Mastering Open Scapholunate Ligament Repair and Dorsal Capsulodesis Augmentation: An Intraoperative Guide

Key Takeaway
This masterclass guides fellows through open scapholunate ligament repair and augmentation. We detail patient positioning, comprehensive wrist anatomy, precise surgical steps from incision to fixation, and critical pearls for managing SLIL instability. Learn intraoperative decision-making, meticulous dissection, hardware application, and essential postoperative care to ensure optimal patient outcomes for acute and reducible chronic tears.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues, to this definitive exploration of one of the most challenging and critical procedures in hand and wrist surgery. Today, we are addressing a pathology that represents one of the most common and potentially debilitating forms of carpal instability: the scapholunate interosseous ligament (SLIL) injury. Left unrecognized or inadequately treated, an SLIL disruption initiates a predictable, unrelenting, and progressive pattern of radiocarpal and midcarpal degenerative joint disease universally known as Scapholunate Advanced Collapse, or the SLAC wrist. Our primary surgical objective is to meticulously repair the primary stabilizing soft tissues and augment the construct to restore native carpal kinematics, thereby halting or preventing this degenerative cascade.
Scapholunate instability is not a singular, monolithic entity; rather, it exists on a complex clinico-radiographic spectrum. This spectrum ranges from occult dynamic instability—where the patient is symptomatic but radiographic changes are only provoked and visualized under active stress—to static instability, where characteristic anatomical derangements are grossly visible on routine, non-weight-bearing plain radiographs. The natural history of a complete SLIL rupture involves the uncoupling of the scaphoid and the lunate. Bereft of its primary ligamentous tether, the scaphoid naturally falls into a flexed and pronated posture under the axial load of the radius and trapezium. Conversely, the lunate, now dictated solely by its remaining triquetral attachments via the lunotriquetral interosseous ligament, extends. This divergent kinematic behavior creates the classic Dorsal Intercalated Segmental Instability (DISI) deformity.
The timing of surgical intervention is a critical determinant of operative success. We strictly differentiate between acute tears, typically defined as those presenting less than six weeks from the initial traumatic event, and chronic tears. Acute and subacute injuries (up to 12 weeks in some robust patients) are frequently amenable to primary ligamentous repair, provided the tissue quality remains viable. Chronic injuries, however, present a formidable challenge; the ligamentous remnants often resorb or undergo severe fibrotic degeneration, necessitating complex tendon reconstructions, regional capsulodesis, or salvage procedures. Crucially, prior to committing to a soft-tissue repair, the surgeon must definitively assess for fixed versus reducible deformities. Only passively reducible deformities, where the articular cartilage remains pristine, are suitable for the open repair and dorsal capsulodesis augmentation we are detailing in this chapter.
Detailed Surgical Anatomy and Biomechanics
The Scapholunate Interosseous Ligament Complex
A profound understanding of the micro-anatomy and biomechanics of the carpus is non-negotiable for the reconstructive wrist surgeon. The SLIL is not a simple, homogenous band of tissue, but rather a complex, C-shaped, tripartite structure comprising dorsal, proximal (membranous), and volar regions. The dorsal region is the thickest, most robust, and biomechanically critical component. Composed of stout, transversely oriented collagen fibers, it is the primary restraint to both volar-dorsal translation and diastasis between the scaphoid and lunate. Studies have demonstrated that the dorsal SLIL possesses a yield strength of approximately 260 to 300 Newtons.
The proximal or membranous region is predominantly fibrocartilaginous. It offers negligible mechanical strength and functions primarily as an articular seal, separating the radiocarpal joint from the midcarpal joint. The volar region is thinner than the dorsal component but plays a vital role in resisting rotational forces. A true, clinically significant DISI deformity typically requires not only the complete disruption of all three components of the SLIL but also the attenuation or tearing of secondary extrinsic stabilizers.
Secondary Extrinsic Stabilizers
The carpus relies heavily on a sophisticated network of secondary extrinsic ligaments. Dorsally, the dorsal intercarpal (DIC) ligament and the dorsal radiocarpal (DRC) ligament form a critical V-shaped stabilizing complex. The DIC originates on the triquetrum and courses radially to insert on the lunate, the dorsal groove of the scaphoid, and the trapezium. The DRC originates on the dorsal rim of the radius and inserts on the lunate and triquetrum. Together, they act as a secondary restraint against scaphoid flexion and lunate extension. In high-energy trauma, the DIC can avulse from its scaphoid attachment, exacerbating the instability.
Volarly, the radioscaphocapitate (RSC) ligament acts as a crucial fulcrum around which the scaphoid rotates. The scaphotrapezial-trapezoid (STT) ligament complex also provides distal stabilization. When the SLIL is compromised, these secondary stabilizers are subjected to abnormal, repetitive stress, eventually stretching out and allowing the classic static DISI deformity to manifest. Our surgical repair must respect and, when possible, recruit these secondary stabilizers—particularly the dorsal capsule and DIC—to augment the primary SLIL repair.
Exhaustive Indications and Contraindications
Patient selection is paramount in scapholunate reconstruction. The ideal candidate for an open primary repair with dorsal capsulodesis is a patient with a symptomatic, acute or subacute (less than 6 to 12 weeks old) complete SLIL rupture, demonstrating a reducible DISI deformity, and possessing no radiographic or arthroscopic evidence of chondral wear.
| Parameter | Indications for Open Repair & Capsulodesis | Contraindications |
|---|---|---|
| Chronicity | Acute (< 6 weeks) or Subacute (6-12 weeks) | Chronic (> 12 weeks) with poor tissue quality |
| Instability Grade | Geissler Grade III or IV (Complete disruption) | Geissler Grade I or II (Consider arthroscopic debridement/pinning) |
| Deformity Reducibility | Passively reducible scaphoid and lunate | Fixed DISI deformity |
| Joint Cartilage | Pristine radiocarpal and midcarpal cartilage | Established SLAC arthritis (Stage I-III) |
| Tissue Quality | Adequate SLIL stump for suture purchase | Completely resorbed or severely friable SLIL |
| Patient Factors | High-demand patient, compliant with rehab | Non-compliant, severe osteopenia, active infection |
Pre-Operative Planning, Diagnostic Modalities, and Patient Positioning
Diagnostic Insights and Imaging Modalities
The clinical evaluation of a patient with suspected SLIL instability begins with a meticulous history. Patients typically present following a fall on an outstretched hand (FOOSH) with the wrist in extension, ulnar deviation, and intercarpal supination. They will report acute dorsal radial wrist pain, grip weakness, and a subjective sense of giving way. The Watson scaphoid shift test is pathognomonic; pressure applied to the volar tuberosity of the scaphoid during ulnar-to-radial deviation will elicit a painful dorsal subluxation, followed by a palpable "clunk" as the scaphoid reduces when pressure is released.
While advanced imaging like MRI, CT arthrography, and high-resolution ultrasound offer valuable clues, their diagnostic accuracy for SLIL tears can be surprisingly variable. MRI sensitivity for complete tears ranges from 60% to 80%, but it is notoriously poor at assessing the integrity of the critical dorsal component. CT arthrography is highly sensitive for detecting tears via contrast leakage but cannot reliably determine the biomechanical competence of the ligament. A negative result on these non-invasive studies absolutely does not rule out a surgically actionable ligamentous injury.
Plain radiography remains the cornerstone of initial evaluation. We scrutinize the PA, lateral, and clenched-fist views for five characteristic findings:
* Terry Thomas sign: A scapholunate interval exceeding 3 mm on a PA radiograph.
* Cortical ring sign: Hyperdensity of the scaphoid cortex on the PA view, representing the flexed scaphoid viewed end-on.
* Angular changes: On the lateral view, a scapholunate angle >60 degrees, a capitolunate angle >15 degrees, or a radiolunate angle >10 degrees strongly suggests a DISI deformity.
* Quadrangular lunate: The lunate appears wedge-shaped or rectangular on the PA view as it rolls into extension.
* Disruption of Gilula’s lines: The three smooth, concentric radiographic arcs outlining the proximal and distal carpal rows are abruptly stepped or broken.
The Gold Standard: Diagnostic Arthroscopy
Because of the limitations of advanced imaging, diagnostic wrist arthroscopy remains the undisputed gold standard for definitively diagnosing SLIL tears, assessing their precise severity, and confirming the absence of early chondral damage. We utilize the standard 3-4 portal for viewing with a 2.7-mm or 1.9-mm arthroscope, establishing outflow via the 6U portal, and using the 4-5 or 1-2 portal for instrumentation.
A 1-mm probe is utilized to test the integrity of the SLIL from both the radiocarpal and midcarpal spaces. A probe that can be passed fully through the scapholunate interval and rotated 360 degrees defines a Geissler Grade III lesion. A "drive-through" sign, where the arthroscope itself can easily pass from the midcarpal space into the radiocarpal space through the SL interval, signifies a Geissler Grade IV lesion (complete disruption). If the joint is pristine and the tear is robust, we proceed immediately to the open repair.
Patient Positioning and Operating Room Setup
Meticulous preoperative setup is the foundation of a smooth surgical procedure.
1. Anesthesia: General anesthesia or a robust regional axillary block is utilized, tailored to the patient's physiological status.
2. Positioning: The patient is positioned supine. A specialized, radiolucent hand table is securely attached to the main operating table. The table should be positioned to face the corner opposite the anesthesia team, maximizing ergonomic space.
3. Tourniquet: A well-padded upper arm pneumatic tourniquet is applied and inflated to 250 mmHg following strict exsanguination.
4. Fluoroscopy: The C-arm fluoroscope is brought in from the opposite side, perpendicular to the patient's wrist. The C-arm should be draped sterilely and kept parallel to the floor, allowing the surgeon to slide it in and out seamlessly for AP and lateral views without disturbing the sterile field.
5. Traction: The operative arm is prepped and draped. The wrist is suspended using a sterile wrist traction tower with 10 to 15 pounds of distraction. This opens the radiocarpal and midcarpal spaces, drastically improving visualization during the initial arthroscopic phase and facilitating subsequent open reduction maneuvers.
Step-by-Step Surgical Approach and Fixation Technique
Incision, Superficial Dissection, and Nerve Protection
Following the arthroscopic confirmation of a repairable Geissler III or IV tear, the wrist is taken out of traction. We initiate a 5 to 6-cm longitudinal dorsal skin incision centered just ulnar to Lister's tubercle. This trajectory provides optimal, direct access to the third extensor compartment and the underlying dorsal carpal capsule.
Subcutaneous dissection must be performed with exacting care. Using blunt-tipped scissors, elevate full-thickness skin flaps radially and ulnarly. The surgeon must remain hyper-vigilant regarding the superficial radial nerve (SRN) branches on the radial aspect and the dorsal cutaneous branch of the ulnar nerve (DCBUN) on the ulnar aspect. The SRN is particularly vulnerable here; aggressive retraction or sharp dissection can lead to devastating, recalcitrant neuromas. Retract these neural structures gently within the full-thickness flaps.
We identify the extensor retinaculum and incise it longitudinally directly over the third extensor compartment. The extensor pollicis longus (EPL) tendon is identified, mobilized, and transposed radially into the subcutaneous tissues. This transposition removes the EPL from the surgical field, preventing iatrogenic injury and allowing unimpeded access to the dorsal capsule.
Dorsal Capsulotomy and Joint Exposure
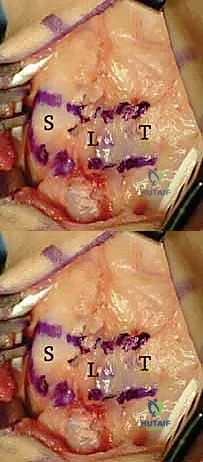
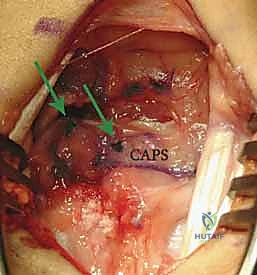
The exposure of the dorsal capsule reveals the transverse fibers of the dorsal radiocarpal (DRC) and dorsal intercarpal (DIC) ligaments. To expose the scapholunate interval while preserving tissue for a subsequent capsulodesis, we design an ulnar-based, ligament-sparing capsular flap. The incision begins radially along the dorsal rim of the radius, extends distally along the axis of the scaphoid, and then turns ulnarly, running parallel to the distal margin of the DIC ligament.
Here, the exposure highlights the ulnar-based dorsal capsular flap. The DIC parallels the transverse limb of the flap. The scaphoid, lunate, and triquetrum are clearly visualized beneath the reflected tissue.
This ulnar-based flap is carefully elevated off the underlying carpus, preserving its vascularity and structural integrity. It is imperative that this flap is at least 1 cm wide and of sufficient length to reach the distal pole of the scaphoid later in the procedure.
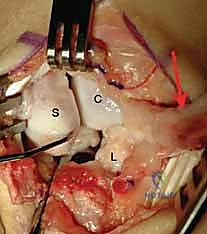
Once the capsule is reflected, the devastating pathology of the SLIL disruption is immediately apparent. We systematically inspect the radiocarpal and midcarpal articular surfaces to confirm the absence of advanced chondromalacia.

Observe the classic DISI deformity. The scaphoid is severely flexed, and the lunate is extended. The complete disruption of the SLIL is evident, leaving a yawning gap between the two carpal bones.
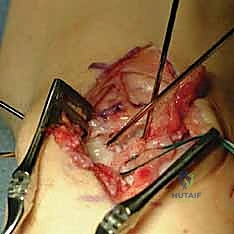
We meticulously debride the interposed hematoma, synovitis, and any frayed, non-viable ligamentous edges using a small rongeur and a motorized shaver. Typically, the dorsal SLIL avulses from its scaphoid footprint, leaving a robust stump attached to the lunate.
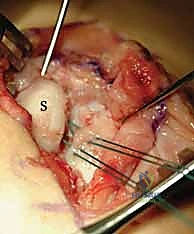
This high-magnification view clearly demonstrates the scaphoid on the left and the viable SLIL stump remaining attached to the lunate on the right, grasped securely by forceps.
Joystick Placement and Anatomic Reduction
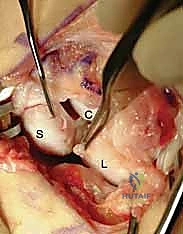
To achieve an anatomic reduction of the DISI deformity, we must independently control the scaphoid and the lunate. We utilize two 0.062-inch smooth Kirschner wires (K-wires) as "joysticks."
The first K-wire is driven into the dorsal-distal pole of the scaphoid, directed proximally and volarly. Because the scaphoid is flexed, the surgeon will initially be looking directly at its dorsal articular surface. The second K-wire is driven into the dorsal aspect of the lunate, directed distally and volarly.
The 0.062-inch K-wire joysticks are securely placed into the scaphoid and lunate. Notice their divergent initial angles, representing the uncoupled state of the carpal bones.
Using these joysticks, we perform the reduction maneuver. The scaphoid joystick is pulled proximally and dorsally to extend and supinate the scaphoid. Simultaneously, the lunate joystick is pushed volarly to flex the lunate, correcting its extended posture. The two joysticks are then brought together, closing the scapholunate diastasis and perfectly realigning the articular congruency.

The reduction maneuver is complete. The joysticks have been manipulated to extend the scaphoid and flex the lunate, closing the gap and restoring the anatomic scapholunate relationship.
Primary Ligament Repair and Suture Anchor Fixation
With the joint anatomically reduced and held securely by an assistant (or temporarily pinned with a 0.045-inch K-wire across the SL joint), we proceed to the primary ligament repair. The scaphoid footprint is lightly decorticated with a small burr or curette to expose bleeding cancellous bone, optimizing the biological environment for ligament-to-bone healing.
Depending on the size of the scaphoid, one or two titanium or bio-composite micro-suture anchors (typically 1.5 mm to 2.0 mm in diameter) are inserted into the decorticated dorsal-proximal footprint of the scaphoid.
Micro-suture anchors are placed into the anatomic footprint on the scaphoid. The high-tensile strength sutures are then passed through the robust SLIL stump on the lunate using a horizontal mattress configuration.
The sutures from the anchors are passed through the lunate SLIL stump using a small, curved needle. We prefer a horizontal mattress configuration to maximize tissue capture and prevent suture pull-through. The sutures are then tied securely, drawing the ligament stump tightly against the bleeding scaphoid footprint.
Dorsal Capsulodesis Augmentation
While primary repair is crucial, the native SLIL is inherently slow to heal, and the repair is subjected to immense shear forces. Therefore, we augment the repair with a dorsal capsulodesis, utilizing the previously elevated ulnar-based capsular flap (a modification of the classic Blatt capsulodesis) or a slip of the DIC ligament.
The ulnar-based dorsal capsular flap is prepared for augmentation. It will act as a secondary dorsal tether, reinforcing the primary SLIL repair.
The distal end of our capsular flap is advanced distally and radially across the repaired SL joint. A trough is created on the dorsal aspect of the distal scaphoid pole. Another suture anchor is placed into this trough.
The capsular flap is advanced and secured to the distal scaphoid using an additional suture anchor. This effectively tethers the scaphoid, preventing it from falling back into a flexed posture.
By securing the capsular flap to the distal scaphoid, we create a stout dorsal check-rein. This capsulodesis neutralizes the inherent flexion forces acting on the scaphoid, offloading the primary SLIL repair during the critical early phases of biological healing.
Transfixion Pinning and Closure
To protect the repair and the capsulodesis from the massive forces generated across the wrist, the carpus must be rigidly immobilized internally. We utilize multiple 0.045-inch or 0.062-inch K-wires for transfixion.

Transfixion pinning is executed. K-wires are driven from the radial aspect of the scaphoid into the lunate, and from the scaphoid into the capitate, neutralizing all rotational and translational forces.
Typically, two wires are driven from the scaphoid into the lunate to protect the SL interval directly. An additional wire is driven from the scaphoid into the capitate to neutralize the midcarpal joint and prevent scaphoid flexion. These wires are verified under multi-planar fluoroscopy to ensure they do not penetrate the radiocarpal articular surface. The wires are cut beneath the skin to minimize pin tract infection risk.
The final construct. The SLIL is repaired, the capsulodesis is secured, and the transfixion wires hold the carpus in perfect anatomic alignment. The EPL is left transposed in the subcutaneous tissue, and the extensor retinaculum is loosely repaired.
The wound is irrigated copiously. The extensor retinaculum is repaired over the remaining extensor compartments, ensuring the EPL remains superficial to the retinaculum to prevent tethering. The skin is closed with non-absorbable sutures, and a bulky, sterile, short-arm thumb-spica splint is applied.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, open SLIL repair with capsulodesis carries a recognized complication profile. The surgeon must be prepared to manage these effectively and counsel the patient preoperatively regarding salvage options.
| Complication | Estimated Incidence | Management and Salvage Strategy |
|---|---|---|
| Post-operative Stiffness | 40% - 60% | The most common complication. Requires aggressive, phased hand therapy. Loss of 15-20 degrees of terminal flexion/extension is expected and considered an acceptable trade-off for stability. |
| Pin Tract Infection | 5% - 10% | Minimized by burying wires beneath the skin. Treated with oral antibiotics and early pin removal if the infection tracks deep. |
| Hardware Failure / Anchor Pull-out | < 5% | Often secondary to non-compliance or osteopenia. May require revision surgery or conversion to a salvage procedure if instability recurs. |
| Recurrent Instability / Stretch-out | 15% - 25% | The capsulodesis may attenuate over time. If symptomatic, requires salvage (e.g., partial wrist fusion). |
| Progression to SLAC Wrist | 10% - 30% (Long-term) | If the repair fails or articular cartilage was compromised, osteoarthritis will progress. Salvage options include Proximal Row Carpectomy (PRC) or Scaphoid Excision and Four-Corner Fusion (4CF). |
| Superficial Radial Nerve Neurapraxia | 2% - 5% | Usually transient due to retraction. Resolves with time and desensitization therapy. Persistent neuroma requires surgical excision and burying of the nerve stump. |
Phased Post-Operative Rehabilitation Protocols
The rehabilitation following an open SLIL repair is as critical as the surgery itself. The protocol must balance the need for rigid immobilization to allow ligamentous healing with the necessity of early motion to prevent debilitating arthrofibrosis.
Phase 1: Maximum Protection (Weeks 0 to 8)
The patient remains in a rigid cast or custom thermoplastic thumb-spica orthosis. Absolute immobilization of the wrist and thumb is maintained. The patient is instructed to perform aggressive active range of motion exercises for the fingers, elbow, and shoulder to prevent proximal and distal stiffness and to promote edema resolution. Heavy lifting and gripping are strictly prohibited.
Phase 2: Hardware Removal and Early Motion (Weeks 8 to 12)
At the 8-week mark, radiographs are obtained to confirm maintenance of reduction. The buried K-wires are removed under local anesthesia in the clinic or a minor procedure room. The patient is transitioned to a removable custom orthosis. Supervised therapy begins, focusing on active and active-assisted range of motion. Crucially, therapy should initially focus on the "dart thrower's motion" (radial extension to ulnar flexion), as biomechanical studies have shown this plane of motion minimizes stress across the healing scapholunate interval.
Phase 3: Strengthening and Return to Function (Weeks 12 and Beyond)
Passive stretching and progressive strengthening exercises are initiated. The orthosis is weaned during the day but may be worn at night or during high-risk activities. Patients are counseled that maximal medical improvement may take up to 12 months. Return to heavy manual labor or contact sports is typically restricted until 5 to 6 months post-operatively, often requiring the use of a protective functional brace.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for scapholunate instability is deeply rooted in several landmark publications. The understanding of carpal kinematics was revolutionized by the work of Garcia-Elias et al., who developed a comprehensive treatment-oriented classification system based on the integrity of the secondary stabilizers, the reducibility of the deformity, and the status of the articular cartilage. Their algorithms remain the foundation of modern clinical decision-making.
The concept of dorsal capsulodesis to augment soft-tissue repairs was popularized by Blatt in 1987. Blatt utilized a proximally based flap of the dorsal capsule tethered to the distal scaphoid to prevent scaphoid flexion. While effective in stabilizing the scaphoid, the classic Blatt procedure was often associated with significant loss of wrist flexion. Consequently, modern techniques, such as the modified ulnar-based capsulodesis detailed in this chapter, or the DIC-based capsulodesis described by Slater et al., have been developed to provide equivalent biomechanical stability while better preserving the radiocarpal arc of motion.
Current clinical guidelines strongly support the use of diagnostic arthroscopy to stage the injury accurately. For acute and subacute, reducible, non-arthritic complete SLIL tears, the consensus strongly favors anatomic open primary repair augmented with a dorsal capsulodesis and rigid temporary internal fixation, as this approach offers the highest probability of restoring native carpal kinematics and preventing the devastating progression to SLAC wrist arthropathy.
