Mastering Radial Styloidectomy: An Open Surgical Approach for Radiocarpal Arthritis

Key Takeaway
This masterclass guides fellows through open radial styloidectomy, a precise technique for radiocarpal arthritis. We'll cover essential anatomy, meticulous patient positioning, and granular intraoperative steps, emphasizing nerve protection and optimal bone resection. Learn to manage potential pitfalls and ensure successful patient outcomes with detailed postoperative rehabilitation protocols.
Comprehensive Introduction and Patho-Epidemiology
The open radial styloidectomy remains a cornerstone in the armamentarium of the hand and wrist surgeon. While often conceptualized as a straightforward osseous resection, the procedure demands a profound understanding of carpal kinematics, precise patient selection, and meticulous surgical execution. Historically utilized as a standalone intervention for localized radiocarpal arthrosis, its contemporary application is frequently as a critical adjunct to broader reconstructive or salvage operations. The fundamental objective is the elimination of painful osseous impingement between the radial styloid and the scaphoid, thereby mitigating localized synovitis, restoring functional grip strength, and optimizing the radiocarpal articular interface. When executed with precision, it offers a highly reliable method for addressing focal mechanical nociception in the degenerative wrist.
The pathogenesis of radioscaphoid arthritis is inextricably linked to alterations in carpal biomechanics. In the normal wrist, load transmission occurs predictably across the radiocarpal joint, with the scaphoid facet bearing a significant proportion of the axial force. However, in the setting of ligamentous incompetence—most notably scapholunate (SL) dissociation—the scaphoid loses its proximal tether to the lunate. This kinematic derangement allows the scaphoid to adopt a pathologically flexed and pronated posture, driven by the unopposed pull of the radiocapitate ligaments and the inherent geometry of the scaphoid fossa. Consequently, the contact area between the scaphoid and the radial fossa decreases, leading to exponentially increased contact pressures localized to the dorsal lip of the radial styloid and the proximal pole of the scaphoid. This predictable pattern of degeneration is the hallmark of the Scapholunate Advanced Collapse (SLAC) wrist.

Similarly, the Scaphoid Nonunion Advanced Collapse (SNAC) wrist presents a parallel biomechanical catastrophe. In an unstable scaphoid nonunion, the proximal pole typically remains anatomically aligned with the lunate, while the distal pole flexes volarly. This flexed distal fragment creates a focal point of abnormal contact stress against the radial styloid. Prolonged impingement inevitably leads to chondral wear, osteophyte formation, and the progressive arthritic changes characteristic of the SNAC I pattern. Furthermore, iatrogenic alterations to carpal mechanics, such as those following a triscaphe (scaphoid-trapezium-trapezoid or STT) arthrodesis, can tether the scaphoid in a position that no longer congruently matches the radial fossa, inducing secondary radial styloid impingement.
Understanding the epidemiology and natural history of these conditions is paramount for managing patient expectations. Radial styloidectomy, particularly when performed in isolation for early-stage SLAC or SNAC wrists, is fundamentally a palliative and temporizing procedure. It effectively addresses the immediate source of mechanical nociception but does not halt the underlying kinematic instability driving the arthritic cascade. Therefore, it is most judiciously applied in low-demand individuals, elderly patients seeking pain relief without the morbidity of a total wrist fusion, or as an adjunct in high-demand patients undergoing concurrent stabilizing procedures, such as partial carpal fusions, proximal row carpectomies, or advanced ligamentous reconstructions.
Detailed Surgical Anatomy and Biomechanics
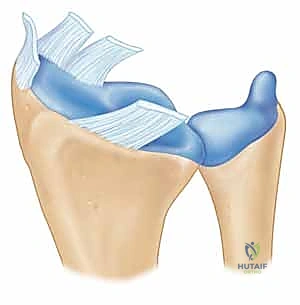
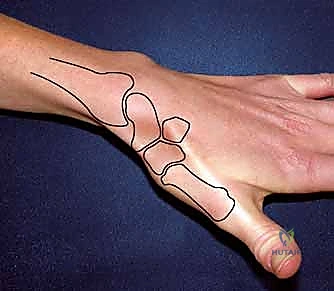
A rigorous command of the osseous and capsuloligamentous anatomy of the radial styloid is the absolute foundation of a safe and effective resection. The radial styloid is the distal-most lateral projection of the radius, exhibiting a gentle volar slope that positions its apex slightly palmar to the midcoronal longitudinal axis of the radial diaphysis. The intra-articular surface of the styloid comprises the lateral aspect of the scaphoid fossa. It is this specific articular geometry that becomes the site of pathologic impingement when the scaphoid assumes a flexed posture. The extra-articular topography of the styloid is equally critical, serving as the anatomical footprint for the robust extrinsic ligaments that govern radiocarpal stability.
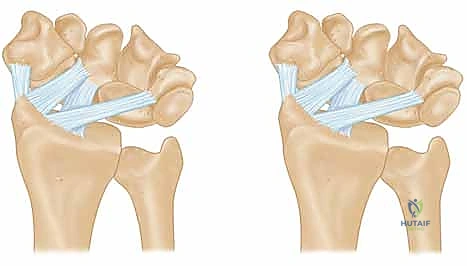
The palmar radiocarpal ligaments are the primary stabilizers against ulnar translation of the carpus. The Radioscaphocapitate (RSC) ligament originates from the palmar cortical margin of the radial styloid, coursing distally and obliquely to support the waist of the scaphoid before inserting on the capitate. Immediately adjacent and ulnar to the RSC is the Long Radiolunate (LRL) ligament. A distinct synovial sulcus separates these two structures, providing a reliable arthroscopic and open landmark. The Radial Collateral Ligament (RCL), a relatively thin and biomechanically less significant structure, originates from the very tip of the radial styloid. While the RCL is universally sacrificed during a styloidectomy, its loss does not precipitate clinically significant instability.

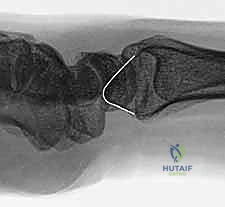
The fundamental surgical peril of radial styloidectomy lies in the inadvertent detachment of the RSC and LRL ligaments. Biomechanical studies by Siegel and Gelberman, alongside volumetric analyses by Nakamura et al., have definitively established the "safe zones" for resection. A transverse resection of more than 3 to 4 millimeters from the tip of the styloid drastically compromises the origin of the RSC ligament. Loss of this ligamentous tether removes the primary restraint to ulnar carpal slide. Therefore, the osteotomy must be meticulously planned as a short, oblique cut—starting distally at the radial margin and exiting proximally within the scaphoid fossa—to decompress the impingement zone while rigorously preserving the volar capsular footprints.
Navigating the surgical approach requires deep respect for the regional neurovascular and tendinous structures. The superficial dissection is fraught with risk to the Radial Sensory Nerve (RSN) and the Lateral Antebrachial Cutaneous Nerve (LABCN). The RSN arborizes extensively in the subcutaneous fat overlying the first dorsal compartment. Iatrogenic injury, traction neuropraxia, or entrapment in scar tissue can result in a debilitating neuroma, often overshadowing the benefits of the osseous resection. Deep to the neural plane, the surgical interval is developed between the first dorsal extensor compartment (containing the abductor pollicis longus and extensor pollicis brevis) and the second dorsal compartment (extensor carpi radialis longus and brevis). Precise retraction of these compartments is essential to expose the dorsal rim of the radius without inducing postoperative tenosynovitis.
Exhaustive Indications and Contraindications
The decision to proceed with a radial styloidectomy hinges on precise clinical and radiographic staging of the radiocarpal joint. The primary, standalone indication is highly localized, symptomatic arthrosis confined strictly to the articulation between the radial styloid and the scaphoid. This is classically observed in SLAC Stage I and SNAC Stage I wrists. In these highly selected scenarios, excising the impinging styloid removes the mechanical block to motion and the source of focal synovitis. Patients typically present with point tenderness directly over the anatomic snuffbox, exacerbated by forced radial deviation and wrist extension—a maneuver that directly compresses the scaphoid against the styloid.

Beyond isolated procedures, radial styloidectomy is heavily utilized as an essential adjunct to broader carpal reconstructions. When performing a scaphoid excision and four-corner arthrodesis for advanced SLAC/SNAC wrists, a concomitant styloidectomy is routinely performed to prevent future impingement of the trapezium or the fused carpal mass against the radial styloid, particularly during radial deviation. Similarly, following a Proximal Row Carpectomy (PRC), the capitate translates proximally to articulate with the lunate fossa. In some morphotypes, this proximal migration allows the trapezium to impinge on the radial styloid; a prophylactic styloidectomy mitigates this risk. It is also utilized in Kienböck's disease, occasionally combined with joint leveling procedures, to alter load distribution across the radiocarpal joint.
Contraindications must be rigorously respected to avoid catastrophic destabilization of the wrist. The absolute contraindication to radial styloidectomy is the presence of pre-existing ulnar translation of the carpus. If the radiocarpal ligaments are already attenuated or incompetent, resecting the bony buttress of the styloid will precipitate rapid, irreversible ulnar subluxation of the entire carpal mass. Furthermore, styloidectomy is contraindicated in SLAC or SNAC Stage II and III wrists if intended as a standalone procedure; addressing only the styloid when degenerative changes have extended to the entire scaphoid fossa or the midcarpal joint will yield negligible clinical improvement and may accelerate global joint deterioration.
Clinical Decision Matrix
| Parameter | Indications for Radial Styloidectomy | Contraindications / Alternative Required |
|---|---|---|
| Pathology Stage | SLAC Stage I, SNAC Stage I | SLAC/SNAC Stage II or III (as standalone) |
| Adjunctive Use | Post-STT Fusion, Proximal Row Carpectomy, 4-Corner Fusion | N/A |
| Ligament Status | Intact RSC and LRL ligaments | Pre-existing ulnar carpal translation |
| Joint Involvement | Arthrosis strictly isolated to the styloid-scaphoid articulation | Diffuse radiocarpal or midcarpal arthrosis |
| Systemic Disease | Post-traumatic or localized degenerative osteoarthritis | Inflammatory arthropathies (e.g., severe Rheumatoid Arthritis) with diffuse capsular laxity |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning begins with high-quality, standardized radiographic imaging. A zero-rotation posteroanterior (PA) view, a true lateral view, and specific scaphoid views are mandatory to assess the extent of joint space narrowing, subchondral sclerosis, and osteophyte formation. The PA radiograph is critically evaluated for any evidence of ulnar variance or pre-existing ulnar translation of the carpus by assessing the radiolunate angle and the Gilula lines. Advanced imaging, specifically a high-resolution non-contrast CT scan, is highly recommended. CT provides a three-dimensional map of the arthrosis, allowing the surgeon to precisely delineate whether the degenerative changes are truly confined to the styloid tip or if they extend deeper into the scaphoid fossa.
Digital templating is a crucial step in the pre-operative workflow. Utilizing the PA radiograph, the surgeon must calculate the exact angle and depth of the proposed osteotomy. The goal is to draw a resection line that initiates at the lateral cortex of the radius, approximately 3 to 4 millimeters proximal to the styloid tip, and angles obliquely to exit at the junction of the scaphoid fossa and the styloid articular surface. This templated line serves as a visual guide to ensure adequate decompression of the impinging bone while strictly preserving the palmar cortical origin of the radioscaphocapitate ligament. Over-resection on the template should prompt a re-evaluation of the surgical strategy.

Anesthetic management typically involves a regional brachial plexus block (supraclavicular or axillary), which provides excellent intra-operative anesthesia and superior postoperative pain control. General anesthesia is reserved for patient preference or specific medical contraindications to regional blockade. A well-padded pneumatic tourniquet is applied to the proximal arm. Exsanguination with an Esmarch bandage and tourniquet inflation (typically 250 mmHg) are essential to provide a bloodless surgical field, which is critical for identifying the delicate branches of the superficial radial nerve.
The patient is positioned supine on the operating table with the operative extremity extended onto a radiolucent hand table. The arm is prepped and draped in a standard sterile fashion, allowing for full mobility of the elbow, wrist, and digits. The wrist is typically positioned in slight ulnar deviation and neutral flexion to place the radial styloid in prominence and draw the scaphoid away from the proposed osteotomy site. Intra-operative fluoroscopy must be readily available and positioned to allow for seamless AP and lateral imaging without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
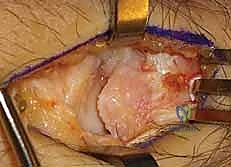
The surgical approach begins with a 4 to 5-centimeter longitudinal or slightly curvilinear dorsoradial incision, centered over the first dorsal extensor compartment and the palpable tip of the radial styloid. The initial dissection through the subcutaneous tissues must be performed with extreme caution using blunt dissecting scissors or a hemostat. The terminal sensory branches of the Radial Sensory Nerve (RSN) and the Lateral Antebrachial Cutaneous Nerve (LABCN) are highly variable in this region. These nerves must be meticulously identified, mobilized, and protected with vessel loops. Vigorous retraction of these nerves must be avoided to prevent traction neuropraxia.

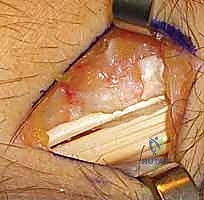
Once the sensory nerves are safely isolated, the deep antebrachial fascia is incised. The surgical interval is developed between the first dorsal compartment (APL and EPB) and the second dorsal compartment (ECRL and ECRB). The first compartment is retracted volarly, and the second compartment is retracted dorsally using small right-angle retractors (e.g., Senn or Ragnell retractors). This exposes the underlying joint capsule and the periosteum of the distal radius. A longitudinal or inverted T-shaped capsulotomy is performed directly over the radial styloid. The capsular flaps are elevated subperiosteally to expose the entire lateral aspect of the styloid and the radioscaphoid articulation.

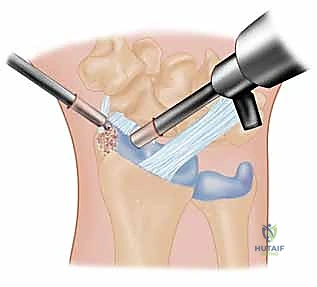
With the joint exposed, the precise location of the impingement is visually confirmed by taking the wrist through a range of motion, particularly radial deviation and extension. The osteotomy is then performed. A micro-sagittal saw or a sharp, thin osteotome is utilized. The cut is initiated on the lateral extra-articular cortex, no more than 3 to 4 millimeters proximal to the tip of the styloid. The blade is directed obliquely, aiming distally and ulnarly to exit precisely at the junction of the styloid and the scaphoid fossa. During the osteotomy, a Freer elevator or a small Hohmann retractor is placed intra-articularly to protect the articular cartilage of the scaphoid from iatrogenic injury.

Following the initial resection, the bony fragment is excised, and the osteotomy site is meticulously smoothed using a rongeur or a high-speed burr to eliminate any sharp cortical edges that could abrade the joint capsule or adjacent tendons. Copious irrigation is employed to remove all bone debris, which could otherwise serve as a nidus for heterotopic ossification or third-body wear. Fluoroscopic evaluation in both AP and lateral planes is mandatory at this juncture to confirm adequate resection and verify that the 3-4mm safe zone has not been violated. The wrist is taken through a full, dynamic range of motion under live fluoroscopy to ensure that impingement has been completely eradicated.


While radial styloidectomy is primarily an excisional procedure, "fixation" in this context refers to the meticulous repair of the capsular structures and, when performed adjunctively, the stabilization of concurrent reconstructive work. The dorsal radiocarpal capsule is carefully reapproximated using interrupted 3-0 or 4-0 absorbable sutures. A robust capsular closure is vital to prevent postoperative synovial fistulas and to restore a degree of secondary dorsal stability. The extensor retinaculum is then repaired, taking care not to overly constrict the first dorsal compartment, which could precipitate de Quervain's tenosynovitis. The skin is closed with a running subcuticular suture, and a bulky, well-padded short-arm volar splint is applied.
Complications, Incidence Rates, and Salvage Management
Despite its conceptual simplicity, radial styloidectomy carries a distinct profile of potential complications that can profoundly impact patient outcomes. The most frequent and arguably most distressing complication is injury to the Radial Sensory Nerve (RSN). The incidence of RSN neuropraxia or neuroma formation ranges from 5% to 15% in the literature, largely dependent on the care taken during the superficial dissection. A symptomatic neuroma can be utterly debilitating, causing intractable neuropathic pain that eclipses the original arthritic symptoms. Management of an established neuroma is notoriously difficult, often requiring surgical exploration, neuroma excision, and nerve end burying into the brachioradialis muscle belly or adjacent bone.

The most catastrophic biomechanical complication is iatrogenic ulnar translation of the carpus. This occurs when the surgeon violates the 3-4mm safe zone, inadvertently detaching the origin of the Radioscaphocapitate (RSC) and Long Radiolunate (LRL) ligaments. Once these critical restraints are lost, the carpus invariably slides ulnarly down the slope of the radial articular surface. This leads to rapid, global radiocarpal and midcarpal arthrosis. Salvage for this disastrous complication is highly complex and typically necessitates a total wrist arthrodesis or a radiolunate arthrodesis to halt the ulnar slide and stabilize the carpus.
Conversely, under-resection of the radial styloid is a common cause of persistent postoperative pain. If the osteotomy does not adequately decompress the impingement zone, particularly during radial deviation, the patient will continue to experience mechanical symptoms. This highlights the absolute necessity of intra-operative fluoroscopic confirmation and dynamic testing. If under-resection is identified postoperatively, a revision styloidectomy may be required. Additionally, Complex Regional Pain Syndrome (CRPS) is a recognized risk following any wrist surgery; early identification and aggressive multimodal management, including sympathetic blocks and intensive hand therapy, are crucial.
Complication Profile and Management Strategies
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| RSN Neuroma / Injury | 5% - 15% | Vigorous retraction, direct laceration | Gabapentinoids, targeted nerve blocks; surgical excision and burying |
| Ulnar Carpal Translation | < 2% | Over-resection (>4mm), RSC/LRL detachment | Total wrist arthrodesis, radiolunate fusion |
| Persistent Impingement | 5% - 10% | Under-resection, inadequate angle of osteotomy | Revision open or arthroscopic styloidectomy |
| De Quervain's Tenosynovitis | 2% - 5% | Over-tightening of extensor retinaculum | Corticosteroid injection, surgical release of 1st dorsal compartment |
| CRPS | 1% - 3% | Idiopathic, prolonged immobilization | Aggressive hand therapy, sympathetic nerve blocks, pain management |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following an open radial styloidectomy is designed to balance the protection of the capsular repair with the early restoration of radiocarpal kinematics. Immediately following surgery, the wrist is immobilized in a bulky, short-arm volar splint with the wrist in neutral extension. This initial phase, lasting approximately 10 to 14 days, is dedicated to acute wound healing, strict edema control, and the prevention of hematoma formation. Patients are instructed to maintain strict elevation of the operative extremity and to perform aggressive active range of motion exercises of the digits, thumb, elbow, and shoulder to prevent stiffness and promote venous return.
At the two-week postoperative mark, the patient returns to the clinic for suture removal and the transition to a custom-molded thermoplastic splint. At this juncture, supervised hand therapy is initiated. The primary focus shifts to restoring wrist mobility, specifically utilizing the "dart-thrower's motion" arc. This oblique plane of motion (from radial extension to ulnar flexion) minimizes stress on the healing dorsal capsule and the scapholunate interval while effectively mobilizing the midcarpal joint. Passive stretching and forceful manipulation are strictly avoided during this early mobilization phase to prevent capsular attenuation and reactive synovitis.
By weeks four to six, the thermoplastic splint is gradually weaned, and patients are encouraged to use the hand for light, activities of daily living (ADLs). Progressive strengthening exercises are introduced, focusing on isometric and subsequent isotonic strengthening of the wrist flexors and extensors. Proprioceptive re-education is also a critical component of this phase, utilizing tools such as the PowerWeb or neuromuscular electrical stimulation (NMES) to optimize dynamic joint stability. Heavy lifting, impact loading, and forced radial deviation are restricted until at least eight to ten weeks postoperatively.
Return to full, unrestricted activity, including heavy manual labor or high-impact sports, is typically permitted between three and four months postoperatively, contingent upon the resolution of pain, the restoration of near-normal grip strength, and radiographic evidence of stable carpal alignment. It is vital to counsel patients that while the mechanical impingement has been addressed, the underlying arthritic process (e.g., SLAC/SNAC) may continue to progress over years or decades. Therefore, long-term follow-up and intermittent radiographic surveillance are recommended to monitor for advancing midcarpal arthrosis or late-onset carpal instability.
Summary of Landmark Literature and Clinical Guidelines
The contemporary understanding and execution of the radial styloidectomy are heavily predicated on several landmark biomechanical and clinical studies. The foundational work by Watson and Ballet in the 1980s elucidated the predictable, progressive pattern of degenerative changes in the SLAC wrist. Their classification system clearly defined the radioscaphoid articulation as the epicenter of early arthrosis (Stage I), thereby establishing the primary clinical indication for isolated radial styloidectomy. Their observations confirmed that excising the impinging styloid could provide durable pain relief in early-stage disease without destabilizing the midcarpal joint.
The biomechanical parameters of the procedure were definitively established by Siegel and Gelberman. Their seminal cadaveric studies meticulously mapped the origins of the volar radiocarpal ligaments, specifically the Radioscaphocapitate (RSC) and Long Radiolunate (LRL) ligaments. They demonstrated that a resection exceeding 3 to 4 millimeters from the tip of the radial styloid significantly compromised the origin of the RSC ligament, leading to measurable ulnar translation of the carpus under axial load. This research established
