Surgical Management of Unreduced Elbow Dislocation
Key Takeaway
Chronic unreduced elbow dislocations present a formidable challenge in orthopedic surgery, often requiring extensive soft tissue mobilization and specialized techniques such as V-Y triceps lengthening. This comprehensive guide details the step-by-step surgical approach, biomechanical considerations, and postoperative protocols necessary to restore joint congruity and function. It also explores salvage options, including interpositional arthroplasty and total elbow arthroplasty, for cases with severe articular degeneration.
Comprehensive Introduction and Patho-Epidemiology
An old, unreduced elbow dislocation represents one of the most profoundly debilitating conditions encountered in orthopedic traumatology, presenting a formidable reconstructive challenge even to the most experienced upper extremity surgeon. Defined generally in the literature as a dislocation that has remained unreduced for longer than three weeks, this pathology is characterized by a cascade of severe soft tissue contractures, myostatic shortening of the triceps brachii, and extensive fibro-osseous proliferation that completely obliterates the normal articular kinematics. While acute elbow dislocations are typically managed successfully with closed reduction and early mobilization, chronic unreduced dislocations are frequently the result of delayed presentation, missed diagnoses in the polytraumatized patient, or inadequate initial immobilization, particularly in developing nations or rural healthcare settings.
The pathoanatomy of the chronic unreduced elbow is complex and progressive. At the time of the initial violent traumatic event, the displacement of the radius and ulna—most commonly in a posterolateral direction—strips the periosteum and capsuloligamentous structures from the distal humerus. In the neglected state, this elevated periosteum, combined with the massive fracture-dislocation hematoma, acts as an osteogenic factory. The hematoma subsequently undergoes aggressive heterotopic ossification, filling the olecranon and coronoid fossae with dense, unyielding callus and fibrotic scar tissue. Concurrently, the collateral ligaments, specifically the medial ulnar collateral ligament (MUCL) and the lateral ulnar collateral ligament (LUCL), heal in a contracted, non-anatomic, and mechanically disadvantageous position.
Furthermore, the articular cartilage undergoes rapid and often irreversible degradation. Deprived of normal synovial fluid nutrition—which relies on the cyclical loading and unloading of the joint for diffusion—and subjected to abnormal, concentrated mechanical pressures from the dislocated bony architecture, the chondrocytes undergo apoptosis. Fibrillation, full-thickness cartilage loss, and subchondral cystic changes ensue. Successful management, therefore, requires a meticulous, stepwise surgical approach tailored to the chronicity of the injury. The primary operative goals are to restore ulnohumeral and radiocapitellar congruity, reconstruct or release the contracted stabilizing ligaments, and regain a functional arc of motion. For cases with severe chronicity (typically greater than six months) or catastrophic articular destruction, joint preservation is often futile, and salvage procedures such as interpositional arthroplasty or total elbow arthroplasty (TEA) must be strongly considered.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of elbow surgical anatomy and biomechanics is the absolute prerequisite for attempting the reconstruction of a chronic unreduced dislocation. The elbow is a highly constrained, complex hinge joint composed of three distinct articulations: the ulnohumeral, radiocapitellar, and proximal radioulnar joints. The ulnohumeral articulation is the primary static stabilizer of the elbow. The highly congruent fit of the greater sigmoid notch of the ulna around the trochlea of the distal humerus provides intrinsic osseous stability, particularly in extension. In a chronic posterior dislocation, the coronoid process of the ulna becomes lodged in the olecranon fossa, while the olecranon rests abnormally proximal to the posterior humeral cortex, leading to severe bony remodeling and blunting of these critical osseous restraints.
The ligamentous anatomy is equally compromised in the chronic state. The medial collateral ligament (MCL) complex consists of anterior, posterior, and transverse bundles. The anterior bundle is the primary restraint to valgus stress and is taut throughout the entire arc of flexion. The lateral collateral ligament (LCL) complex includes the radial collateral ligament, the annular ligament, and the lateral ulnar collateral ligament (LUCL). The LUCL is the primary restraint to posterolateral rotatory instability (PLRI). In an unreduced dislocation, these capsuloligamentous complexes are avulsed from their epicondylar origins and heal in shortened, fibrotic masses that tether the joint in its dislocated position. Surgical reduction requires extensive, virtually circumferential capsular release and frequently necessitates ligamentous reconstruction using autograft or allograft tissue to restore stability once the joint is reduced.
The musculotendinous units crossing the elbow joint undergo severe myostatic contracture, presenting one of the greatest hurdles to surgical reduction. The triceps brachii, crossing the posterior aspect of the joint, shortens significantly. Attempting to force reduction against a contracted triceps will invariably lead to iatrogenic fractures of the osteopenic distal humerus or olecranon. Anteriorly, the brachialis and biceps brachii also contract, tethering the anterior capsule and encasing the neurovascular structures in dense scar tissue. The ulnar nerve, situated in the cubital tunnel posterior to the medial epicondyle, is at extreme risk. The altered osseous anatomy stretches the nerve over the displaced medial epicondyle, and the ensuing perineural fibrosis tethers the nerve, making it highly susceptible to intraoperative traction injury during reduction maneuvers.
Exhaustive Indications and Contraindications
The decision-making algorithm for treating a chronic unreduced elbow dislocation hinges on the patient's age, functional demands, chronicity of the dislocation, and the viability of the articular cartilage. Joint-preserving open reduction is the gold standard for younger, active patients presenting within the first 3 to 6 months of injury. The primary indication is a rigidly fixed elbow with profound loss of motion that severely limits the patient's ability to perform activities of daily living (ADLs), feed themselves, or perform personal hygiene. Pain is a variable symptom; some patients experience severe neuropathic or mechanical pain, while others present with a painless, albeit useless, stiff extremity.
Contraindications to joint-preserving open reduction include advanced patient age with low functional demands, severe medical comorbidities precluding prolonged general anesthesia, and the presence of active or recent intra-articular infection. A critical local contraindication is the presence of a non-functional upper extremity, such as in cases of severe, irreversible brachial plexus palsy, where restoring elbow motion would not yield functional improvement. Furthermore, if intraoperative assessment reveals complete destruction of the articular cartilage (grade IV chondromalacia across both the trochlea and capitellum), attempting a simple open reduction will inevitably result in a painful, stiff, arthritic joint, necessitating immediate conversion to an arthroplasty or arthrodesis.
Surgical Modalities and Patient Selection Matrix
| Clinical Scenario / Pathology | Primary Surgical Indication | Relative/Absolute Contraindications | Expected Functional Outcome |
|---|---|---|---|
| Young/Active, < 3-6 months dislocated, viable cartilage | Open Reduction with V-Y Triceps Lengthening (Speed Technique) | Severe cartilage destruction, active infection, non-compliant patient | Functional ROM (30°-130°), high risk of mild residual stiffness |
| Young/Active, > 6 months dislocated, severe cartilage loss | Distraction Interpositional Arthroplasty (Fascia Lata/Achilles) | Lack of adequate bone stock, profound ligamentous deficiency | Pain relief, moderate ROM, requires hinged external fixator |
| Elderly/Low-Demand, severe chronicity, osteopenic bone | Total Elbow Arthroplasty (TEA) - Semiconstrained | High-demand manual laborer, active infection, profound triceps deficiency | Excellent pain relief and ROM, lifetime lifting restrictions (< 5-10 lbs) |
| Pediatric (< 12 years), chronic anterior radial head dislocation | Joint Preservation: Bell Tawse Procedure (Ligament reconstruction + Ulnar osteotomy) | Skeletal maturity (relative), asymptomatic patient | Restoration of radiocapitellar kinematics, prevention of cubitus valgus |
| Adult, chronic isolated anterior radial head dislocation | Radial Head Excision | Growing child (Absolute contraindication - leads to Madelung deformity) | Relief of mechanical block to flexion, potential for mild instability |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative evaluation is paramount to anticipate and mitigate the severe intraoperative challenges associated with chronic elbow dislocations. Clinical assessment begins with a precise measurement of the current arc of motion, which is typically restricted to a few degrees of painful jog. The carrying angle is often grossly distorted into valgus or varus, and the prominent olecranon is easily palpable posteriorly. A meticulous neurological examination is mandatory and must be documented comprehensively. Particular attention must be paid to the ulnar nerve; signs of cubital tunnel syndrome, intrinsic muscle wasting, or sensory deficits in the ring and small fingers must be noted, as the nerve is frequently tethered, stretched, or encased in scar tissue.
Radiographic evaluation extends far beyond standard anteroposterior (AP) and lateral plain films. While plain radiographs confirm the direction of the dislocation (most commonly posterolateral) and reveal gross periarticular ossification, they are insufficient for operative planning. A non-contrast Computed Tomography (CT) scan with 3D reconstructions is an absolute requirement in chronic cases. The 3D CT precisely delineates the volume and spatial orientation of heterotopic ossification, particularly within the olecranon and coronoid fossae. It identifies occult osteochondral defects of the capitellum or radial head, assesses the degree of osseous remodeling, and is critical for preoperative templating if total elbow arthroplasty or the application of a hinged external fixator is anticipated.
Patient positioning and anesthesia require careful coordination. The procedure is performed under general anesthesia, almost universally supplemented with an indwelling regional brachial plexus block (supraclavicular or axillary) for prolonged postoperative pain control and to facilitate early rehabilitation. The patient is typically positioned in the lateral decubitus position. The operative arm is draped free over a well-padded L-bar or post, allowing for full, unobstructed flexion, extension, pronation, and supination of the elbow. A sterile pneumatic tourniquet is applied high on the arm to ensure a bloodless field, which is critical for the meticulous dissection of neurovascular structures embedded in scar tissue. Prophylactic intravenous antibiotics are administered prior to tourniquet inflation.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of chronic unreduced elbow dislocations relies heavily on the principles established by J.S. Speed. The "Speed Technique" remains the gold standard for addressing the severe triceps contracture and joint obliteration. The procedure demands an extensile exposure, meticulous handling of the fragile, nutrient-deprived articular surfaces, and a systematic approach to soft tissue balancing.
1. Incision and Ulnar Nerve Isolation
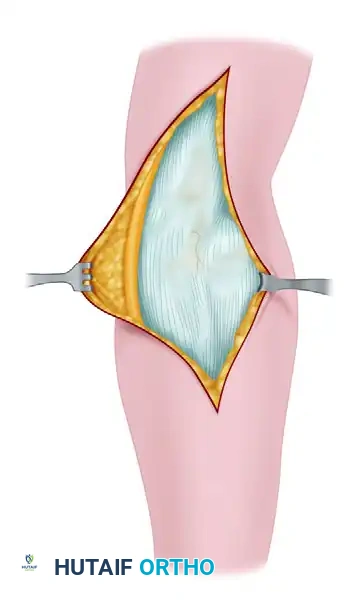
A generous posterior midline incision is utilized. The incision begins approximately 10 cm proximal to the tip of the olecranon, courses distally, and curves slightly lateral to the olecranon tip to avoid placing the surgical scar directly over the bony prominence, which can cause painful hardware or bone prominence issues postoperatively. Full-thickness fasciocutaneous flaps are elevated medially and laterally to protect the cutaneous nerves and preserve the vascular supply to the skin.
The very first critical deep step is the identification, neurolysis, and protection of the ulnar nerve. Due to the altered osseous anatomy and dense perineural fibrosis, attempting to find the nerve directly at the epicondyle is hazardous. The nerve must be identified proximally in the normal, unscarred tissue of the posterior compartment along the medial border of the triceps. It is then meticulously traced distally into the cubital tunnel and through the two heads of the flexor carpi ulnaris. The nerve is completely mobilized, freed from all fascial bands (including the arcade of Struthers and Osborne's ligament), and protected with a vessel loop. Depending on the tension following joint reduction, a formal anterior subcutaneous or submuscular transposition is frequently required to prevent postoperative traction neuropathy.
2. Triceps Reflection and V-Y Preparation
To overcome the profound myostatic contracture of the triceps brachii, which physically prevents reduction, a formal V-Y lengthening is performed. An inverted "V" incision is made through the triceps aponeurosis. The apex of the "V" is positioned proximally at the musculotendinous junction, and the limbs extend distally to the medial and lateral borders of the olecranon. The triceps muscle belly is then incised longitudinally in line with the aponeurotic incision.
Using a combination of sharp scalpel dissection and blunt Cobb elevators, the triceps and adjacent musculature are stripped subperiosteally from the distal humerus. This stripping must be meticulous and stay strictly on the bone to avoid injuring the radial nerve laterally. This extensive elevation exposes the posterior aspect of the joint, the medial and lateral columns, and the completely obliterated olecranon fossa.
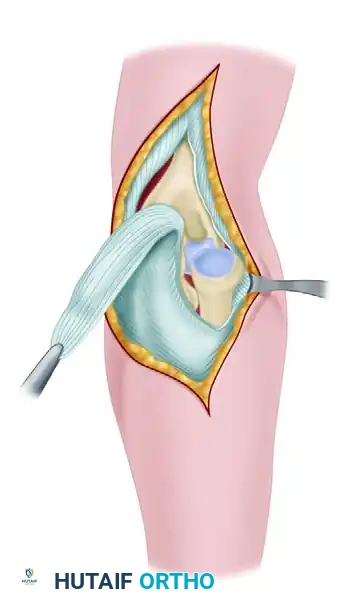
3. Joint Debridement and Extensive Mobilization
The surgeon will immediately encounter a massive volume of callus and heterotopic bone on the posterior surface of the humerus, completely filling the olecranon fossa. This is the direct result of the periosteum being stripped and elevated during the initial traumatic event. Using a combination of Leksell rongeurs, curettes, and a high-speed motorized burr, this callus and all intervening dense scar tissue must be meticulously excised. The olecranon fossa must be completely reconstituted to its native depth and width to accommodate the olecranon tip during terminal extension.
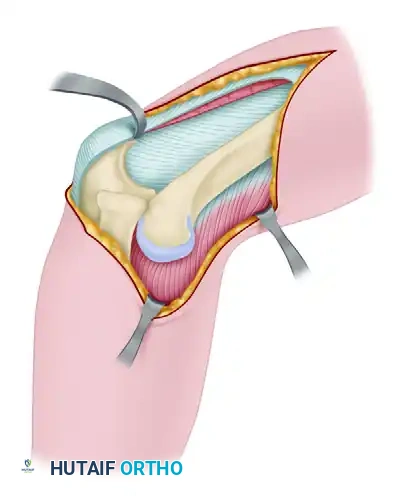
After completely freeing the distal humerus posteriorly and recreating the fossa, the dissection is carried anteriorly. The collateral ligaments are typically contracted and functionless, requiring subperiosteal release from the epicondyles. The anterior capsule, which is often severely contracted and adherent to the anterior humerus, must be elevated and released to expose the radial head and clear the trochlear notch of the ulna. The coronoid fossa must also be cleared of scar tissue to allow for full flexion.
4. The Reduction Maneuver
Reduction must be performed systematically and with extreme caution to avoid iatrogenic damage to the fragile articular cartilage or fractures of the osteopenic bone. Forceful levering is strictly prohibited.
- Radiocapitellar Reduction: The forearm is gently rotated, and direct thumb pressure is applied to the anterior surface of the capitellum while applying longitudinal traction. The radial head is levered anteriorly and distally into its normal anatomic position against the capitellum.
- Ulnohumeral Reduction: Once the radial head is reduced (which effectively restores the lateral column length and acts as a fulcrum), the coronoid process is slipped distally and then translated anteriorly over the trochlea.
If the radial head or ulna cannot be reduced easily, the surgeon must resist the temptation to apply excessive force. Instead, the soft tissues must be dissected more widely, the contracted anterior capsule released further, and more scar tissue cleared from the coronoid and olecranon fossae.
5. Joint Stabilization and Closure
Once reduced, the joint is carried through a full range of motion under direct visualization to assess stability and identify any bony or soft tissue impingement. Because the collateral ligaments are chronically attenuated, avulsed, or deliberately released during the approach, the elbow is usually grossly unstable. To maintain the reduction and allow for soft tissue healing, the olecranon is transfixed to the distal humerus. The elbow is held at exactly 90 degrees of flexion, and one or two heavy Steinmann pins or thick Kirschner wires are driven percutaneously through the olecranon into the anterior cortex of the distal humerus. The pins are cut short, and the proximal portions are bent to prevent intra-articular migration. Alternatively, a hinged external fixator may be applied if ligamentous reconstruction is performed and early motion is desired.
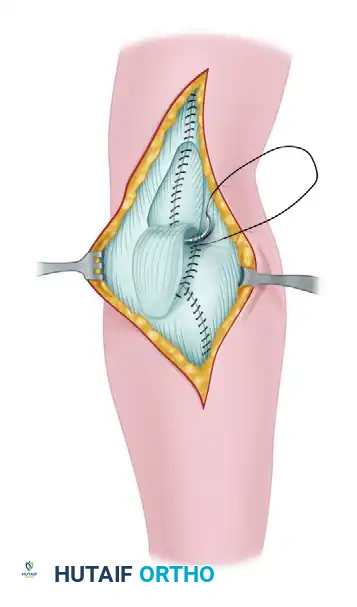
The periosteum and the deep triceps muscle belly are sutured over the posterior surface of the humerus. Finally, the V-Y lengthening is completed. The tongue of the triceps aponeurosis (the inverted "V") is advanced to a slightly more distal level to accommodate the new length of the reduced elbow without placing excessive tension on the repair. It is sutured to the medial and lateral fascial expansions using heavy, non-absorbable sutures.
A deep subfascial suction drain is placed to prevent hematoma formation, which is a potent stimulus for recurrent heterotopic ossification. The subcutaneous tissues and skin are closed in layers, and the limb is placed in a well-padded posterior splint.
Complications, Incidence Rates, and Salvage Management
The surgical treatment of chronic unreduced elbow dislocations is fraught with high complication rates, reflecting the severity of the underlying pathoanatomy. Surgeons must thoroughly counsel patients preoperatively regarding these risks and maintain a low threshold for utilizing salvage procedures.
The most ubiquitous complication is recurrent stiffness and loss of terminal extension. Despite flawless surgical execution, the immense soft tissue trauma and intrinsic propensity for fibrosis in the elbow joint frequently result in a functional arc of motion (e.g., 30 degrees to 130 degrees) rather than full anatomic motion. Heterotopic ossification (HO) is another major concern, occurring in up to 30-40% of cases despite meticulous surgical technique. Prophylactic measures, including a single dose of localized radiation therapy (700 cGy) within 24 hours postoperatively or a course of oral Indomethacin, should be considered in high-risk patients.
Ulnar neuropathy can occur due to intraoperative traction, delayed perineural fibrosis, or subluxation of the nerve if not properly transposed. Iatrogenic fractures of the distal humerus or olecranon are catastrophic complications that occur when excessive force is used during the reduction maneuver against a contracted triceps or unrecognized bony block.
Complications and Salvage Management Strategies
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Recurrent Stiffness / Arthrofibrosis | 40 - 60% | Inadequate release, prolonged immobilization, patient non-compliance | Aggressive static progressive splinting; late open or arthroscopic capsular release. |
| Heterotopic Ossification (HO) | 20 - 40% | Severe initial trauma, hematoma, delayed surgery, aggressive passive stretching | Prophylactic Indomethacin/Radiation; delayed surgical excision (after 6 months when mature). |
| Ulnar Neuropathy | 10 - 25% | Traction during reduction, inadequate neurolysis, perineural scarring | Revision neurolysis and submuscular anterior transposition. |
| Recurrent Instability / Subluxation | 10 - 15% | Failure to address collateral ligament deficiency, premature pin removal | Application of hinged external fixator; formal LUCL/MCL reconstruction with autograft. |
| Severe Articular Degeneration | Variable (Time-dependent) | Chondrocyte apoptosis from chronicity, abnormal mechanical loading | Distraction interpositional arthroplasty (young) or Total Elbow Arthroplasty (elderly). |
For patients who develop severe, painful articular degeneration or those who present with joints too destroyed for primary reduction, salvage procedures are indicated. Distraction interpositional arthroplasty involves reshaping the articular surfaces and interposing a biologic graft (autogenous fascia lata or Achilles tendon allograft) between the humerus and ulna, protected by a hinged external fixator. In elderly, low-demand patients, primary semiconstrained Total Elbow Arthroplasty (TEA) reliably restores motion and stability, though surgeons must be vigilant regarding the risk of premature polyethylene wear and aseptic loosening due to altered soft-tissue mechanics.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation of a chronic elbow dislocation is a highly delicate, protracted balance between protecting the tenuous osseous stability and preventing recurrent arthrofibrosis. The protocol must be strictly adhered to and closely monitored by both the operative surgeon and a specialized upper extremity physical therapist.
Phase I: Immediate Postoperative and Immobilization (Days 0-14)
Immediately following surgery, the arm is immobilized in a bulky, well-padded posterior splint with the elbow rigidly held at 90 degrees of flexion and the forearm in neutral rotation. The suction drain is typically removed after 24 to 48 hours once output decreases. The primary goals during this phase are wound healing, edema control, and pain management. Active range of motion of the digits and shoulder is encouraged immediately to prevent dependent edema and complex regional pain syndrome (CRPS).
Phase II: Pin Removal and Early Mobilization (Weeks 2-6)
Approximately 14 days postoperatively, the patient returns to the clinic for suture removal and extraction of the transarticular Steinmann pins. This is a critical transition point. Once the pins are removed, the static splint is transitioned to a custom-molded thermoplastic splint or a hinged elbow brace. The splint is removed several times a day for gentle, active, and active-assisted range of motion exercises in both flexion-extension and pronation-supination.
Clinical Pearl: Passive stretching by the therapist or patient is strictly and absolutely avoided during this phase. Forceful passive manipulation induces microtrauma, exacerbates the inflammatory cascade, promotes heterotopic ossification, and risks iatrogenic subluxation of the newly reduced joint. Motion must be driven by the patient's own musculature.
Phase III: Long-Term Maintenance and Strengthening (Months 2-6)
By the 6-to-8-week mark, if clinical and radiographic stability is maintained, the daytime splint may be gradually discarded to encourage functional use of the extremity in light ADLs. However, a static progressive or dynamic extension splint should be worn at night for an additional 3 to 6 months. The elbow joint is notoriously prone to losing terminal extension, and nocturnal splinting is the most effective method to combat this insidious contracture. Strengthening exercises for the triceps, biceps, and forearm musculature are initiated progressively.
If the dislocation has been present for an extended period prior to surgery, the best functional results are obtained only by continuing disciplined, daily exercises for up to a year. It is noteworthy that pediatric patients possess a vastly superior capacity for biological remodeling and typically regain a functional arc of motion more easily and completely than adults, provided the reduction is concentric and stable.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for unreduced elbow dislocations is grounded in several landmark contributions to orthopedic literature. J.S. Speed's original description of the V-Y triceps lengthening remains the cornerstone technique for overcoming the massive soft tissue contractures that define this pathology. His insistence on extensile exposure and meticulous joint clearance set the standard for joint preservation.
Morrey and colleagues at the Mayo Clinic revolutionized the understanding of elbow biomechanics, defining the primary and secondary stabilizers of the joint. Their work laid the foundation for recognizing the necessity of addressing the collateral ligament complexes during reduction. Furthermore, Morrey, Tan et al., and Lyons and Armstrong pioneered the use of distraction interpositional arthroplasty. Their studies demonstrated that interposing a biologic graft (such as fascia lata) combined with a hinged external fixator provides a viable salvage option for young, active patients with destroyed articular cartilage, delaying the need for total joint replacement.
In the realm of arthroplasty, Mighell et al. provided critical outcome data on the use of semiconstrained Total Elbow Arthroplasty for chronic dislocations in the elderly. Their series (average 17 weeks dislocated) confirmed that TEA reliably restores motion and provides excellent pain relief, though they cautioned against its use in high-demand patients due to the risk of catastrophic implant failure.
Finally, the management of pediatric chronic radial head dislocations is dictated by the principles established by Bell Tawse. Hasler et al. further refined these indications, reporting highly satisfactory results using a combination of open reduction, annular ligament reconstruction (using a triceps slip), and ulnar osteotomy to correct the bowing of the ulna and tension the interosseous membrane. The literature unequivocally supports the clinical guideline that radial head excision is strictly contraindicated in the growing child, as it invariably leads to proximal migration of the radius, severe cubitus valgus, distal radioulnar joint (DRUJ) disruption, and a debilitating acquired Madelung-like deformity.
