
Introduction and Epidemiology
Elbow dislocations represent a significant proportion of acute orthopedic trauma, accounting for 11% to 28% of all elbow injuries. The elbow is the second most commonly dislocated major joint in adults, following the glenohumeral joint, and the most commonly dislocated joint in the pediatric population. The annual incidence of elbow dislocations is estimated at 6 to 8 cases per 100,000 population per year. The highest incidence is observed in the 10- to 20-year-old age cohort, predominantly associated with high-energy sports injuries, gymnastics, and athletic falls. Unlike glenohumeral dislocations, recurrent dislocation of the elbow is relatively uncommon due to the high intrinsic osseous stability of the ulnohumeral articulation.
Elbow dislocations are broadly classified into two distinct categories based on the presence or absence of associated periarticular fractures. Simple dislocations are purely capsuloligamentous injuries without associated fractures. Complex dislocations, representing slightly less than 50% of all elbow dislocations, occur in conjunction with fractures of the surrounding osseous structures, most notably the radial head, the coronoid process, and the olecranon. The "terrible triad" of the elbow—characterized by a posterior dislocation, a radial head fracture, and a coronoid fracture—is a classic example of a complex dislocation that presents significant challenges regarding joint stability and functional recovery.
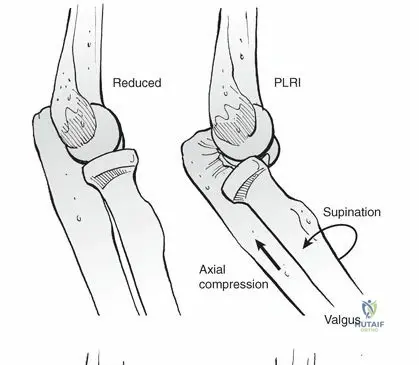
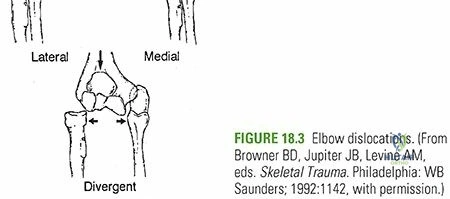
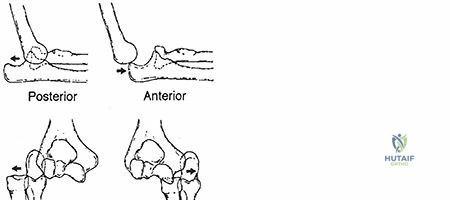
Directionally, posterior dislocations are by far the most common, accounting for 80% to 90% of all elbow dislocations. The mechanism of injury typically involves a fall onto an outstretched hand (FOOSH). This generates a complex combination of forces: axial loading, supination, and valgus stress. This levering force effectively unlocks the olecranon from the trochlea, combined with the translation of the articular surfaces, producing the dislocation. Posterior dislocations specifically result from a combination of elbow hyperextension, valgus stress, arm abduction, and forearm supination. Conversely, anterior dislocations are exceedingly rare and typically result from a direct traumatic force striking the posterior aspect of the forearm while the elbow is in a flexed position, driving the olecranon anteriorly relative to the distal humerus.

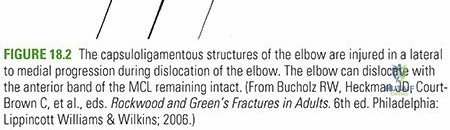
Most elbow dislocations and fracture-dislocations result in predictable, sequential injury to the capsuloligamentous stabilizers of the elbow joint. The notable exceptions to this pattern include transolecranon fracture-dislocations and complex injuries involving fractures of the coronoid that encompass nearly the entire coronoid process, where the osseous failure precedes or precludes complete ligamentous disruption.
Surgical Anatomy and Biomechanics
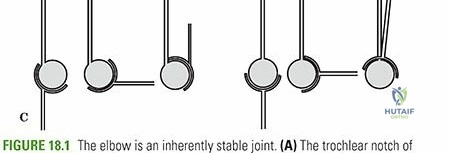
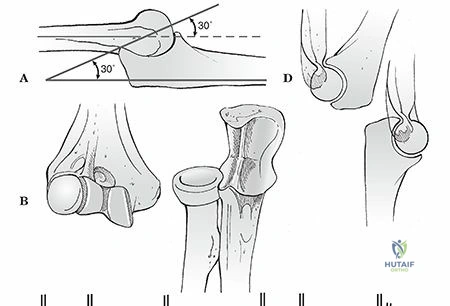
The elbow is a highly constrained "modified hinge" (ginglymus) joint that exhibits a high degree of intrinsic stability. This stability is multifactorial, owing to the precise congruity of the articular surfaces, the dynamic opposing tension of the triceps and flexor-pronator muscle masses, and the robust static ligamentous constraints.
The joint comprises three separate but biomechanically linked articulations:
1. The ulnotrochlear joint, which functions as a primary hinge allowing flexion and extension.
2. The radiocapitellar joint, which facilitates forearm rotation and provides secondary valgus and longitudinal stability.
3. The proximal radioulnar joint, which works in concert with the distal radioulnar joint to allow pronation and supination.
Primary and Secondary Stabilizers
Stability of the elbow is dictated by primary and secondary restraints across multiple planes of motion.
In the anterior-posterior plane, stability in extension is primarily governed by the interlocking of the trochlea and the olecranon fossa. In flexion, stability relies on the coronoid process articulating with the coronoid fossa, the radiocapitellar joint, and the dynamic anterior tension provided by the biceps and brachialis muscles, counterbalanced by the triceps posteriorly. The anterior joint capsule is also recognized as a critical structure in maintaining ulnohumeral stability, particularly in extension.
Valgus stability is primarily controlled by the medial collateral ligament (MCL) complex. The anterior bundle of the MCL (AMCL) is the primary static stabilizer against valgus stress in both flexion and extension. The AMCL originates from the anterior inferior aspect of the medial epicondyle and inserts onto the sublime tubercle of the coronoid. Full extension relies on the anterior capsule and the radiocapitellar joint for approximately 30% of valgus stability, whereas at 90 degrees of flexion, the AMCL provides greater than 50% of the resistance to valgus forces. Resection or incompetent healing of the anterior band will cause gross valgus instability in all positions except full extension.
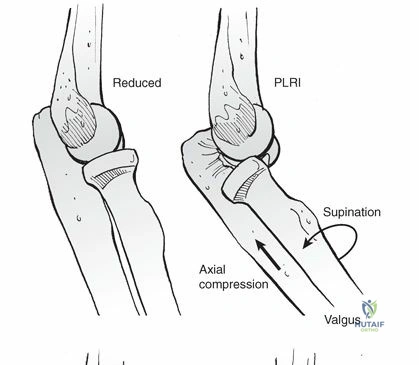
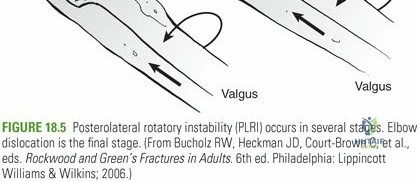
Varus stability and resistance to posterolateral rotatory forces are governed by the lateral collateral ligament (LCL) complex. The lateral ulnar collateral ligament (LUCL) is the primary static restraint, originating from the lateral epicondyle and inserting on the supinator crest of the ulna. The anconeus muscle serves as a critical dynamic stabilizer against varus and posterolateral rotatory forces. The lateral ligaments collectively prevent posterior subluxation and rotation of the ulna away from the humerus during forearm supination, a condition clinically recognized as posterolateral rotatory instability (PLRI).
The Hori Circle Concept
The capsuloligamentous injury in a typical posterior elbow dislocation progresses in a predictable lateral-to-medial sequence, fundamentally described by O'Driscoll as the Hori circle.
* Stage 1 involves disruption of the LCL complex, resulting in PLRI.
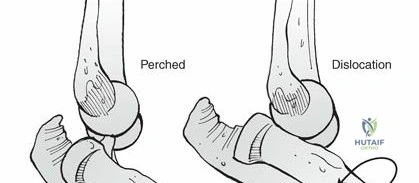
* Stage 2 involves further energy propagation causing disruption of the anterior and posterior joint capsules, leading to perched articular surfaces.
* Stage 3 involves disruption of the MCL complex. Stage 3A involves the posterior band of the MCL, while Stage 3B involves complete disruption of the anterior band of the MCL, resulting in a frank, highly unstable posterior dislocation.
Kinematics and Range of Motion
The normal anatomical range of motion (ROM) of the elbow encompasses 0 to 150 degrees of flexion, 85 degrees of supination, and 80 degrees of pronation. Historically, the functional ROM required for basic activities of daily living (ADLs) was defined by Morrey as a 100-degree arc comprising 30 to 130 degrees of flexion, 50 degrees of supination, and 50 degrees of pronation. However, more recent kinematic analyses suggest that an increased ROM is necessary to perform contemporary ADLs, such as utilizing modern communication devices, typing on keyboards, and operating a computer mouse. Restoration of this expanded functional arc is the primary goal of both conservative and operative management.
Indications and Contraindications
The management of elbow dislocations is dictated by the complexity of the injury, the presence of associated fractures, and the stability of the joint following closed reduction. The overarching goal is to achieve a concentric, stable reduction that permits early active range of motion to prevent debilitating post-traumatic stiffness.
Simple dislocations are predominantly managed non-operatively. Following a successful closed reduction, the elbow is assessed for stability through a full range of motion. If the elbow remains concentrically reduced and stable through a functional arc (typically from full flexion to approximately 30 degrees of extension), non-operative management with brief immobilization followed by early active motion is indicated.
Operative intervention is strictly indicated for complex dislocations, such as the terrible triad, transolecranon fracture-dislocations, and Monteggia variants. Furthermore, simple dislocations that remain grossly unstable following reduction, requiring immobilization in greater than 45 to 60 degrees of flexion to maintain congruity, or those associated with acute vascular compromise, necessitate surgical exploration and stabilization.
| Clinical Scenario | Management Strategy | Rationale and Considerations |
|---|---|---|
| Simple Dislocation Stable Post Reduction | Non Operative | Brief immobilization (3-7 days) followed by early active ROM. Excellent long-term outcomes. |
| Simple Dislocation Unstable Post Reduction | Operative | Ligamentous repair (LCL, occasionally MCL) required if concentric reduction cannot be maintained in <45 degrees of flexion. |
| Terrible Triad Fracture Dislocation | Operative | Requires systematic repair: coronoid fixation, radial head repair/arthroplasty, and LCL repair to restore stability. |
| Transolecranon Fracture Dislocation | Operative | Restoration of the greater sigmoid notch is mandatory. Typically requires rigid plate osteosynthesis. |
| Open Dislocation or Vascular Compromise | Operative | Surgical emergency. Requires immediate debridement, reduction, vascular repair, and skeletal stabilization. |
Contraindications to surgical intervention are primarily systemic. Patients with severe medical comorbidities precluding anesthesia, or those with non-ambulatory status and minimal functional demands, may be managed non-operatively even in the setting of complex instability, accepting a chronically subluxated or stiff elbow. Active local soft tissue infection is an absolute contraindication to internal fixation until the infection is eradicated.
Pre Operative Planning and Patient Positioning
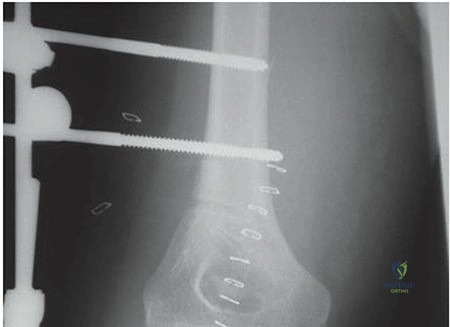
Thorough preoperative planning is paramount for the successful surgical management of complex elbow dislocations. Standard orthogonal anteroposterior (AP) and lateral radiographs of the elbow are mandatory both before and immediately following closed reduction. The post-reduction lateral radiograph must be critically evaluated for concentric reduction of the ulnohumeral joint; even a subtle widening of the posterior ulnohumeral clear space indicates residual subluxation and instability.
For any complex dislocation or fracture-dislocation, a fine-cut computed tomography (CT) scan with 3D reconstructions is strongly recommended. The CT scan accurately delineates the size and comminution of the coronoid fracture, the morphology of the radial head fracture, and the presence of any intra-articular osteochondral shear fragments that might impede anatomical reduction.

Patient Positioning Considerations
Patient positioning must allow unhindered access to both the medial and lateral aspects of the elbow, as well as the ability to utilize intraoperative fluoroscopy.
- Supine Position: The patient is placed supine with the operative arm resting on a radiolucent hand table. This is optimal for isolated lateral or medial approaches and allows excellent access for anterior coronoid fixation. A sterile tourniquet is applied high on the brachium.
- Lateral Decubitus Position: The patient is placed in the lateral decubitus position with the operative arm draped over a well-padded post (e.g., a Leksell arm holder). This position provides excellent access to the posterior, lateral, and medial aspects of the elbow and is highly preferred for complex fracture-dislocations requiring a universal posterior approach. It also utilizes gravity to assist with ulnohumeral reduction during the procedure.
Appropriate equipment must be available, including small and mini-fragment plates, radial head arthroplasty systems, suture anchors for ligamentous repair, and an articulated external fixator in cases where severe osseous comminution precludes stable internal fixation.
Detailed Surgical Approach and Technique
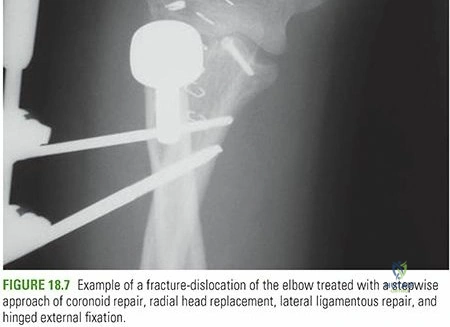
The surgical management of an unstable elbow dislocation, particularly a complex fracture-dislocation like the terrible triad, follows a systematic, stepwise algorithm aimed at sequentially restoring the osseous and ligamentous stabilizers from deep to superficial.

Surgical Approaches
The universal posterior approach is the workhorse incision for complex elbow trauma. A longitudinal incision is made slightly lateral to the tip of the olecranon to avoid placing the scar directly over the bony prominence. Full-thickness fasciocutaneous flaps are elevated medially and laterally to access both columns of the distal humerus.
From the lateral window, two deep internervous planes can be utilized:
1. The Kocher Approach: Utilizes the interval between the anconeus (radial nerve) and the extensor carpi ulnaris (posterior interosseous nerve). This provides excellent exposure of the radial head and the lateral ulnohumeral joint but poses a theoretical risk to the LUCL if not carefully identified.
2. The Kaplan Approach: Utilizes the interval between the extensor digitorum communis (posterior interosseous nerve) and the extensor carpi radialis brevis (radial nerve). This approach provides a more anterior view of the radiocapitellar joint and the coronoid process.
From the medial window, an "over-the-top" approach can be utilized to address the coronoid or the MCL. The ulnar nerve must be identified, mobilized, and protected throughout the procedure. Routine anterior transposition is not mandatory unless the nerve is under tension or heavily manipulated during fixation.
Stepwise Reconstruction Technique
The surgical sequence typically proceeds from deep to superficial, addressing the coronoid, then the radial head, and finally the lateral ligamentous complex.
Coronoid Fixation
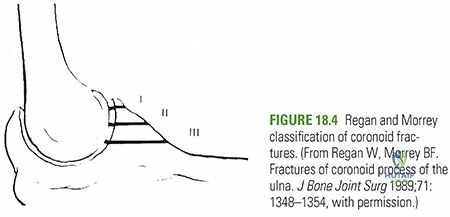
The coronoid process is the keystone of anterior ulnohumeral stability. Type I fractures (tip avulsions) are often capsular avulsions. If the fragment is small, it can be secured using a suture lasso technique. Heavy non-absorbable sutures are passed through the anterior capsule and the coronoid fragment, then passed through drill holes exiting the posterior cortex of the ulna and tied over a bony bridge. Type II and III fractures (anteromedial facet or basal fractures) require rigid internal fixation using mini-fragment screws or specialized coronoid plates applied via a medial or anteromedial approach.

Radial Head Management
Once the coronoid is addressed, the radial head is evaluated. If the fracture consists of fewer than three large fragments without significant impaction, open reduction and internal fixation (ORIF) with headless compression screws or a low-profile plate applied to the "safe zone" (the non-articulating portion of the radial head) is performed. If the radial head is highly comminuted (Mason Type III), radial head arthroplasty is indicated. Excision of the radial head without replacement in the setting of ligamentous instability is strictly contraindicated, as it will lead to immediate proximal radial migration and profound valgus and posterolateral instability.
Lateral Collateral Ligament Repair
The LUCL is almost universally avulsed from its origin on the lateral epicondyle. Repair is achieved using suture anchors or transosseous tunnels. The isometric point on the lateral epicondyle—located at the center of capitellar curvature—must be precisely identified. The arm is placed in 90 degrees of flexion and maximum pronation to reduce the ulnohumeral joint, and the heavy non-absorbable sutures are tied, securing the LCL complex back to its anatomic footprint.
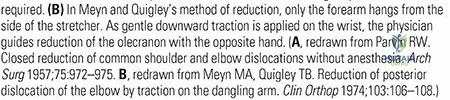
Assessment of Stability and Medial Sided Repair
Following LCL repair, the elbow is taken through a full range of motion. The "hanging arm test" can be employed to assess for residual subluxation. If the elbow remains concentrically reduced from full flexion to 30 degrees of extension, the procedure is concluded. If the elbow subluxates in extension, the MCL complex must be evaluated. While historically routine, MCL repair is now reserved for cases of persistent instability following adequate anterior, lateral, and radial column reconstruction. If required, the AMCL is repaired to the medial epicondyle using suture anchors.
In the rare event that the elbow remains grossly unstable despite comprehensive osseous and ligamentous reconstruction, an articulated dynamic external fixator is applied to maintain concentric reduction while allowing early motion.
Complications and Management
Complications following elbow dislocations and fracture-dislocations are frequent and can significantly impair upper extremity function. The high intrinsic congruity of the joint makes it particularly susceptible to stiffness and heterotopic ossification.
Post-traumatic stiffness is the most common complication. The elbow capsule is highly reactive to trauma and hemorrhage, rapidly undergoing fibrotic contracture. Prevention relies on achieving stable fixation that permits early active ROM. If profound stiffness persists beyond 6 months despite aggressive physical therapy, operative intervention via an open or arthroscopic capsular release (column procedure) may be indicated.
Heterotopic ossification (HO) frequently occurs in the surrounding musculature or capsule, particularly following delayed surgical intervention or severe head trauma. Prophylaxis with indomethacin or single-fraction localized radiation therapy is considered in high-risk patients. Excision of HO should be delayed until the bone is metabolically mature, typically indicated by sharp cortical margins on radiographs and normalized serum alkaline phosphatase levels.
| Complication | Incidence | Pathophysiology and Salvage Strategy |
|---|---|---|
| Post-Traumatic Stiffness | High (30-50%) | Capsular fibrosis and contracture. Salvage: Arthroscopic or open capsulectomy (column procedure) after 6 months of failed conservative therapy. |
| Heterotopic Ossification | Moderate (10-20%) | Aberrant bone formation in soft tissues. Salvage: Surgical excision once metabolically mature, combined with immediate postoperative radiation or NSAIDs. |
| Recurrent Instability (PLRI) | Low (<5%) | Failure of LUCL healing or unrecognized injury. Salvage: LUCL reconstruction utilizing palmaris longus or triceps autograft. |
| Ulnar Neuropathy | Moderate (10-15%) | Traction injury during dislocation or iatrogenic during medial approach. Salvage: Ulnar nerve neurolysis and anterior transposition. |
| Post-Traumatic Arthrosis | High (long term) | Chondral shear injury at the time of dislocation. Salvage: Interposition arthroplasty (young patients) or Total Elbow Arthroplasty (elderly/low demand). |
Post Operative Rehabilitation Protocols
The paramount objective of the postoperative rehabilitation protocol is to balance the protection of repairing osseous and ligamentous structures with the absolute necessity of early mobilization to prevent capsular contracture. Prolonged immobilization beyond 2 to 3 weeks is strictly avoided, as it exponentially increases the risk of permanent functional impairment.
In the immediate postoperative phase (Days 1-7), the elbow is typically immobilized in a well-padded posterior splint at 90 degrees of flexion with the forearm in neutral to slight pronation. Pronation inherently tightens the medial soft tissue structures and provides a buttress against posterolateral subluxation, thereby protecting the lateral collateral ligament repair.
Phase II (Weeks 1-6) initiates active and active-assisted range of motion. An extension block splint may be utilized if there is concern regarding terminal extension stability. The block is typically set at 30 degrees of extension and is gradually reduced by 10 degrees each week. During this phase, it is critical to avoid shoulder abduction combined with internal rotation, as this creates a significant varus gravitational moment across the elbow, placing deleterious stress on the healing LUCL. Passive stretching is strictly prohibited, as it exacerbates inflammation, promotes capsular fibrosis, and increases the risk of heterotopic ossification.
Phase III (Weeks 6-12) focuses on weaning all splinting and initiating progressive strengthening of the dynamic stabilizers, particularly the triceps, brachialis, and flexor-pronator mass. Full functional return to heavy labor or high-impact athletics is generally delayed until 4 to 6 months post-injury, contingent upon the complete restoration of stability and radiographic union of all associated fractures.
Summary of Key Literature and Guidelines
The modern academic understanding and surgical management of elbow dislocations are heavily predicated on landmark biomechanical and clinical studies.
The foundational concept of elbow stability was revolutionized by O'Driscoll et al., who elucidated the mechanism of posterolateral rotatory instability (PLRI) and defined the Hori circle of sequential capsuloligamentous disruption. Their work established the LUCL as the primary restraint to varus and external rotatory stress, shifting the surgical paradigm toward anatomical lateral-sided reconstruction.
Regarding complex fracture-dislocations, the work of Jupiter and Ring on the "terrible triad" of the elbow defined the modern treatment algorithm. Their retrospective analyses demonstrated that non-operative management or isolated radial head excision in the setting of a terrible triad injury universally leads to chronic instability and catastrophic arthrosis. They established the absolute necessity of a systematic surgical approach: repairing the coronoid, restoring the radial head (via ORIF or arthroplasty), and repairing the lateral ligamentous complex.
Current consensus guidelines from orthopedic trauma societies emphasize that for simple dislocations, early active mobilization is superior to prolonged casting. Immobilization should not exceed 14 days, and functional outcomes are maximized when patients initiate an active, gravity-assisted motion protocol immediately following a stable closed reduction. Surgical intervention for simple dislocations is strictly reserved for those rare instances where a concentric reduction cannot be maintained in a functional arc of motion.
Clinical & Radiographic Imaging
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding elbow-dislocation