Complex Elbow Dislocation with PMRRI and Coronoid Fracture: Clinical Presentation & Diagnostic Insights

Key Takeaway
Posteromedial Rotatory Instability (PMRRI) is a complex elbow dislocation, often with an anteromedial coronoid fracture (O'Driscoll Type III). Diagnosis involves clinical assessment for post-reduction instability and critical CT imaging. CT scans precisely define fracture morphology, essential for accurate orthopedic diagnosis and guiding optimal surgical management plans.
A 48-year-old male presents with this elbow injury after a fall on an outstretched hand. The elbow was reduced in the ED, but remains unstable to varus stress. Look at the provided imaging. What is your diagnosis, and how does this biomechanically differ from a "Terrible Triad" injury?
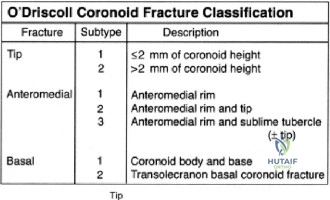

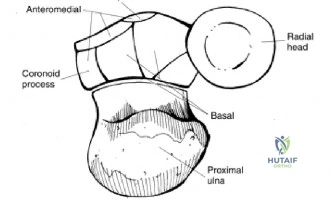
Candidate: The patient has a varus posteromedial rotatory instability (VPMRI) of the elbow. This is characterized by an anteromedial coronoid facet fracture and a lateral collateral ligament (LCL) complex tear. Unlike the Terrible Triad, which is caused by valgus/axial loading and involves a radial head fracture and transverse coronoid fracture, VPMRI is caused by varus/axial loading with pronation, shearing off the medial buttress of the coronoid.
Candidates often miss the specific mechanism, merely calling it a "complex dislocation." They fail to emphasize the O'Driscoll classification or the critical distinction that VPMRI involves the *anteromedial facet* rather than the *coronoid tip*, which is the hallmark of the Terrible Triad.
Define the injury as Varus Posteromedial Rotatory Instability (VPMRI). Explain the biomechanics: VPMRI is a shear injury caused by varus stress driving the medial trochlea into the anteromedial coronoid facet. Contrast this with the Terrible Triad (Valgus/Axial/Supination) which results in a Radial Head fracture and transverse coronoid tip fracture. Mention the O'Driscoll Type II fracture and highlight the loss of the medial buttress, which makes the joint inherently unstable even if the LCL is repaired.
You have decided to proceed to surgery. Describe your management strategy for the medial side. Specifically, how do you manage the ulnar nerve and what is your surgical goal for the anteromedial coronoid fragment?
Candidate: I would use a medial approach. I would identify and decompress the ulnar nerve, protecting it throughout. I would use an FCU-split approach to visualize the anteromedial facet. The goal is anatomical reduction of the fragment and rigid fixation using a buttress plate, as this is the primary medial constraint. I would then address the lateral side separately.
Failing to mention the "buttress" principle. Some candidates suggest simple screw fixation, which may be insufficient for comminuted fractures. Also, forgetting to explicitly state the management of the ulnar nerve during the medial approach is a common procedural oversight.
The goal is to restore the "medial column." Approach: Medial incision, routine identification and protection of the ulnar nerve (anterior transposition is often practiced to avoid iatrogenic neuropraxia). Use the FCU-split interval to access the sublime tubercle. Fixation: A pre-contoured anteromedial coronoid buttress plate is mandatory. If the fragment is too small, use suture lasso techniques through the plate. Crucially, emphasize that medial fixation is performed before the lateral repair to provide a stable foundation.
The surgery has been completed. What does your rehabilitation protocol look like, and which specific movement must be avoided during the first 6 weeks to protect the lateral collateral ligament (LCL) repair?
Candidate: Rehabilitation involves a hinged brace. I would allow early active flexion/extension but keep the forearm in pronation. The movement to avoid is supination, especially in extension, as this is the mechanism that stresses the LCL repair and could lead to recurrent subluxation.
Suggesting "complete immobilization" or being vague about the forearm position. Failing to mention why pronation is used (to close the lateral joint space) indicates a lack of conceptual understanding of the biomechanics.
Structure the rehab into phases: Phase I (0-2w) splinted in 90-deg flexion/pronation. Phase II (2-6w) hinged brace allowing flexion/extension, maintaining pronation. Crucial Warning: Supination, particularly combined with elbow extension, must be avoided as this is the primary mechanism for VPMRI and directly antagonizes the LCL repair. Also, advise the patient to avoid shoulder abduction/internal rotation ("chair push-up") to prevent varus stress.
