maintain smooth kinematics. When this system fails, the resulting altered force transmission rapidly accelerates articular wear. Osteoarthritis in the wrist is rarely idiopathic; it is most frequently secondary to specific kinematic disruptions. The most common etiologies include Scapholunate Advanced Collapse (SLAC) and Scaphoid Nonunion Advanced Collapse (SNAC). In these conditions, the uncoupling of the scaphoid and lunate leads to predictable patterns of progressive chondral wear, typically sparing the radiolunate joint until the absolute end stages.
Beyond post-traumatic degenerative changes, inflammatory arthropathies constitute a significant portion of the patient demographic requiring pan-carpal fusion. Rheumatoid arthritis, in particular, induces an aggressive, proliferative synovitis that systematically destroys the intrinsic and extrinsic ligaments, leading to profound carpal instability, ulnar translation of the carpus, and eventual global joint destruction. Other inflammatory conditions, such as crystalline arthropathies (gout and pseudogout), can similarly precipitate widespread articular devastation. Furthermore, septic arthritis, if not aggressively managed with prompt surgical debridement and targeted antimicrobial therapy, can rapidly obliterate the chondral surfaces, leaving complete arthrodesis as the only viable option to restore a functional, infection-free limb.
Before contemplating surgical intervention, the orthopedic surgeon must ensure that all nonoperative modalities have been rigorously trialed and have subsequently failed. The conservative management algorithm typically begins with activity modification and the judicious use of nonsteroidal anti-inflammatory drugs (NSAIDs) to mitigate acute inflammatory flares. Custom-fabricated orthoses, particularly rigid thumb spica splints or volar resting splints, are instrumental in restricting painful arcs of motion while allowing compensatory interphalangeal function. Intra-articular corticosteroid injections serve a dual purpose: providing transient symptomatic relief and acting as a diagnostic tool to confirm the primary locus of pain. For patients with systemic inflammatory diseases, optimization of disease-modifying antirheumatic drugs (DMARDs) and biologic therapies under the guidance of a rheumatologist is absolutely paramount before considering operative management.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the complex osseous and soft tissue anatomy of the wrist is the foundation of a successful arthrodesis. The carpus is composed of eight intricately shaped bones arranged in two distinct functional rows, intercalated between the distal radius and the metacarpal bases. The distal carpal row—comprising the trapezium, trapezoid, capitate, and hamate—functions biomechanically as a single unit tightly bound to the metacarpal bases via stout ligaments. This rigid distal segment exhibits minimal interosseous motion and serves as the primary load-bearing platform for the hand. Conversely, the proximal carpal row—consisting of the scaphoid, lunate, and triquetrum—acts as an intercalated segment with no direct tendinous insertions. Its motion is entirely dependent on the mechanical forces exerted by the surrounding articulations and the integrity of the intrinsic interosseous ligaments, particularly the scapholunate and lunotriquetral ligaments.
The radiocarpal articulation, formed by the distal radius and the proximal surfaces of the scaphoid and lunate, is the primary site of wrist flexion and extension, as well as radial and ulnar deviation. The midcarpal joint, situated between the proximal and distal rows, contributes significantly to the global arc of wrist motion. Biomechanically, normal wrist function relies on the "dart-thrower's motion," an oblique plane of movement from radial extension to ulnar flexion. Complete wrist arthrodesis deliberately obliterates these kinematic pathways. By fusing the radius to the proximal row, the proximal row to the distal row, and the distal row to the metacarpals, the surgeon converts this multi-articulated chain into a single, rigid lever arm.
The surgical approach to the wrist necessitates meticulous navigation of the dorsal soft tissue envelope, specifically the extensor retinaculum and its six distinct fibro-osseous compartments. Lister's tubercle, a prominent bony landmark on the dorsal aspect of the distal radius, serves as the critical anatomical signpost. It separates the second extensor compartment (extensor carpi radialis longus and brevis) from the third compartment, which houses the extensor pollicis longus (EPL) tendon. The EPL tendon takes an oblique course around Lister's tubercle, making it highly susceptible to iatrogenic injury or postoperative attrition against prominent hardware. The fourth extensor compartment, containing the extensor digitorum communis and extensor indicis proprius, lies immediately ulnar to Lister's tubercle and must be subperiosteally elevated to expose the dorsal radiocarpal capsule.
Deep to the extensor tendons lies the posterior interosseous nerve (PIN), a terminal branch of the radial nerve. The PIN provides critical nociceptive sensory innervation to the dorsal wrist capsule. Routine identification and prophylactic excision of a segment of the PIN during the dorsal approach is a standard adjunctive procedure in wrist arthrodesis. This targeted neurectomy serves to denervate the dorsal capsule, significantly reducing postoperative pain and mitigating the risk of painful neuroma formation within the surgical scar. Furthermore, surgeons must remain acutely aware of the vascular anatomy, particularly the dorsal branches of the radial artery that supply the dorsal carpal arch, ensuring these structures are protected during radial retraction and capsular elevation.
Exhaustive Indications and Contraindications
The decision to proceed with a complete wrist arthrodesis is highly nuanced and must be individualized to the patient's specific pathology, functional demands, and physiological status. The primary indication is intractable, end-stage pan-carpal arthritis that has proven refractory to all conservative measures. This encompasses severe SLAC or SNAC wrist (Stage III or IV), advanced Kienböck's disease with secondary global arthrosis, and end-stage rheumatoid arthritis characterized by profound carpal collapse and instability. Complete arthrodesis is also the procedure of choice for post-traumatic conditions resulting in massive carpal bone loss, severe spastic contractures of the wrist (as seen in cerebral palsy or severe traumatic brain injury), and as a salvage operation for failed total wrist arthroplasty or failed limited intercarpal fusions.
Conversely, absolute contraindications are relatively few but must be strictly respected. Active, untreated local or systemic infection precludes the implantation of extensive orthopedic hardware and bone grafting. In the pediatric population, complete wrist arthrodesis is absolutely contraindicated in the presence of open physes, as surgical violation of the distal radial growth plate will result in premature growth arrest and severe subsequent deformity. Relative contraindications require careful clinical judgment and often a multidisciplinary approach. Patients with severe osteopenia or osteoporosis may lack the necessary bone stock to achieve adequate screw purchase for plate osteosynthesis, necessitating alternative fixation methods such as intramedullary rod fixation or specialized locking plate constructs.
The patient's functional requirements and handedness play a pivotal role in the decision-making process. For the dominant extremity, patients are often highly motivated to preserve any residual motion to facilitate activities of daily living, such as writing or personal hygiene. In these scenarios, motion-preserving salvage procedures might be aggressively pursued, even if it means accepting a low level of chronic pain. However, for the non-dominant extremity, or in patients whose primary limitation is a lack of grip strength due to pain, complete arthrodesis offers a profound functional improvement by providing a stable, pain-free platform for hand function.
| Category | Specific Conditions | Clinical Considerations |
|---|---|---|
| Absolute Indications | End-stage SLAC/SNAC (Stage III/IV) | Global articular destruction precluding limited fusion. |
| Advanced Rheumatoid Arthritis | Severe carpal collapse, ulnar translation, uncorrectable instability. | |
| Failed Total Wrist Arthroplasty | Massive bone loss requiring rigid structural salvage. | |
| Spastic Wrist Contractures | Severe cerebral palsy or TBI requiring positional correction. | |
| Post-Traumatic Global Arthrosis | Irreparable intra-articular fractures with secondary OA. | |
| Relative Indications | Kienböck's Disease (Lichtman Stage IV) | When proximal row carpectomy is contraindicated due to capitate wear. |
| Brachial Plexus Palsy | To provide a stable terminal lever arm for tendon transfers. | |
| Absolute Contraindications | Active Local/Systemic Infection | High risk of deep hardware infection and osteomyelitis. |
| Skeletally Immature Patients | Risk of iatrogenic physeal arrest and severe growth deformity. | |
| Relative Contraindications | Severe Osteoporosis | Poor bone stock compromising plate and screw purchase. |
| Non-Compliant Patients | Inability to adhere to strict postoperative immobilization protocols. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the absolute cornerstone of a successful complete wrist arthrodesis. The diagnostic workup must begin with high-quality, orthogonal radiographs of the affected wrist, including standard posteroanterior (PA), lateral, and oblique views. These images are scrutinized to assess the degree of carpal collapse, the presence of subchondral sclerosis or cyst formation, and the overall alignment of the carpus relative to the radius and metacarpals. In cases of complex post-traumatic deformity or when assessing bone stock for hardware placement, a fine-cut Computed Tomography (CT) scan is indispensable. The CT scan provides a three-dimensional understanding of the osseous architecture, allowing the surgeon to precisely map out the areas of maximal bone loss and plan for necessary structural bone grafting.
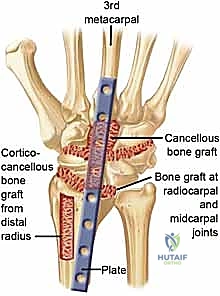
Hardware selection is a critical component of the preoperative strategy. The modern standard for complete wrist arthrodesis is rigid plate osteosynthesis using specifically designed, pre-contoured dorsal wrist fusion plates. These plates are engineered to span from the distal radius to the third metacarpal and are typically pre-bent to provide 20 to 30 degrees of wrist extension. This slight extension is biomechanically optimal, as it maximizes the tension in the extrinsic flexor tendons, thereby optimizing grip strength. Straight plates may be utilized but require manual contouring intraoperatively. In contrast, intramedullary rod osteosynthesis (using stout Steinmann pins) is often reserved for patients with severe inflammatory arthritis, profound bone loss, or compromised soft tissue envelopes where a bulky dorsal plate might lead to wound breakdown. Rods are typically placed to achieve a neutral wrist position, which is often preferred by rheumatoid patients to facilitate perineal care and other specific activities of daily living.

Medical optimization prior to surgery is mandatory. Patients on anticoagulant therapy (e.g., Warfarin, direct oral anticoagulants) must have these medications appropriately withheld or bridged according to established perioperative protocols to mitigate the risk of catastrophic hematoma formation and subsequent soft tissue compromise. For patients with inflammatory arthropathies, coordination with the treating rheumatologist is essential to manage biologic agents and DMARDs, balancing the risk of perioperative infection against the risk of a severe disease flare. Digital templating using the preoperative radiographs is strongly recommended. Templating allows the surgeon to accurately predict the required plate length, anticipate screw trajectories, and ensure that the chosen hardware will adequately span the radiocarpal and carpometacarpal joints without impinging on adjacent articulations.
Patient positioning in the operating room sets the stage for the entire procedure. The patient is positioned supine on the operating table with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal brachium to provide a bloodless surgical field, which is critical for meticulous joint decortication and precise hardware placement. Before the induction of general or regional anesthesia, the surgeon must carefully assess the patient’s comfortable range of shoulder motion. The arm board must be positioned such that it does not force the shoulder into excessive abduction or external rotation, which could precipitate devastating postoperative brachial plexopathy or exacerbate pre-existing shoulder pathology, a common comorbidity in the rheumatoid population.
Step-by-Step Surgical Approach and Fixation Technique
Dorsal Approach and Exposure
The procedure commences with a longitudinal, midline dorsal incision centered over the radiocarpal joint, extending from the distal third of the radius to the mid-shaft of the third metacarpal. The incision is strategically placed just ulnar to Lister's tubercle. Meticulous subcutaneous dissection is performed, taking great care to identify and retract the dorsal sensory branches of the radial and ulnar nerves, as well as superficial venous structures. The extensor retinaculum is then identified, and a longitudinal incision is made directly over the third extensor compartment. The extensor pollicis longus (EPL) tendon is mobilized from its sheath and retracted radially with a vessel loop. This transposition is critical; it not only provides access to the underlying radiocarpal joint but also permanently relocates the EPL out of its native compartment, preventing postoperative attrition rupture against the dorsal fusion plate.
Following EPL transposition, the fourth extensor compartment (containing the extensor digitorum communis and extensor indicis proprius) is sharply incised along its radial border. Using a sharp periosteal elevator, the entire fourth compartment is elevated subperiosteally from the dorsal aspect of the distal radius and retracted ulnarly. This wide subperiosteal elevation exposes the dorsal radiocarpal ligament and the underlying joint capsule. At this juncture, the posterior interosseous nerve (PIN) is routinely identified on the floor of the fourth compartment. A 1 to 2-centimeter segment of the PIN is sharply excised, and the proximal stump is allowed to retract into the deep musculature to prevent painful neuroma formation. A robust, U-shaped or longitudinal capsulotomy is then performed, elevating the dorsal capsule as a thick, full-thickness flap to expose the radiocarpal, midcarpal, and carpometacarpal articulations.

Joint Preparation and Decortication
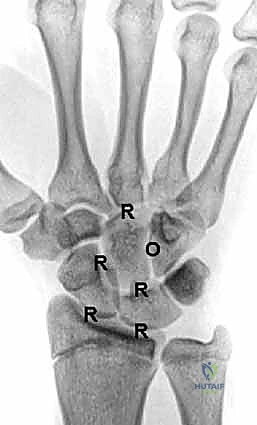
The success of any arthrodesis is fundamentally dependent on the meticulous preparation of the articular surfaces. The goal is to completely eradicate all remaining hyaline cartilage and expose healthy, bleeding subchondral bone to facilitate robust osteogenesis. Using a combination of a #15 scalpel blade, sharp curettes of varying sizes, and small rongeurs, the surgeon systematically denudes the specific joints targeted for fusion. For a complete wrist arthrodesis utilizing a plate fixed to the third metacarpal, the requisite joints for decortication include the radioscaphoid, radiolunate, scaphocapitate, capitolunate, and the third carpometacarpal joint. While the triquetrolunate and other ulnar-sided joints may technically be left intact if asymptomatic, most surgeons prefer a pan-carpal decortication to maximize the total surface area available for the fusion mass.

In areas of severe eburnation and subchondral sclerosis, manual curettage is often insufficient. A high-speed, water-cooled pneumatic burr (such as a 3mm matchstick or round burr) is utilized to meticulously remove the sclerotic bone down to a vascularized cancellous bed. Extreme care must be taken during burring to avoid thermal necrosis of the bone, hence the necessity of continuous, copious saline irrigation. To further stimulate the local osteogenic response, the denuded subchondral surfaces are repeatedly fenestrated or "shingled" using a 0.045-inch smooth Kirschner wire or a fine drill bit. This process opens the medullary canals of the carpal bones, allowing the influx of osteoprogenitor cells and marrow elements into the fusion site. If significant bone voids are present following decortication, cancellous autograft (typically harvested from the distal radius or iliac crest) or high-quality allograft must be packed tightly into the interstices to ensure structural continuity.

Plate and Screw Osteosynthesis
With the joints meticulously prepared, the focus shifts to rigid internal fixation. The pre-contoured dorsal wrist fusion plate is introduced into the surgical field. The plate is positioned such that its proximal segment lies flat against the flat dorsal surface of the distal radius, while its distal segment rests securely on the dorsal cortex of the third metacarpal. Intraoperative fluoroscopy is utilized extensively at this stage to confirm optimal plate positioning in both the coronal and sagittal planes. The surgeon must ensure that the pre-contoured bend of the plate aligns perfectly with the radiocarpal joint, imparting the desired 20 to 30 degrees of extension and approximately 5 to 10 degrees of ulnar deviation, which optimizes the biomechanical axis of the hand.
Fixation typically begins distally. A non-locking cortical screw is placed through the oblong hole in the distal segment of the plate into the diaphysis of the third metacarpal. This allows for minor proximal-distal adjustments. Once the distal position is confirmed, a corresponding non-locking screw is placed in the proximal oblong hole on the radial shaft. With the plate provisionally secured, the surgeon applies axial compression across the carpus. This can be achieved manually or by using an articulated tensioning device. The remaining screw holes are then systematically filled. Modern plate designs incorporate specialized locking holes over the carpal segment, allowing for the insertion of locking screws into the capitate and occasionally the lunate or scaphoid. This creates a highly stable, fixed-angle construct that is highly resistant to pullout, even in osteopenic bone.
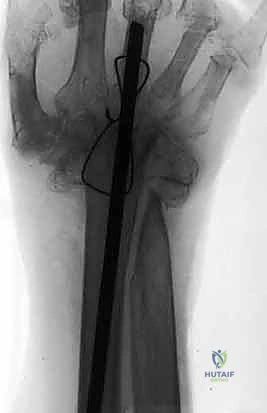
Intramedullary Rod Osteosynthesis
In scenarios where plate fixation is contraindicated—such as in severe rheumatoid arthritis with profound osteopenia, compromised dorsal soft tissues, or when a neutral wrist position is specifically desired—intramedullary rod osteosynthesis is an excellent alternative. Following identical joint preparation, a stout Steinmann pin (typically 1/8 inch or 3.2mm) is utilized. The pin is introduced retrogradely. It is driven distally through the capitate and down the medullary canal of the third metacarpal until it exits the metacarpophalangeal (MCP) joint with the joint held in maximal flexion. The pin is then advanced until its proximal tip is flush with the proximal articular surface of the capitate.
The wrist is then carefully reduced into a neutral alignment. The Steinmann pin is driven proximally, crossing the radiocarpal joint and advancing deep into the medullary canal of the distal radius. Fluoroscopy is critical to ensure the pin remains centrally located within the radial canal and does not breach the volar or dorsal cortices. Often, a second, parallel or slightly divergent pin is placed through the second or fourth metacarpal to provide rotational stability to the construct. The distal ends of the pins are cut flush with the metacarpal head beneath the articular cartilage, or left slightly prominent dorsally for planned removal once radiographic union is achieved. The dorsal capsule is then meticulously repaired over the hardware, and the EPL tendon is left transposed in the subcutaneous tissues prior to layered skin closure.

Complications, Incidence Rates, and Salvage Management
While complete wrist arthrodesis is generally a highly successful and reliable procedure, it is not without the potential for significant complications. The orthopedic surgeon must be intimately familiar with these risks, their incidence, and the appropriate salvage strategies. The most concerning complication is nonunion or pseudarthrosis, which occurs in approximately 2% to 5% of cases. Nonunion most frequently occurs at the carpometacarpal (CMC) articulation, particularly the third CMC joint, due to the high shear forces experienced at this interface. Risk factors for nonunion include inadequate joint decortication, failure to utilize bone graft in the presence of voids, smoking, and the use of non-rigid fixation techniques. Management of a symptomatic nonunion requires revision surgery, aggressive debridement of the pseudarthrosis, copious autogenous bone grafting, and revision of the internal fixation construct, often upgrading to a more robust locking plate system.
Hardware-related complications are relatively common, particularly with dorsal plate osteosynthesis. The dorsal soft tissue envelope of the wrist is exceptionally thin, and prominent plates or screw heads can lead to significant tenosynovitis, tendon attrition, and ultimately, tendon rupture. The extensor pollicis longus (EPL) and extensor digitorum communis (EDC) tendons are at the highest risk. The incidence of hardware removal due to symptomatic prominence ranges from 10% to 15%. To mitigate this risk, meticulous closure of the extensor retinaculum over the plate (if possible) or utilizing local capsular flaps to interpose between the hardware and the tendons is crucial. If a tendon rupture occurs, salvage options include tendon transfers (e.g., extensor indicis proprius to EPL transfer) combined with immediate hardware removal once solid bony union is confirmed.
Postoperative infection, while rare (incidence < 2%), is a devastating complication that threatens the viability of the entire fusion construct. Superficial wound infections can often be managed with targeted oral antibiotics and local wound care. However, deep space infections involving the hardware require aggressive surgical intervention. The standard protocol involves immediate surgical debridement, copious irrigation, and obtaining deep tissue cultures. If the hardware remains rigidly fixed and the infection is acute, the hardware may occasionally be retained while the patient undergoes a prolonged course of intravenous antibiotics. However, if the hardware is loose or the infection is chronic, all hardware must be explanted. The wrist is then stabilized with an external fixator or a temporary antibiotic spacer until the infection is eradicated, at which point a revision arthrodesis can be attempted.
| Complication | Estimated Incidence | Primary Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Nonunion / Pseudarthrosis | 2% - 5% | Inadequate decortication, smoking, poor bone stock, insufficient fixation. | Revision arthrodesis, autogenous bone grafting, upgraded rigid fixation. |
| Hardware Prominence / Pain | 10% - 15% | Thin dorsal soft tissue envelope, inadequate plate contouring. | Hardware removal (only after solid radiographic union is confirmed). |
| Extensor Tendon Rupture | 1% - 3% | Attrition against prominent plate or screw heads (EPL most common). | Hardware removal, tendon transfer (e.g., EIP to EPL). |
| Deep Surgical Site Infection | < 2% | Rheumatoid arthritis, chronic steroid use, prolonged operative time. | Aggressive I&D, IV antibiotics. Hardware removal if loose or chronic. |
| Carpal Tunnel Syndrome | 2% - 5% | Altered carpal arch mechanics, postoperative edema, hematoma. | Carpal tunnel release (can be done concurrently if pre-existing). |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a complete wrist arthrodesis is a structured, phased process designed to protect the surgical construct while maximizing the functional recovery of the adjacent, non-fused joints. The immediate postoperative phase (Days 0 to 14) focuses on edema control, pain management, and the protection of the soft tissue envelope. The patient is placed in a bulky, well-padded short arm volar splint in the operating room. Strict elevation of the operative extremity above the level of the heart is mandatory to minimize swelling. Crucially, immediate, active range of motion of all digits (metacarpophalangeal and interphalangeal joints), as well as the elbow and shoulder, is strongly encouraged starting on postoperative day one. This prevents secondary stiffness and encourages venous and lymphatic return.
At the two-week postoperative mark, the patient returns to the clinic for the first wound check and suture removal. If the surgical incisions are well-healed, the bulky splint is transitioned to a custom-molded, removable thermoplastic short arm orthosis or a short arm fiberglass cast, depending on the surgeon's preference and the patient's compliance level. During this intermediate phase (Weeks 2 to 6), the primary goal remains the protection of the arthrodesis site. The patient is instructed to wear the orthosis strictly at all times, removing it only for hygiene and supervised therapy sessions. Occupational therapy is formally initiated, focusing on aggressive digital range of motion, intrinsic muscle strengthening, and scar mobilization techniques to prevent tethering of the extensor tendons.
The late postoperative phase begins around 6 to 8 weeks, contingent upon radiographic evidence of progressive bony consolidation. Radiographs are scrutinized for the presence of bridging trabecular bone across the radiocarpal and midcarpal joints. Once clinical and radiographic union is confirmed, the patient is gradually weaned from the rigid orthosis. Strengthening exercises are initiated, focusing on grip and pinch strength. Patients must be counseled that while pain relief is typically profound and immediate, maximal grip strength recovery may take up to 12 to 18 months to plateau. The final functional outcome is a stable, painless wrist that allows for powerful grip, though patients must adapt to the permanent loss of wrist flexion and extension by utilizing compensatory movements at the elbow and shoulder.
Summary of Landmark Literature and Clinical Guidelines
The evolution of complete wrist arthrodesis is deeply rooted in the historical literature, transitioning from rudimentary pin fixation to the sophisticated, biomechanically optimized plate constructs utilized today. Early techniques, popularized by Mannerfelt and Malmsten in the 1970s, relied heavily on intramedullary rush pins or Steinmann pins, particularly in the rheumatoid population. While successful in achieving fusion, these techniques often lacked the rigidity required for early mobilization and were associated with higher rates of hardware migration. The paradigm shifted significantly with the application of AO (Arbeitsgemeinschaft für Osteosynthesefragen) principles to the wrist. The landmark studies by Hastings and others in the 1980s and 1990s demonstrated that rigid dorsal plate osteosynthesis dramatically reduced nonunion rates and allowed for more predictable functional outcomes
