Arthroscopic Dorsal Radiocarpal Ligament Repair: An Intraoperative Masterclass

Key Takeaway
This masterclass guides you through arthroscopic dorsal radiocarpal ligament (DRCL) repair. We cover comprehensive wrist anatomy, meticulous preoperative planning, and granular, step-by-step intraoperative execution from a surgeon's perspective. Learn precise portal placement, suture management, and thermal augmentation. Critical pearls, pitfalls, and comprehensive postoperative rehabilitation protocols are emphasized for optimal patient outcomes in isolated and associated DRCL tears.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater and to this definitive exploration of an often-underestimated etiology of persistent wrist pain: tears of the dorsal radiocarpal ligament (DRCL). Historically, the intricate capsular ligaments of the wrist were frequently overlooked in favor of the more prominent primary interosseous stabilizers, such as the scapholunate interosseous ligament (SLIL) and the lunotriquetral interosseous ligament (LTIL). However, as our arthroscopic visualization and understanding of carpal kinematics have evolved, we now recognize that DRCL tears are far more common than previously suspected. Furthermore, these lesions are beautifully amenable to arthroscopic repair, provided the surgeon possesses a meticulous technique and a profound, three-dimensional understanding of wrist anatomy.
The epidemiology of DRCL injuries is intrinsically linked to both acute traumatic events and chronic, repetitive microtrauma. Patients frequently present with a history of a sudden loading event to a dorsiflexed and ulnarly deviated wrist, or conversely, a history of repetitive torquing movements required in certain occupations and athletic pursuits. Unrecognized DRCL tears constitute a significant, yet frequently missed, cause of treatment failure in patients presenting with persistent dorsal wrist pain. In the realm of non-dissociative carpal instability, the pain is often attributed to dynamic joint incongruity; however, it is highly plausible that the torn, hyperplastic edge of the DRCL impinges against the lunate or adjacent carpal bones during physiologic motion, generating a localized, painful synovitis.
The paradigm shift in modern wrist surgery involves recognizing the profound proprioceptive role of these secondary stabilizers. The DRCL is not merely a static mechanical checkrein; it is a dynamic sensory organ. The ligament and its enveloping epiligamentous sheath are richly innervated, accounting for up to 80% of the mechanoreceptors in the dorsal radiocarpal region. This dense neurohistological profile suggests a significant proprioceptive function, highly analogous to the anterior cruciate ligament in the knee. Consequently, repairing a torn DRCL achieves far more than simply restoring mechanical tethering; it re-establishes the crucial afferent neuromuscular feedback loop necessary for dynamic carpal stability.
As we delve into this masterclass, it is imperative to view the wrist as a complex, interdependent continuum of primary and secondary stabilizers. While isolated DRCL tears can independently generate chronic, debilitating wrist pain, their presence alongside injuries to the SLIL, LTIL, or triangular fibrocartilage complex (TFCC) often signifies a more profound degree of carpal instability. Addressing only the primary lesion while ignoring a concomitant DRCL tear typically portends a poorer clinical prognosis. This chapter will exhaustively detail the anatomical, diagnostic, and technical nuances required to master arthroscopic DRCL repair.
Detailed Surgical Anatomy and Biomechanics
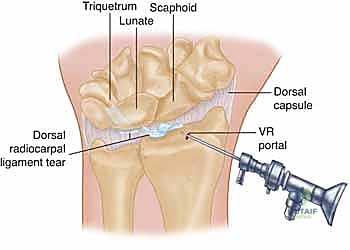
The dorsal radiocarpal ligament is a robust, extracapsular structure situated on the dorsum of the wrist, serving as a critical secondary stabilizer of the proximal carpal row. Its anatomical journey is distinct and clinically highly relevant. The ligament originates from a broad footprint on the dorsal aspect of the distal radius, specifically centered around the tubercle of Lister. From this robust origin, the fibers course obliquely in a distal and ulnar direction. While its primary and most substantial insertion is onto the dorsal tubercle of the triquetrum, the DRCL is not a simple, singular cord. Its radial-sided fibers provide highly significant, albeit thinner, attachments to the dorsal horn of the lunate and the dorsal aspect of the lunotriquetral interosseous ligament (LTIL).
When evaluating the wrist arthroscopically, particularly from the volar radial (VR) portal, the DRCL is typically visualized immediately ulnar to the standard 3-4 dorsal portal trajectory, positioned directly superficial to the lunate. It is critical for the arthroscopist to recognize that the actual longitudinal collagen fibers of the ligament may not be readily visible in a healthy wrist. Normally, the DRCL is enveloped and protected by a thin, highly vascularized, and critically important epiligamentous sheath. It is this sheath that houses the majority of the pacinian corpuscles and Ruffini endings responsible for the ligament's proprioceptive capabilities.
Biomechanically, the wrist relies on a complex interplay of primary and secondary stabilizers to maintain synchronous carpal alignment under load. The SLIL, LTIL, and TFCC act as the primary stabilizers, bearing the brunt of axial loading and preventing intercarpal dissociation. The capsular ligaments, including the DRCL and the dorsal intercarpal (DIC) ligament, function as vital secondary stabilizers. The DIC originates from the triquetrum and extends radially to insert on the lunate, the dorsal scaphoid groove, and the trapezium. Together, the DIC and the DRCL form a lateral "V" configuration, effectively acting as a dorsal radioscaphoid ligament complex that stabilizes the proximal row during dynamic flexion, extension, and radio-ulnar deviation.
Pathoanatomically, a chronic tear of a primary stabilizer can lead to compensatory attenuation, cyclical stress, and eventual tearing of these secondary capsular ligaments. When the DRCL tears, it typically fails near its origin at Lister's tubercle or mid-substance, leading to a redundant, frayed ligamentous stump. This stump can interpose itself between the radius and the proximal carpal row during wrist extension, causing mechanical impingement and localized synovitis. Understanding this complex biomechanical relationship is essential for recognizing why isolated DRCL repairs succeed, and why combined capsular and interosseous ligament repairs are necessary in more advanced stages of carpal instability.

Exhaustive Indications and Contraindications
The clinical presentation of a patient with an isolated DRCL tear is notoriously subtle, demanding a high index of suspicion from the examining surgeon. Our typical patient will present with complaints of intermittent, dorsal midline wrist pain that is often described as a deep ache. This pain may be sporadic, lasting a few days, and is predictably precipitated or exacerbated by repetitive loading, weight-bearing across the extended wrist, or torquing movements. Crucially, there are no pathognomonic physical examination findings for an isolated DRCL tear. While some patients may exhibit mild point tenderness directly over the tubercle of Lister, this is not universally present.
Because physical examination is often equivocal, our diagnostic algorithm must be systematic and thorough. Plain radiographs (including PA, lateral, oblique, and clenched fist views) are mandatory to assess for static carpal instability patterns (such as VISI or DISI), degenerative changes, or occult fractures, though they are typically normal in isolated DRCL tears. Conventional MRI, while our gold standard for many soft tissue pathologies, can be highly misleading in this context. It is not uncommon for an MRI to be misinterpreted as showing a simple dorsal ganglion cyst due to a high fluid signal intensity localized over the dorsal capsule, when in fact, this fluid represents an effusion leaking through a DRCL defect. Therefore, an MR arthrogram or a double-row wrist arthrogram is highly recommended to meticulously evaluate the primary interosseous ligaments and the integrity of the dorsal capsule.
We classify DRCL tears based on the presence or absence of associated carpal pathology, utilizing a staging system that directly guides our operative strategy. Stage 1 represents an isolated DRCL tear. Stage 2 involves a DRCL tear with an associated SLIL or LTIL tear (Geissler stage 1 or 2) or a peripheral TFCC tear. Stage 3A features a DRCL tear with a more significant SLIL and/or LTIL tear (Geissler stage 3) and/or a TFCC tear. Stage 3B is defined by a DRCL tear with a complete SLIL and/or LTIL disruption (Geissler stage 4). Finally, Stage 4 denotes widespread carpal pathology with advanced chondromalacia. The ligament with the highest Geissler grade dictates the overall stage, with each successive stage denoting a longer-standing or more severe condition that impacts the ultimate prognosis.
Arthroscopic repair is unequivocally indicated for Stage 1 (isolated) DRCL tears that have failed a comprehensive trial of nonoperative management. We also strongly consider arthroscopic repair for Stage 2 and Stage 3A tears, provided the associated interosseous ligament or TFCC pathology can be simultaneously addressed via arthroscopic techniques. However, for Stage 3B and Stage 4 tears, the outcomes of isolated or even combined arthroscopic DRCL repair become highly unpredictable. In these advanced scenarios, the degree of carpal collapse and fixed deformity usually necessitates more invasive open procedures.
| Category | Specific Criteria |
|---|---|
| Indications | Stage 1 Isolated DRCL tear failing > 3 months non-op management. |
| Stage 2 DRCL tear with Geissler 1/2 SLIL/LTIL tears amendable to arthroscopy. | |
| Stage 3A DRCL tear with Geissler 3 SLIL/LTIL tears (combined repair planned). | |
| Persistent dorsal impingement pain with MRI-confirmed capsular defect. | |
| Contraindications | Stage 3B (Geissler 4) tears with fixed carpal malalignment (DISI/VISI). |
| Stage 4 widespread radiocarpal or midcarpal chondromalacia/arthritis. | |
| Active localized soft tissue infection or untreated osteomyelitis. | |
| Patient non-compliance or inability to adhere to strict post-operative splinting. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a fluid and successful arthroscopic DRCL repair. The surgeon must meticulously review all imaging modalities, particularly the MR arthrogram, to anticipate the exact location of the capsular defect and to pre-emptively identify any concomitant SLIL, LTIL, or TFCC pathology. Equipment preparation is equally critical. A modern, high-definition digital arthroscopy tower is mandatory to visualize the delicate epiligamentous structures. The procedure requires a 2.7-mm, 30-degree angled arthroscope, standard diagnostic instruments including a 3-mm hook-probe, and specialized debridement tools such as a motorized shaver (2.0 mm or 2.9 mm) and suction punch forceps.
Furthermore, the surgeon must ensure the availability of a radiofrequency (RF) diathermy unit, such as an Oratec probe, which is indispensable for debriding localized synovitis and, more importantly, for augmenting the repair via thermal capsular shrinkage. For suture management, a variety of curved and straight 18-gauge spinal needles are required for the outside-in suture passage technique. A dedicated suture lasso or micro-grasper is absolutely necessary for retrieving suture ends within the tight confines of the radiocarpal joint.
Patient positioning and the application of traction are paramount for optimizing joint distraction and ensuring safe instrument maneuverability. The patient is positioned supine on the operating table with the operative arm abducted to 90 degrees and supported on a dedicated hand table. Regional anesthesia (such as a supraclavicular or axillary block) is generally preferred, supplemented with a well-padded proximal pneumatic tourniquet. We apply axial traction using a specialized wrist traction tower (e.g., the ARC wrist traction tower). The hand is suspended via sterile finger traps applied to the index and middle fingers; occasionally, the ring finger is included to afford better control over ulnar deviation.
Typically, 5 to 10 pounds of traction is applied. It is imperative that this traction is applied axially, aligning perfectly with the forearm to maximize radiocarpal and midcarpal joint distraction without imparting undue stress on the elbow or shoulder joints. The forearm is securely strapped to the arm board to prevent inadvertent rotation during the procedure. Finally, a C-arm fluoroscope should be draped and positioned perpendicular to the hand table, allowing for seamless anteroposterior (AP) and lateral radiographic views without requiring repositioning of the patient's arm. This fluoroscopic capability is crucial for confirming precise portal placement and assessing dynamic carpal alignment intraoperatively.
Step-by-Step Surgical Approach and Fixation Technique
Portal Placement and Diagnostic Arthroscopy
The surgical approach begins with the meticulous establishment of standard and specialized arthroscopic portals. The dorsal portals (3-4, 4-5, and 6R/6U) are established first, utilizing a standard "nick and spread" technique with a blunt hemostat to protect the underlying extensor tendons and the delicate branches of the superficial radial and dorsal ulnar sensory nerves. The 3-4 portal, located between the extensor pollicis longus (EPL) and the extensor digitorum communis (EDC), serves as our initial viewing portal for the standard diagnostic sweep. During this sweep, the SLIL, LTIL, and TFCC are systematically probed to rule out occult pathology.
However, the definitive visualization and repair of the DRCL require the establishment of the Volar Radial (VR) portal. This portal is technically demanding but absolutely essential. The surface landmark is the flexor carpi radialis (FCR) tendon at the level of the proximal wrist crease. A 2 cm longitudinal incision is made centered over the FCR. The superficial fascia is incised, and the FCR tendon sheath is opened. The FCR tendon is then retracted ulnarly. This specific retraction is a critical safety maneuver: the radial artery lies radial to the FCR, and the median nerve lies ulnar to it. By retracting the FCR ulnarly, the surgeon effectively protects both of these vital neurovascular structures, exposing the volar radiocarpal capsule directly beneath.

An 18-gauge spinal needle is then introduced through the exposed volar capsule, directed dorsally and slightly ulnarly, aiming towards the radiocarpal joint under direct visualization from the 3-4 dorsal portal. Once the needle trajectory is confirmed to be intra-articular and free of the scaphoid and lunate, the capsule is incised, and the arthroscope is transitioned to the VR portal.
Ligament Preparation and Debridement
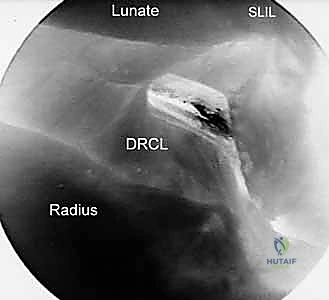
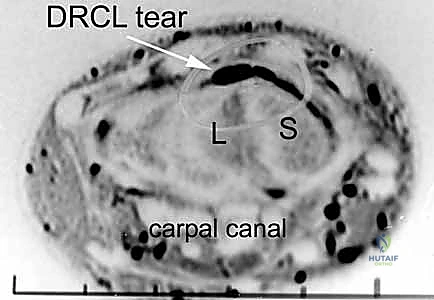
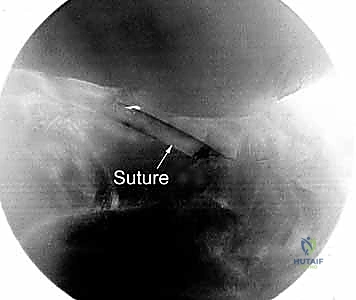
Viewing from the VR portal completely alters the arthroscopic perspective, providing a panoramic view of the dorsal capsule and the DRCL. From this vantage point, the normal DRCL is seen sweeping obliquely from Lister's tubercle towards the triquetrum. When a tear is present, it is typically identified as a focal defect, a redundant flap of tissue, or an area of profound, localized hypervascular synovitis directly overlying the lunate or the radiocarpal joint line.

Once the tear is identified, meticulous preparation of the tear edges is paramount for biological healing. A 2.9-mm motorized shaver is introduced through the 3-4 or 4-5 portal to carefully debride the reactive synovitis and the frayed, necrotic edges of the torn ligament. This debridement must be thorough enough to expose healthy, bleeding collagenous tissue but conservative enough to avoid excising viable ligament that is needed for the repair.

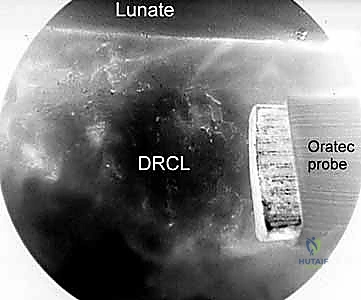
Following mechanical debridement, a radiofrequency (RF) diathermy probe is introduced. The RF probe serves a dual purpose: it provides excellent hemostasis in this highly vascular region, and it can be used to gently shrink and consolidate the attenuated edges of the DRCL, making them more robust for subsequent suture passage. The thermal energy must be applied judiciously to avoid thermal necrosis of the ligament or the adjacent articular cartilage of the lunate and radius.
Suture Passage and Knot Tying
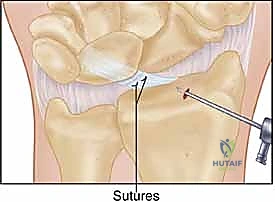
The core of the repair utilizes an outside-in suture passage technique. While viewing from the VR portal, an 18-gauge spinal needle, loaded with a 2-0 or 3-0 PDS (polydioxanone) or non-absorbable braided suture, is introduced percutaneously through the dorsal skin, targeting the ulnar aspect of the DRCL tear. The needle pierces the intact dorsal capsule and passes through the ulnar leaf of the torn ligament. The suture is advanced into the joint, and the needle is withdrawn.
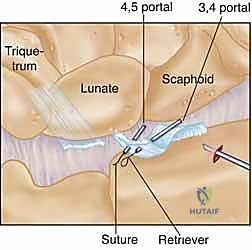
A second 18-gauge spinal needle, loaded with a specialized wire loop or a suture lasso, is then introduced just adjacent to the first needle puncture. This second needle is directed through the radial leaf of the torn DRCL. Once inside the joint, the suture lasso is deployed. A micro-grasper, introduced through a working portal (typically the 4-5 or 6R), is used to manipulate the free end of the previously passed PDS suture and feed it through the wire loop of the lasso.
The lasso is then retracted, pulling the PDS suture out through the second needle tract. This creates a horizontal mattress or a simple interrupted suture configuration that securely spans the DRCL defect. This process is repeated as necessary, typically requiring two to three distinct sutures to achieve a watertight and mechanically sound closure of the capsular defect.
Final Assessment and Closure
Once all sutures are passed, they are tied blindly over the dorsal capsule but deep to the extensor tendons through a small dorsal incision connecting the needle puncture sites. Before the final knots are secured, the axial traction on the wrist is released. Tying the sutures with the wrist in a neutral, un-distracted position is critical to prevent over-tensioning the repair, which could lead to severe post-operative stiffness and a loss of palmar flexion.
After the knots are tied, the arthroscope is reintroduced through the VR portal to directly visualize the final repair. The surgeon must confirm that the capsular defect is completely closed, that the DRCL is appropriately tensioned, and that no redundant tissue remains to impinge within the radiocarpal joint. The repair is gently probed to ensure mechanical integrity.

Finally, the joint is thoroughly irrigated to remove any remaining debris. The VR portal incision requires meticulous closure, ensuring the FCR tendon sheath is re-approximated if possible, followed by standard skin closure. The dorsal portals are typically closed with simple nylon sutures or adhesive strips. The wrist is immediately placed in a bulky dressing and a rigid volar splint with the wrist in neutral extension.
Complications, Incidence Rates, and Salvage Management
While arthroscopic DRCL repair is generally safe and highly effective, it is a technically demanding procedure fraught with potential complications if anatomical landmarks are not strictly respected. The most feared complications are iatrogenic neurovascular injuries. The establishment of the VR portal places the radial artery and the palmar cutaneous branch of the median nerve at significant risk. Strict adherence to the technique of incising the FCR sheath and retracting the tendon ulnarly is the primary defense against this catastrophic complication. Dorsally, the superficial sensory branch of the radial nerve and the dorsal cutaneous branch of the ulnar nerve are at risk during portal placement and percutaneous suture passage.
Iatrogenic cartilage damage is another significant concern. The radiocarpal joint is a tight space, and the introduction of rigid trocars, shavers, and RF probes can easily score the delicate articular cartilage of the radius, scaphoid, or lunate. Maintaining adequate axial traction and utilizing a 2.7-mm (rather than a 4.0-mm) arthroscope minimizes this risk. Post-operative infection, while rare in arthroscopic procedures (incidence < 1%), remains a possibility and requires standard sterile precautions and appropriate perioperative antibiotic prophylaxis.
The most common post-operative complication is transient wrist stiffness, particularly a loss of terminal palmar flexion, which is an expected consequence of capsular plication. However, severe, recalcitrant stiffness or the development of Complex Regional Pain Syndrome (CRPS) can occur and requires aggressive, early intervention with specialized hand therapy and potentially sympathetic nerve blocks. Recurrent instability or failure of the repair is typically seen in patients with unrecognized, high-grade primary stabilizer injuries (e.g., missed Geissler 3/4 SLIL tears) or in patients who fail to comply with post-operative immobilization protocols.
For patients who fail arthroscopic DRCL repair, salvage options become progressively more invasive. If the failure is due to isolated capsular attenuation without fixed carpal collapse, an open dorsal capsulodesis (such as a Blatt capsulodesis) may be indicated. However, if the failure is associated with progressive carpal instability (DISI/VISI) and early chondromalacia, salvage procedures shift toward partial carpal fusions (e.g., scaphoid-trapezium-trapezoid fusion, scaphocapitate fusion) or a proximal row carpectomy (PRC) to provide definitive pain relief at the expense of motion.
| Complication | Estimated Incidence | Prevention and Management Strategy |
|---|---|---|
| Superficial Nerve Injury | 2% - 5% | Blunt dissection for dorsal portals; careful percutaneous needle placement. Manage with observation, gabapentin; surgical neurolysis if neuroma forms. |
| Radial Artery Laceration | < 1% | Strict ulnar retraction of FCR during VR portal creation. Requires immediate open vascular repair if injured. |
| Iatrogenic Cartilage Scuffing | 5% - 10% | Maintain 5-10 lbs axial traction; use 2.7mm scope; direct visualization of instrument entry. Usually asymptomatic, but avoid deep gouges. |
| Post-operative Stiffness | 15% - 20% | Tie |
