Volar Wrist Surgery: Master the Anatomy of the tendon of the flexor

Key Takeaway
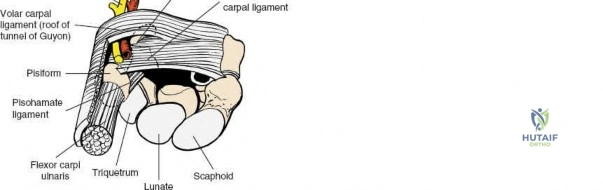
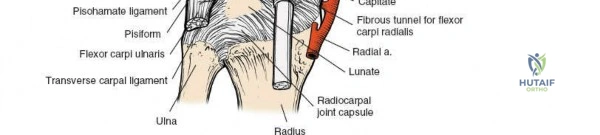
For anyone wondering about Volar Wrist Surgery: Master the Anatomy of the tendon of the flexor, The flexor retinaculum forms the roof of the carpal tunnel, a fibroosseous canal on the wrist's volar surface. It attaches to the pisiform, hook of hamate, ridge of trapezium, and scaphoid tubercle. The pisiform lies within the tendon of the flexor carpi ulnaris, and the tendon of the flexor carpi radialis runs through a tunnel formed by the retinaculum near the trapezium.
Introduction and Epidemiology
The volar aspect of the wrist represents one of the most anatomically dense and surgically significant regions in orthopedic surgery. Mastery of the applied surgical anatomy of the volar wrist is a prerequisite for safely executing a wide array of procedures, ranging from routine carpal tunnel releases to complex intra-articular distal radius fracture fixations and flexor tendon reconstructions. The volar wrist serves as the primary conduit for the flexor tendons, the median nerve, and the ulnar neurovascular bundle as they transition from the forearm into the hand.
Epidemiologically, pathology involving the volar wrist is exceedingly common. Carpal tunnel syndrome remains the most frequently diagnosed compressive neuropathy in the upper extremity, with an estimated prevalence of 3 to 6 percent in the general adult population. Distal radius fractures account for approximately 17.5 percent of all fractures evaluated in emergency departments, and the advent of volar locking plate technology has made the volar approach the gold standard for operative fixation.
Furthermore, flexor tendon lacerations, volar ganglion cysts, and ulnar nerve compression at Guyon’s canal represent significant clinical entities requiring precise surgical intervention. Understanding the intricate relationships between the flexor retinaculum, the carpal bones, and the traversing neurovascular structures is critical to minimizing iatrogenic injury and optimizing functional outcomes.

Surgical Anatomy and Biomechanics
The structural foundation of the volar wrist is defined by the carpal tunnel, a rigid fibroosseous canal. Its base is formed by the deeply concave surface of the volar aspect of the carpal bones, creating the carpal arch. The roof of this canal is formed by the flexor retinaculum, also known as the transverse carpal ligament.

The Flexor Retinaculum and Palpable Landmarks
The flexor retinaculum is a dense connective tissue structure that prevents bowstringing of the flexor tendons during wrist flexion. It features four distinct, palpable bony attachments that serve as critical surgical landmarks:
- The pisiform. Located on the ulnar border of the wrist, the pisiform is a mobile sesamoid bone lying within the tendon of the flexor carpi ulnaris (FCU) muscle. Historically, artisans and cobblers utilized the pisiform to tap nails into soft wood or leather, leading to documented stress fractures in these populations. In contemporary practice, acute fractures are described in contact sports athletes, and pisotriquetral arthrosis is recognized as a specific etiology of ulnar-sided wrist pain.
- The hook of the hamate. Situated slightly distal and radial to the pisiform. To locate it clinically, the interphalangeal joint of the thumb is placed on the pisiform, pointing the tip toward the first web space, resting the tip of the thumb on the palm. The hook of the hamate lies directly under the thumb tip. Because it is enveloped by layers of hypothenar musculature and soft tissue, firm palpation is required to appreciate its shallow contours. The deep motor branch of the ulnar nerve curves directly around the hook, making it highly susceptible to neurapraxia or transection in cases of hamate hook fractures.
- The ridge of the trapezium. The trapezium lies on the radial side of the carpus, articulating with the first metacarpal to form the trapeziometacarpal joint. The ridge can be palpated by passively moving the thumb metacarpal and identifying the prominent lump on the volar aspect of the trapezium.
- The tubercle of the scaphoid. This small protuberance is palpable just distal to the distal radius articular surface on the volar-radial aspect of the wrist joint.

Contents of the Carpal Tunnel
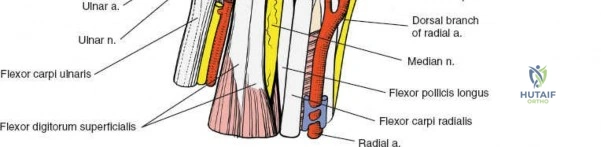
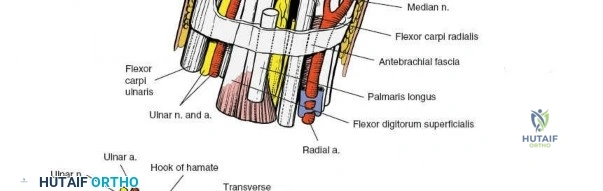
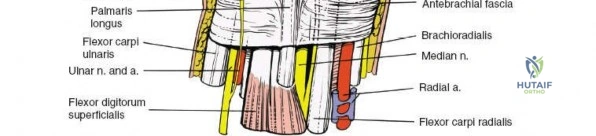
The carpal tunnel contains ten primary structures: the median nerve and nine flexor tendons. The tendons include four flexor digitorum superficialis (FDS) tendons, four flexor digitorum profundus (FDP) tendons, and the flexor pollicis longus (FPL) tendon. The FDS tendons are arranged in a specific spatial orientation within the tunnel, with the tendons to the middle and ring fingers lying volar (superficial) to those of the index and small fingers.

The median nerve typically lies superficial and radial to the superficialis tendons, directly beneath the transverse carpal ligament. Variations in median nerve anatomy, such as a high bifurcation or anomalous motor branch trajectories (transligamentous, preligamentous, or subligamentous), must be anticipated during surgical release.

Flexor Carpi Radialis Tunnel
On the radial aspect of the wrist, the flexor retinaculum attaches across the groove of the trapezium. This attachment converts the groove into a distinct fibroosseous tunnel through which the tendon of the flexor carpi radialis (FCR) muscle runs. After traversing this tunnel, the FCR inserts onto the bases of the second and third metacarpals. The FCR sheath is an essential landmark for the volar approach to the distal radius.

Guyon Canal Anatomy
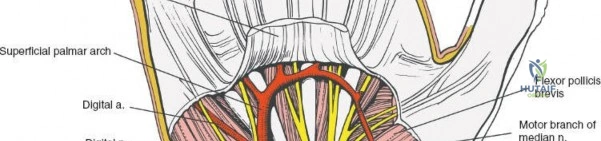
The ulnar nerve and artery do not pass through the carpal tunnel. Instead, they run over the superficial surface of the flexor retinaculum, enclosed within their own fibroosseous canal known as Guyon's canal. The boundaries of Guyon's canal consist of the volar carpal ligament (roof), the transverse carpal ligament and hypothenar muscles (floor), the pisiform and FCU (ulnar border), and the hook of the hamate (radial border). Within this canal, the ulnar nerve bifurcates into the superficial sensory branch and the deep motor branch.
Biomechanics of the Volar Wrist
The flexor retinaculum functions as a critical biomechanical pulley. By tethering the flexor tendons close to the axis of rotation of the radiocarpal and midcarpal joints, it maximizes tendon excursion efficiency and prevents volar bowstringing during forceful wrist and digital flexion. Disruption of this retinaculum alters the moment arms of the flexor tendons, which can result in a measurable decrease in grip strength, a phenomenon often observed transiently following carpal tunnel release.


Indications and Contraindications
Surgical intervention on the volar aspect of the wrist is dictated by a variety of traumatic, degenerative, and compressive pathologies. The decision to proceed with operative management must be carefully weighed against the patient's functional demands, comorbidities, and the specific pathoanatomy.

Operative Indications
The most common indication for exploring the volar wrist is median nerve compression refractory to conservative management. Other primary indications include displaced or unstable distal radius fractures with volar comminution (Smith fractures, volar Barton fractures), acute flexor tendon lacerations (zones IV and V), and ulnar nerve entrapment at the wrist.
Contraindications
Absolute contraindications to elective volar wrist surgery include active local soft tissue infection (unless the procedure is an irrigation and debridement) and severe medical comorbidities precluding anesthesia. Relative contraindications for specific approaches, such as the volar Henry approach for distal radius fractures, include isolated dorsal shear fractures that cannot be adequately reduced or buttressed from a volar approach.

Summary of Operative and Non Operative Management
| Pathology | Operative Indications | Non-Operative Indications |
|---|---|---|
| Carpal Tunnel Syndrome | Refractory to splinting/injections, thenar atrophy, profound sensory loss | Mild to moderate symptoms, intermittent paresthesia, normal EMG/NCS |
| Distal Radius Fracture | Volar tilt >15 degrees, intra-articular step-off >2mm, radial shortening >3mm | Non-displaced fractures, stable reduction in cast, low-demand elderly patients |
| Flexor Tendon Laceration | >60% tendon width laceration, loss of active flexion | <60% laceration without triggering, isolated minor partial tears |
| Ulnar Tunnel Syndrome | Motor weakness, intrinsic atrophy, space-occupying lesion (e.g., ganglion) | Mild sensory symptoms, negative imaging for masses |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is essential for anticipating anatomical variants and ensuring appropriate surgical exposure.

Imaging Modalities
Standard orthogonal radiographs (posteroanterior, lateral, and oblique views) are mandatory for evaluating osseous trauma, carpal alignment, and degenerative changes. For complex intra-articular fractures, computed tomography (CT) with sagittal and coronal reconstructions provides critical detail regarding articular step-offs and fragment morphology. Magnetic resonance imaging (MRI) is the modality of choice for evaluating occult space-occupying lesions within the carpal tunnel or Guyon's canal, such as lipomas, ganglion cysts, or anomalous muscle bellies.

Electrodiagnostic Studies
Electromyography (EMG) and nerve conduction studies (NCS) provide objective data regarding the severity and chronicity of nerve compression. They are particularly useful in differentiating radiculopathy or proximal compression (e.g., pronator syndrome) from distal entrapment at the wrist.

Patient Positioning and Operating Room Setup
The patient is positioned supine with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm.

The arm is exsanguinated with an Esmarch bandage, and the tourniquet is typically inflated to 250 mmHg or 100 mmHg above the patient's systolic blood pressure. Loupe magnification (2.5x to 3.5x) is highly recommended for meticulous identification of the palmar cutaneous branch of the median nerve and the digital nerves.
Detailed Surgical Approach and Technique
The volar aspect of the wrist can be accessed via several distinct surgical approaches, depending on the target pathology. The two most fundamental approaches are the standard carpal tunnel approach and the extended flexor carpi radialis (Henry) approach.
Standard Carpal Tunnel Release
The incision is planned in the palm, typically in line with the radial border of the ring finger, remaining ulnar to the thenar crease to avoid injury to the palmar cutaneous branch of the median nerve (PCBMN).

The superficial dissection proceeds through the skin and subcutaneous fat. The palmar aponeurosis is identified and longitudinally incised. Blunt retractors are placed to protect the underlying structures. The transverse carpal ligament is identified by its transversely oriented fibers.

The ligament is divided longitudinally from proximal to distal. The surgeon must stay on the ulnar side of the median nerve to avoid the recurrent motor branch, which typically arises from the radial aspect of the nerve just distal to the ligament.

Once the ligament is completely transected, the median nerve is inspected for hour-glassing or hyperemia. The proximal forearm fascia is also released for 2 to 3 centimeters to ensure no proximal tethering remains.

Volar Approach to the Distal Radius
The volar approach, utilizing the interval between the FCR and the radial artery, is the standard for distal radius fracture fixation.

A longitudinal incision is made directly over the course of the FCR tendon, extending proximally from the wrist crease. The FCR tendon sheath is incised longitudinally.

The FCR tendon is retracted ulnarly, protecting the median nerve which lies immediately ulnar to it. Retracting the tendon radially is discouraged as it places tension on the palmar cutaneous branch of the median nerve.

The floor of the FCR sheath is incised, exposing the underlying pronator quadratus muscle. The radial artery is identified and gently retracted radially.
The pronator quadratus is elevated off the volar surface of the radius via an L-shaped incision along its radial and distal borders. This subperiosteal elevation exposes the entire volar metaphysis of the distal radius, allowing for fracture reduction and application of a volar locking plate.
Guyon Canal Release
For ulnar nerve entrapment, an incision is made along the ulnar border of the hypothenar eminence, curving radially across the wrist crease toward the FCU tendon.

The palmaris brevis muscle is divided. The volar carpal ligament is incised, exposing the ulnar neurovascular bundle. The ulnar artery typically lies radial to the nerve.

The nerve is traced distally to its bifurcation into the superficial and deep branches. The deep branch must be followed as it dives between the abductor digiti minimi and the flexor digiti minimi, wrapping around the hook of the hamate. The fibrous arch of the hypothenar muscles is released to ensure complete decompression of the motor branch.
Complications and Management
Surgery on the volar wrist carries a distinct set of potential complications, primarily related to the dense neurovascular anatomy. Meticulous surgical technique and a thorough understanding of anatomical danger zones are required to minimize morbidity.

Iatrogenic Nerve Injury
Injury to the palmar cutaneous branch of the median nerve (PCBMN) is a devastating complication that can result in a painful neuroma. The PCBMN typically branches from the median nerve 5 cm proximal to the wrist crease, traveling between the palmaris longus and FCR before crossing the superficial surface of the flexor retinaculum. Transverse incisions across the wrist crease should be avoided or performed with extreme caution to prevent transection of this nerve.

Injury to the recurrent motor branch of the median nerve can occur if the transverse carpal ligament is released too far radially. This results in profound weakness of thumb opposition and thenar atrophy.
Tendon Complications
Following volar plating of the distal radius, flexor tendon irritation or rupture can occur if the plate is positioned distal to the watershed line. The FPL tendon is particularly vulnerable as it sweeps across the volar-radial aspect of the distal radius. Prominent hardware must be avoided, and the plate should be recessed proximal to the watershed line.

Bowstringing of the flexor tendons can occur following aggressive or complete release of the flexor retinaculum, particularly if accompanied by an extensive release of the distal forearm fascia. This biomechanical failure leads to a loss of grip strength and potential flexion contractures.

Summary of Complications and Salvage Strategies
| Complication | Estimated Incidence | Prevention and Salvage Strategies |
|---|---|---|
| PCBMN Neuroma | 1-2% | Stay ulnar to thenar crease; salvage via neuroma excision and burying proximal stump into pronator quadratus. |
| Incomplete TCL Release | 2-5% | Ensure direct visualization of distal edge of retinaculum and fat pad; salvage via revision open release. |
| FPL Tendon Rupture | 1-3% (Post-plating) | Keep plate proximal to watershed line; salvage via FDS to FPL tendon transfer or tendon graft. |
| Pillar Pain | 10-25% | Avoid excessive retraction of hypothenar/thenar musculature; usually self-limiting, manage with desensitization therapy. |
| Superficial Palmar Arch Injury | <1% | Direct visualization during distal extension of carpal tunnel release; salvage via microsurgical repair or ligation if collateral flow is adequate. |
Post Operative Rehabilitation Protocols
Rehabilitation following volar wrist surgery is highly dependent on the specific procedure performed and the stability of the underlying tissues.

Nerve Decompression Rehabilitation
Following isolated carpal tunnel or Guyon's canal release, early active range of motion of the digits is encouraged immediately postoperatively to prevent perineural adhesions and tendon tethering. The wrist is typically supported in a bulky soft dressing or a removable volar splint for 1 to 2 weeks. Heavy lifting and forceful gripping are restricted for 4 to 6 weeks to allow the flexor retinaculum to heal in a lengthened position without predisposing the tendons to bowstringing.

Distal Radius Fracture Rehabilitation
For distal radius fractures treated with rigid volar locking plates, early mobilization is the standard of care. Patients are placed in a removable splint and instructed to begin active digital and radiocarpal motion within the first postoperative week. This early motion protocol significantly reduces the incidence of joint stiffness and complex regional pain syndrome (CRPS). Strengthening exercises are progressively introduced between 6 and 8 weeks postoperatively, contingent upon radiographic evidence of fracture consolidation.

Flexor Tendon Repair Protocols
Rehabilitation following flexor tendon repair in the volar wrist (Zones IV and V) requires a delicate balance between protecting the repair site and preventing restrictive adhesions. Protocols such as the Modified Duran or the Kleinert protocol utilize dorsal blocking splints to prevent active wrist and digital extension while allowing controlled passive flexion and active extension within the constraints of the splint. True active flexion is typically delayed until 4 weeks postoperatively.
Summary of Key Literature and Guidelines
Evidence-based practice in volar wrist surgery is supported by extensive anatomical and clinical literature.

The American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines for the Management of Carpal Tunnel Syndrome strongly recommend surgical release for patients with severe neurophysiologic deficits or those unresponsive to non-operative modalities. The literature demonstrates no clinically significant long-term difference in outcomes between open and endoscopic carpal tunnel release, though endoscopic techniques may offer a faster return to work with a slightly higher risk of transient nerve injury.

Regarding the volar approach to the distal radius, seminal work by Orbay et al. established the biomechanical advantages of the volar locking plate, particularly in osteoporotic bone. Subsequent anatomical studies have emphasized the critical concept of the "watershed line"—the transverse ridge marking the distal margin of the pronator fossa. Literature consistently demonstrates that prominent hardware placed distal to this line significantly increases the risk of flexor tendon attrition and rupture.

Finally, anatomical studies detailing the variations of the median nerve and the PCBMN underscore the necessity of meticulous surgical technique. The classic anatomical studies by Lanz categorized median nerve variations into four groups, highlighting the frequency of anomalous motor branches and accessory nerve bundles. Familiarity with this literature is essential for any surgeon operating within the complex landscape of the volar wrist.

