Fingertip Amputation Reconstruction: An Intraoperative Masterclass in Soft Tissue Coverage

Key Takeaway
This masterclass guides fellows through advanced soft tissue coverage for fingertip amputations. We'll meticulously cover comprehensive surgical anatomy, critical preoperative planning, and real-time, step-by-step intraoperative execution of various flap and graft techniques. Learn to manage neurovascular risks, optimize patient outcomes, and navigate potential pitfalls with expert precision, ensuring functional and aesthetic restoration of the most sensitive area of the hand.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to this definitive masterclass in reconstructive hand surgery. Today, we are tackling a ubiquitous yet profoundly challenging clinical entity: the fingertip amputation. The human fingertip is an evolutionary marvel, representing the most sensitive, functionally critical, and anatomically specialized region of the upper extremity. It is the primary interface between the human intellect and the physical environment. Our overarching objective in the surgical management of these injuries transcends mere wound closure; it demands the meticulous preservation of digital length, the restoration of critical tactile sensation, and the provision of robust, durable soft tissue coverage to optimize terminal pinch and grip kinematics. Achieving these goals requires a nuanced, almost microscopic understanding of regional anatomy, flawless execution of soft tissue handling, and a highly tailored, algorithmic approach to each unique structural defect.
Fingertip injuries and terminal amputations are defined precisely as traumatic disruptions to the digit occurring distal to the terminal insertion of the extensor and flexor tendons, typically demarcated by the distal interphalangeal (DIP) joint crease. Epidemiologically, these injuries are remarkably prevalent, accounting for approximately 45% of all hand trauma presentations in emergency departments globally. The mechanisms of injury exhibit significant heterogeneity, ranging from high-energy avulsions, severe industrial crush injuries, and hydraulic compression traumas to sharp lacerations and low-velocity dull impacts. Understanding the specific vector and energy of the trauma is paramount, as a high-velocity crush injury imparts a zone of injury that extends far proximally to the visible wound edge, profoundly altering flap viability and reconstructive decision-making.
The natural history of fingertip trauma is heavily dictated by the presence or absence of exposed osseous or tendinous structures. Injuries devoid of exposed bone, particularly those measuring less than 1 square centimeter, possess a remarkable capacity to heal by secondary intention. This conservative approach, facilitated by meticulous daily wound care and semi-occlusive dressings, often yields exceptional sensory recovery due to the centripetal contraction of the highly innervated surrounding pulp skin. However, for larger defects, or those involving exposed distal phalanx or articular cartilage, secondary intention becomes fraught with unacceptable risks. Prolonged healing times predispose the patient to deep space infections, debilitating joint stiffness, and the development of fragile, atrophic scars that are highly susceptible to recurrent breakdown and exquisite cold intolerance.
Therefore, the modern orthopedic hand surgeon must be armed with an expansive armamentarium of reconstructive techniques. The decision matrix involves weighing the patient's physiological age, hand dominance, occupational demands, and compliance against the geometric realities of the defect. A concert pianist with a volar oblique amputation of the dominant index finger demands a vastly different reconstructive paradigm than a retired, sedentary individual with a transverse amputation of the non-dominant small finger. This chapter will exhaustively detail the anatomical foundations, preoperative algorithms, and step-by-step intraoperative execution required to master fingertip reconstruction.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel is ever mounted, a profound, three-dimensional comprehension of fingertip anatomy is mandatory. The fingertip is not merely skin overlying bone; it is a highly specialized sensory organ integrated with a complex appendage, the nail complex. The biomechanical interplay between the rigid distal phalanx, the stabilizing nail plate, and the compliant, fluid-filled pulp dictates the efficiency of the human pinch mechanism. Observe the intricate cross-sectional anatomy, which serves as the foundation for all reconstructive efforts.
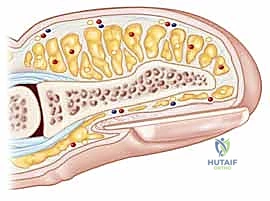
The nail complex itself is a masterpiece of specialized epithelium. The eponychium (cuticle) represents the thin, specialized membrane overlying the dorsum of the nail at the proximal nail fold, forming a critical waterproof seal against environmental pathogens. Laterally, the perionychium encompasses the skin at the lateral nail margins, providing structural containment. Distally, the hyponychium is situated beneath the distal free edge of the nail plate. This region consists of a dense mass of keratin heavily populated with lymphocytes and polymorphonuclear leukocytes, serving as the first line of immunological defense against subungual infections. Proximal to this lies the nail root, nestled deep within the eponychial fold, where the continuous process of onychopoiesis (nail growth) is initiated.
The matrix of the nail is functionally bifurcated. The lunula, the visible, opaque, crescent-shaped structure at the base of the nail, represents the distal-most extent of the germinal matrix. This germinal matrix is the biological powerhouse of the nail complex, responsible for generating approximately 90% of the nail plate's volume. Any iatrogenic or traumatic injury to this region will almost certainly result in permanent, aesthetically and functionally displeasing nail deformities. Distal to the lunula lies the sterile matrix, which, while contributing minimally to nail volume, is absolutely essential for the dense adherence of the nail plate to the underlying bed. The nail plate itself is a rigid structure composed of flattened, anuclear, keratinized epithelial cells, providing dorsal protection and acting as a rigid counter-board that enhances the tactile sensitivity of the volar pulp during pinch.

Ventrally, the pulp is a highly specialized, densely innervated, and richly vascularized connective tissue pad. It is compartmentalized by robust fibrous septa that traverse from the volar dermis to the periosteum of the distal phalanx. These septa functionally tether the skin, preventing sheer during power grip and pinch, but they also create closed compartments that can rapidly succumb to ischemic necrosis in the setting of a closed space infection (felon). The vascular and sensory supply is delivered via the proper palmar neurovascular bundles. These structures run volarly along the digit, arborizing extensively at the level of the DIP joint to form a rich anastomotic arcade. Locating and preserving these bundles, which lie just dorsal and lateral to the flexor tendon sheath, is the absolute crux of safely executing advancement flaps.
Exhaustive Indications and Contraindications
The selection of the appropriate reconstructive modality is governed by a strict algorithmic approach, primarily dictated by the geometry of the amputation, the presence of exposed bone, and patient-specific factors. We frequently utilize the Allen Classification to categorize these injuries: Type I involves only the pulp; Type II involves the pulp and nail bed; Type III includes a fracture of the distal phalanx; and Type IV represents an amputation proximal to the lunula. Furthermore, the angle of the amputation—transverse, volar oblique, or dorsal oblique—heavily influences flap selection.
A critical error made by junior surgeons is the failure to recognize when a seemingly simple closure is contraindicated. Primary closure under tension is a catastrophic mistake in the fingertip. Attempting to forcibly approximate volar skin to the dorsal nail bed over a shortened distal phalanx will inevitably result in a "hook nail" deformity, severe distal tip tenderness, and potentially, ischemic necrosis of the advanced skin edge. If tension-free primary closure is impossible, the surgeon must immediately pivot to either bone shortening (if functionally acceptable) or soft tissue flap coverage.
The following table delineates the strict indications and contraindications for the most frequently utilized reconstructive techniques in fingertip amputations. Mastery of this decision matrix is non-negotiable for the operating surgeon.
| Reconstructive Technique | Primary Indications | Absolute/Relative Contraindications |
|---|---|---|
| Secondary Intention | Defect < 1 cm²; No exposed bone/tendon; Pediatric patients; Non-compliant patients unable to tolerate surgery. | Exposed distal phalanx; Exposed flexor/extensor tendon; Defects > 1.5 cm²; Need for rapid return to manual labor. |
| Full-Thickness Skin Graft (FTSG) | Clean, well-vascularized defect > 1 cm²; No exposed avascular structures (bone/tendon without paratenon/periosteum). | Exposed bare bone or tendon; Heavily contaminated or crushed wound beds; Active infection; Poor donor site availability. |
| V-Y Advancement Flap (Atasoy) | Transverse or dorsal oblique amputations; Exposed distal phalanx; Need for durable, sensate tip coverage. | Volar oblique amputations (insufficient volar tissue); Extensive crush injury to the volar pulp; Proximal amputations (Allen Type IV). |
| Volar Advancement Flap (Moberg) | Thumb amputations up to 1.5 cm; Need to preserve thumb length and volar sensation. | Use in fingers other than the thumb (high risk of dorsal tip necrosis due to different vascular anatomy); Severe joint stiffness. |
| Cross-Finger Flap | Large volar oblique defects; Extensive exposed bone/tendon on the volar aspect; Failure of local advancement flaps. | Rheumatoid arthritis or preexisting stiffness in the donor digit; Advanced age (>60) due to stiffness risk; Uncooperative patient. |
Pre-Operative Planning, Templating, and Patient Positioning
The success of any soft tissue reconstruction is predicated upon exhaustive preoperative planning and meticulous patient positioning. The history and physical examination must be forensic in nature. We must ascertain the exact mechanism of injury, as a hydraulic press injury will mandate a much wider zone of debridement than a clean laceration from a kitchen knife. The patient's age, hand dominance, and specific occupational requirements must be documented, as these factors will dictate the aggressiveness of our reconstructive efforts. A rigorous sensory evaluation using static and moving two-point discrimination is essential; a healthy fingertip typically registers 3-5 mm of two-point discrimination.
Imaging is a mandatory component of the preoperative workup. True orthogonal plain radiographs (posteroanterior, lateral, and oblique views) of the affected digit are required to assess for occult fractures of the distal phalanx, retained radiopaque foreign bodies, and the exact level of osseous amputation. If a nail bed laceration is suspected, particularly in the setting of a subungual hematoma encompassing more than 50% of the visible nail plate, the patient must be counseled on the necessity of nail plate removal and microscopic repair of the sterile or germinal matrix.

Anesthesia and Patient Setup
"Alright team, let's proceed with patient positioning and anesthesia." The patient is positioned strictly supine on the operating table. A standard, rigid hand table is secured to the operative bed, ensuring it is perfectly level with the patient's torso to prevent traction neurapraxia of the brachial plexus. The affected upper extremity is extended onto the hand table, resting on a well-padded surface. The surgeon and the surgical assistant should be seated opposite each other, with the microscope or loupe magnification readily accessible.
Anesthesia is typically achieved via a regional block. A meticulously performed digital block using a 50/50 mixture of 1% Lidocaine and 0.5% Bupivacaine (without epinephrine if using a tourniquet, though WALANT principles are increasingly utilized) provides excellent, prolonged anesthesia. We routinely employ a digital tourniquet—either a sterile glove finger rolled proximally or a dedicated commercial digital tourniquet—placed at the base of the proximal phalanx. "Nurse, please note the exact time of tourniquet inflation. We must maintain a bloodless field to safely identify the arborizing neurovascular structures during flap elevation. We will limit tourniquet time to a maximum of 60 minutes before allowing a period of reperfusion."

Prior to any definitive incision, the wound undergoes rigorous irrigation and sharp debridement. We utilize copious amounts of sterile normal saline, delivered via a low-pressure system, to mechanically clear debris. Using a No. 15 scalpel and fine tenotomy scissors, all non-viable, crushed, or contaminated soft tissue is sharply excised until healthy, punctate bleeding is observed from the wound margins upon temporary tourniquet release. If the germinal matrix is irreparably damaged, it must be completely ablated to prevent the formation of painful, ectopic nail horns.
Step-by-Step Surgical Approach and Fixation Technique
The intraoperative execution of soft tissue coverage requires a mastery of tissue handling. We will detail the two most fundamental techniques in the reconstructive ladder for fingertip amputations: the Full-Thickness Skin Graft (FTSG) and the V-Y Advancement Flap.
Technique 1: The Full-Thickness Skin Graft (FTSG)
For defects possessing a robust, well-vascularized bed devoid of exposed, denuded bone or tendon, a full-thickness skin graft is the gold standard. FTSGs are vastly superior to split-thickness grafts in the hand, as they undergo significantly less primary and secondary contracture, provide superior durability against shear forces, and offer enhanced sensory recovery over time due to the inclusion of a greater density of neural elements within the dermis.

1. Defect Templating and Donor Site Selection:
"Fellows, observe the debrided defect. The bone is adequately covered by a thin layer of healthy periosteum and pulp tissue. We will proceed with an FTSG. First, we must create a precise template." We utilize the sterile foil from a suture packet, pressing it firmly against the defect to capture a blood imprint, and then trim it to the exact dimensions of the wound. For fingertip reconstruction, the hypothenar eminence is the premier donor site. It provides glabrous skin that perfectly matches the color, texture, and thickness of the palmar fingertip, while leaving a well-hidden, functionally inconsequential scar.

2. Graft Harvest and Meticulous Defatting:
"We transfer our foil template to the ulnar aspect of the hypothenar eminence, ensuring the long axis of the ellipse aligns with the resting skin tension lines." Using a No. 15 blade, the skin is incised down to the subcutaneous fat. The graft is then sharply elevated.

The most critical step in this procedure is the defatting of the graft. "Fellows, a graft will only survive through the process of plasmatic imbibition followed by inosculation. Any residual adipose tissue acts as an impenetrable barrier to these processes." The graft is inverted over the surgeon's index finger. Using curved iris scissors, the subcutaneous fat is meticulously trimmed away until the undersurface of the dermis presents a stark, pearly-white appearance, completely devoid of yellow adipose lobules.

Observe the harvested graft ex vivo; the complete absence of fat is visually confirmed before proceeding to inset.

3. Insetting and Bolster Application:
The defatted graft is transferred to the recipient bed. "We will inset the graft using 6-0 chromic gut sutures in a simple interrupted fashion. It is imperative to achieve exact dermal-to-dermal approximation without placing the graft under excessive tension."

To ensure intimate contact between the graft and the recipient bed and to prevent shearing forces, a tie-over bolster dressing is mandatory. We leave four to six of our inset sutures long. A layer of non-adherent Xeroform gauze is placed directly over the graft, followed by a bolus of mineral oil-soaked sterile cotton or a specialized foam sponge. The long sutures are then tied over this bolus, creating a compressive, immobile environment that is essential for graft take. The hypothenar donor site is undermined slightly and closed primarily with 4-0 nylon sutures.

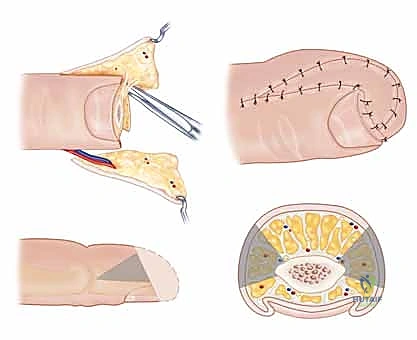
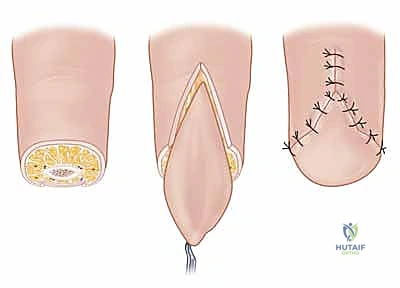
Technique 2: The V-Y Advancement Flap (Atasoy Flap)
When the amputation geometry is transverse or dorsal oblique, and there is exposed distal phalanx lacking periosteal coverage, a skin graft will inevitably fail. In these scenarios, the V-Y advancement flap, originally popularized by Atasoy, provides durable, sensate, autologous tissue coverage.

1. Flap Design and Incision:
"We must design the flap with geometric precision. The width of the 'V' at the distal amputation edge must exactly match the width of the defect. The apex of the 'V' should extend proximally to the distal interphalangeal (DIP) joint crease, but no further, to avoid compromising the flexion crease." The lines are drawn with a sterile marker. Using a No. 15 blade, the skin is incised along the 'V' markings. Crucially, the incision must only penetrate the epidermis and dermis. Deepening the incision into the subcutaneous tissue at the margins will inevitably sever the arborizing neurovascular supply to the flap, resulting in catastrophic flap necrosis.

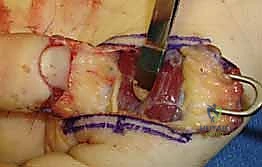
2. Mobilization and Septal Release:
This is the most technically demanding portion of the procedure. "The flap is currently tethered to the underlying distal phalanx by the dense fibrous septa of the pulp. We must release these septa to allow distal advancement, while meticulously preserving the neurovascular bundles that enter the flap volarly." Using fine tenotomy scissors or a No. 15 blade, the surgeon works beneath the flap, carefully dividing the fibrous septa right at their insertion onto the periosteum of the distal phalanx.

Gentle distal traction is applied to the flap with skin hooks. As the septa are released, the flap will mobilize distally. The surgeon must constantly visualize the neurovascular bundles, ensuring they are stretching but not tearing. The flap must advance sufficiently to cover the exposed bone without any tension. If tension exists, further proximal septal release is required.

3. Insetting and Closure:
Once adequate, tension-free advancement is achieved, the flap is inset. "We first secure the distal edge of the flap to the nail bed or the dorsal skin margin using 5-0 or 6-0 absorbable sutures."
Following the distal inset, the proximal donor defect, which was originally a 'V', is now closed primarily in a straight line, converting the overall incision into a 'Y'. This proximal closure effectively pushes the flap distally, alleviating tension on the critical distal anastomosis.

The tourniquet is deflated, and the flap is observed for capillary refill. A healthy pink hue should return within seconds. The digit is then dressed with a non-adherent layer, bulky gauze, and placed in a protective splint, ensuring the PIP joint remains free to prevent proximal stiffness.

Alternative Coverage: Cross-Finger and Regional Flaps
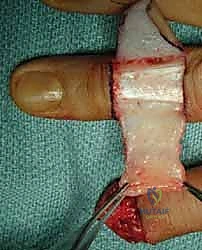
For extensive volar oblique defects where local tissue is insufficient, regional flaps must be employed. The Cross-Finger Flap utilizes skin and subcutaneous tissue from the dorsum of the adjacent, uninjured finger.

This flap is elevated above the paratenon of the extensor mechanism of the donor digit and hinged laterally to cover the volar defect of the injured finger.

The donor site is subsequently covered with a full-thickness skin graft. This technique requires the digits to be sutured together (syndactylized) for 14 to 21 days before the pedicle is divided, making it contraindicated in patients prone to joint stiffness.

Complications, Incidence Rates, and Salvage Management
Despite flawless surgical execution, fingertip reconstructions are fraught with potential complications. The biological interface between reconstructed skin, a rigid nail plate, and the highly mobile distal phalanx creates an environment where minor biomechanical imbalances lead to significant functional morbidity. The surgeon must be acutely aware of these pitfalls and possess the clinical acumen to manage them promptly.

The most devastating acute complication is flap necrosis, which typically presents within the first 48 to 72 hours postoperatively. This is almost universally the result of technical error: either excessive tension on the distal inset, failure to adequately release the restraining fibrous septa, or iatrogenic transection of the arborizing neurovascular bundles during dissection. If venous congestion is noted early, releasing a few sutures may salvage the flap. However, established arterial necrosis demands immediate return to the operating room for debridement and conversion to a higher-order reconstructive option, such as a cross-finger flap or even terminal revision amputation.

Long-term complications are frequent and can be debilitating. Cold intolerance is nearly ubiquitous, reported in up to 70% of patients following significant fingertip trauma,
Clinical & Radiographic Imaging Archive