Surgical Management of Old Unreduced Elbow Dislocations
Key Takeaway
Old unreduced posterior elbow dislocations present a profound reconstructive challenge characterized by severe soft-tissue contracture, myositis ossificans, and joint space obliteration. Successful management requires meticulous open reduction, extensive capsuloligamentous release, triceps lengthening, and ulnar nerve decompression. Postoperative stability is frequently augmented using a dynamic hinged external fixator to maintain concentric reduction while permitting early active range of motion, thereby optimizing functional outcomes and preventing recurrent stiffness.
Comprehensive Introduction and Patho-Epidemiology
Old unreduced dislocations of the elbow represent a formidable challenge in modern orthopedic surgery, characterized by profound anatomical distortion and severe functional impairment. While these neglected injuries are relatively rare in developed nations—largely due to the ubiquity of advanced cross-sectional imaging, routine radiographic screening, and immediate access to specialized emergency trauma care—they remain a highly significant and frequently encountered clinical entity in developing countries and rural, resource-stratified settings. In these environments, delayed presentations are often the result of initial misdiagnosis, reliance on traditional bone setters, or profound geographic and socioeconomic barriers to accessing definitive surgical care. Operative treatment for these neglected injuries has been extensively documented by surgeons practicing in the Near and Far East, where the chronicity of presentation necessitates highly specialized, salvage-oriented surgical algorithms.
Posterior and posterolateral dislocations constitute the vast majority of these chronic cases, mirroring the epidemiological distribution of acute elbow instability. Clinically, the patient presents with a profoundly stiff, virtually ankylosed elbow, generally fixed in extension or very slight flexion. The arc of motion is severely restricted, often limited to a non-functional jog of a few degrees. This position of extension is functionally devastating, as it prevents the patient from performing essential activities of daily living, such as feeding, personal hygiene, and dressing. The prolonged abnormal articulation leads to adaptive shortening of the entire flexor-extensor mechanism, effectively locking the joint in this non-functional posture.
In addition to the devastating loss of the flexion-extension arc, forearm rotation is profoundly compromised. Clinical examination typically reveals that pronation is significantly more limited than supination. This specific, reproducible rotational deficit occurs because the biceps brachii muscle and its distal tendon are placed under significant, unyielding tension as the tendon angulates acutely around the displaced, prominent anterior humeral condyles. This abnormal anatomical routing biomechanically tethers the forearm into a supinated posture, creating a rigid supinatory contracture that cannot be overcome by active or passive manipulation. The combination of a stiff, extended elbow and a supinated forearm renders the upper extremity virtually useless, mandating complex surgical intervention to restore a functional arc of motion.
Detailed Surgical Anatomy and Biomechanics
The chronicity of an unreduced elbow dislocation initiates a devastating cascade of severe soft-tissue contractures and osseous adaptations that render delayed closed reduction not only impossible but strictly contraindicated. The pathoanatomy is characterized by a complete obliteration of the normal functional spaces of the elbow joint, replaced by dense scar tissue, heterotopic bone, and contracted myofascial units. Open reduction in this setting is highly complex, requiring meticulous dissection through distorted tissue planes to safely mobilize the neurovascular structures and restore the concentric articulation of the ulnohumeral and radiocapitellar joints.
Silva extensively described the pathological findings associated with old unreduced elbow dislocations, establishing the foundational understanding of this complex pathoanatomy. The hallmark features include extensive myositis ossificans and rampant heterotopic bone formation around the joint. This ectopic ossification aggressively infiltrates the brachialis anteriorly and the triceps brachii muscle bellies posteriorly, essentially cementing the displaced articular surfaces in their abnormal positions. Concurrently, there is marked myotendinous contracture; the triceps muscle undergoes profound shortening and fibrosis, while the medial and lateral collateral ligamentous complexes become rigidly contracted, losing all elastic properties.
Neurological tethering is a critical and highly dangerous component of this pathoanatomy. The ulnar nerve, normally gliding freely within the cubital tunnel, becomes completely encased in dense, unyielding perineural scar tissue. Because the nerve is tethered behind the medially displaced medial epicondyle, any attempt at elbow flexion places the nerve under severe, acute traction, risking catastrophic iatrogenic traction neuritis or frank structural failure. Furthermore, the joint capsule undergoes dense fibrous thickening or frank ossification, completely obliterating the normal capsular recesses. Extensive, dense fibrous tissue completely fills the olecranon and coronoid fossae, as well as the anatomical space between the distal humerus and the proximal radius and ulna, physically blocking any attempt at reduction until meticulously debrided.
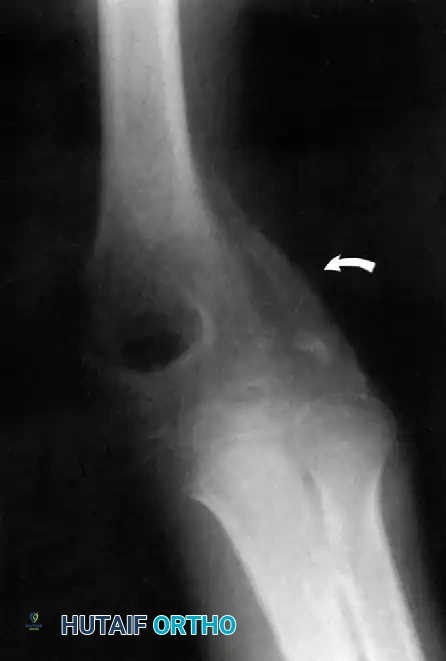
Furthermore, Allende and Freytes identified a pathognomonic radiographic and anatomical feature known as the "radial humeral horn," which was present in 100% of their 35 reported cases. This "horn" is the direct result of the ossification of a massive fracture hematoma trapped between the stripped periosteum and the anterior joint capsule near the radial head. Recognizing this structure preoperatively is absolutely critical, as it acts as a rigid, bony mechanical block to reduction. It must be surgically identified, isolated, and completely excised at its base to allow the radial head to glide back into its native articulation with the capitellum.
Exhaustive Indications and Contraindications
The surgical management of an old unreduced elbow dislocation is dictated by the chronicity of the injury, the patient's physiological age, functional demands, and the integrity of the articular cartilage. The treatment options exist on a spectrum ranging from complex open reduction with dynamic stabilization to definitive salvage procedures such as interposition arthroplasty, total elbow arthroplasty (TEA), or arthrodesis.
Most authorities agree that closed reduction of the elbow is virtually impossible—and strictly contraindicated—after 3 weeks from the initial injury. By this timeline, profound soft-tissue contracture and localized periarticular osteoporosis have developed. Attempting forceful closed manipulation is highly hazardous; the extreme leverage required to overcome the fibrotic tethering frequently results in catastrophic iatrogenic fractures of the osteopenic distal humerus, or severe, irreversible shearing damage to the remaining articular cartilage. Even during the early subacute period (1 to 3 weeks), manipulation must be performed with extreme caution under general anesthesia with complete neuromuscular blockade to ensure absolute muscle relaxation.
The likelihood of restoring useful, pain-free function through open reduction alone is inversely proportional to the length of time elapsed from injury to surgery. While historical series noted that adult patients with delays of 19 to 24 months fared better with fascial arthroplasty or excision arthroplasty, contemporary data suggest that meticulous open reduction, combined with hinged external fixation, can yield good to excellent results if performed within 3 to 6 months of injury. Interestingly, pediatric patients exhibit remarkable adaptive remodeling and chondral resilience. Fowles et al. emphasized that open reduction in children is always worth attempting, regardless of the delay. Children treated as late as 1 to 3 years post-injury have demonstrated the profound biological ability to regain functional arcs of motion following extensive open releases.
| Clinical Scenario / Chronicity | Primary Surgical Indication | Absolute Contraindications | Preferred Surgical Strategy |
|---|---|---|---|
| Subacute (1-3 Weeks) | Failure of initial closed reduction; functional block. | Severe medical comorbidities precluding anesthesia. | Careful closed reduction under anesthesia; Open reduction if closed fails. |
| Chronic Adult (3 Weeks - 3 Months) | Fixed extension posture; profound stiffness; intact cartilage on imaging. | Attempted closed reduction; active joint infection. | Extensile Open Reduction + V-Y Triceps Lengthening + Hinged Ex-Fix. |
| Neglected Adult (> 6-12 Months) | Severe articular degradation; extensive bridging heterotopic ossification. | High physical demand laborer (relative contraindication for TEA). | Total Elbow Arthroplasty (TEA) or Interposition Arthroplasty (younger patients). |
| Pediatric Neglected (> 1 Year) | Any delayed presentation in a skeletally immature patient. | None, open reduction should always be attempted. | Open Reduction + Extensive Soft Tissue Release (remodeling expected). |
| Grossly Unstable / Paralytic | Concomitant severe brachial plexus injury; massive bone loss. | Active infection; viable reconstructive options available. | Elbow Arthrodesis (positioned at 90° flexion for optimal function). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful surgical outcome in neglected elbow dislocations. Standard orthogonal anteroposterior and lateral radiographs are mandatory but insufficient for complete surgical mapping. A fine-cut Computed Tomography (CT) scan with 3-dimensional surface-rendered reconstructions is absolutely critical. The CT scan accurately delineates the extent of heterotopic ossification, maps the precise location of the "radial humeral horn," and evaluates the structural integrity of the coronoid process and radial head. It allows the surgeon to conceptualize the exact areas of bony impingement that must be resected.
Magnetic Resonance Imaging (MRI) may be indicated if there is a documented preoperative ulnar or median neuropathy, allowing the surgeon to assess the degree of perineural fibrosis and plan for extensive neurolysis or transposition. Furthermore, preoperative templating is essential. The surgeon must template for a hinged elbow external fixator (such as the Compass hinge) to ensure appropriate pin sizing and placement. In older adults with suspected severe cartilage degradation, the surgeon must also template for a semi-constrained Total Elbow Arthroplasty and have the implants available in the operating room as a definitive salvage option if the joint is deemed unsalvageable upon direct inspection.
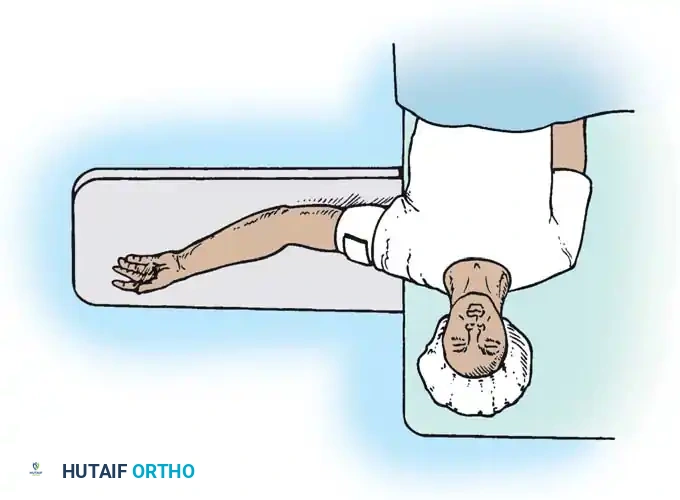
Patient positioning must allow for an extensile posterior approach, unhindered access to the medial and lateral columns of the distal humerus, and the ability to intraoperatively assess the full arc of flexion and extension. The patient is typically placed in the lateral decubitus position with the operative arm draped over a sterile padded bolster (the "over-the-top" position). Alternatively, the prone position with the arm resting on a radiolucent arm board can be utilized. A sterile pneumatic tourniquet is applied as high on the proximal arm as possible to maximize the surgical field. The entire upper extremity, from the fingertips to the axilla, is prepped and draped free to allow for dynamic intraoperative manipulation and precise fluoroscopic imaging.
Step-by-Step Surgical Approach and Fixation Technique
To achieve a successful open reduction, the surgeon must systematically address the pathoanatomy through a highly structured, stepwise approach. The Speed technique remains the gold standard for addressing the severe triceps contracture and global joint obliteration associated with neglected posterior dislocations.
Extensile Exposure and Ulnar Nerve Neurolysis
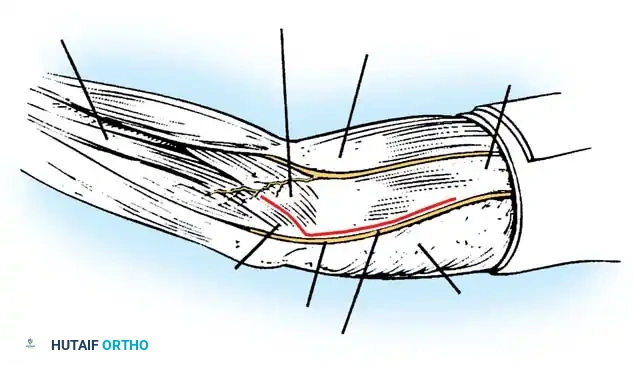
Make a generous, extensile posterior incision beginning in the midline approximately 10 to 12 cm proximal to the tip of the olecranon. Continue the incision distally to just proximal to the olecranon tip, curve it slightly laterally to avoid the tip itself and prevent painful scar formation, and extend it 5 to 7 cm distally onto the proximal forearm over the subcutaneous border of the ulna. Undermine and retract the full-thickness fasciocutaneous flaps to expose the tendinous insertion and broad aponeurosis of the triceps muscle.
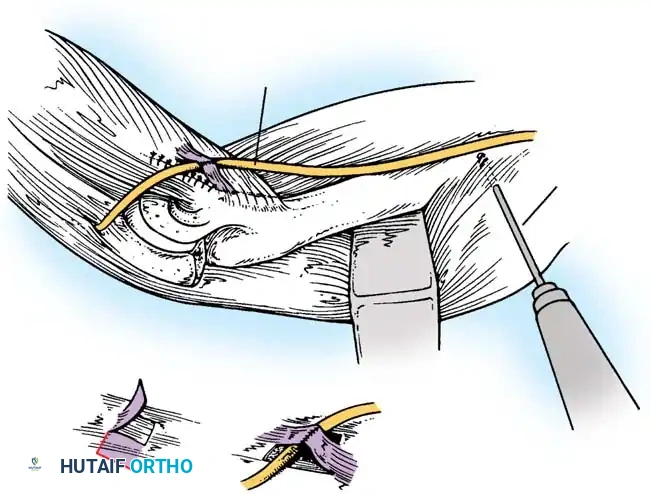
Before proceeding with any deep dissection or soft tissue release, the ulnar nerve must be definitively identified and protected. Locate the ulnar nerve proximally in the posterior compartment of the arm. Dissect it meticulously from its bed along the postcondylar groove of the medial epicondyle. The nerve is often encased in dense scar tissue and may be significantly flattened or hyperemic. Perform a thorough neurolysis, freeing the nerve from the arcade of Struthers proximally to the two heads of the flexor carpi ulnaris distally. Secure the nerve with a vessel loop to maintain absolute control throughout the procedure. Given the extensive subsequent mobilization of the joint, the ulnar nerve is frequently transposed anteriorly into a subcutaneous or subfascial bed to prevent traction neuritis during postoperative mobilization.
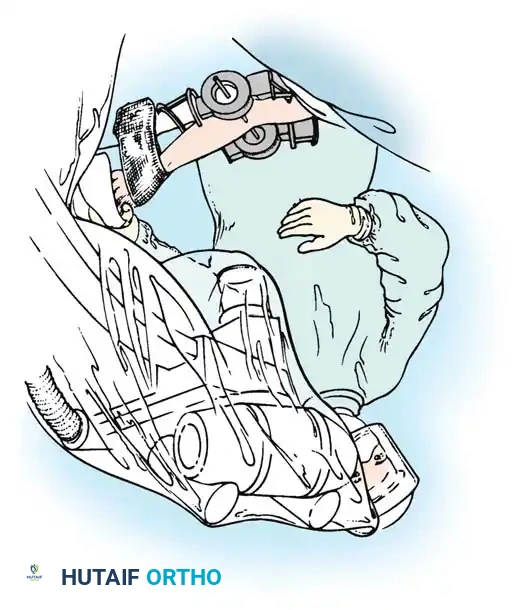
Triceps Flap and Subperiosteal Stripping
Beginning proximally, use sharp dissection to reflect the aponeurosis of the triceps distally, forming a robust, broad tongue-like flap of tissue that remains firmly attached to the olecranon. Starting approximately 7.5 cm proximal to the joint line, make a midline incision through the underlying, contracted muscle fibers of the triceps down to the posterior cortex of the humerus. Curve this deep incision around the lateral edge of the olecranon to preserve the continuity of the extensor mechanism.
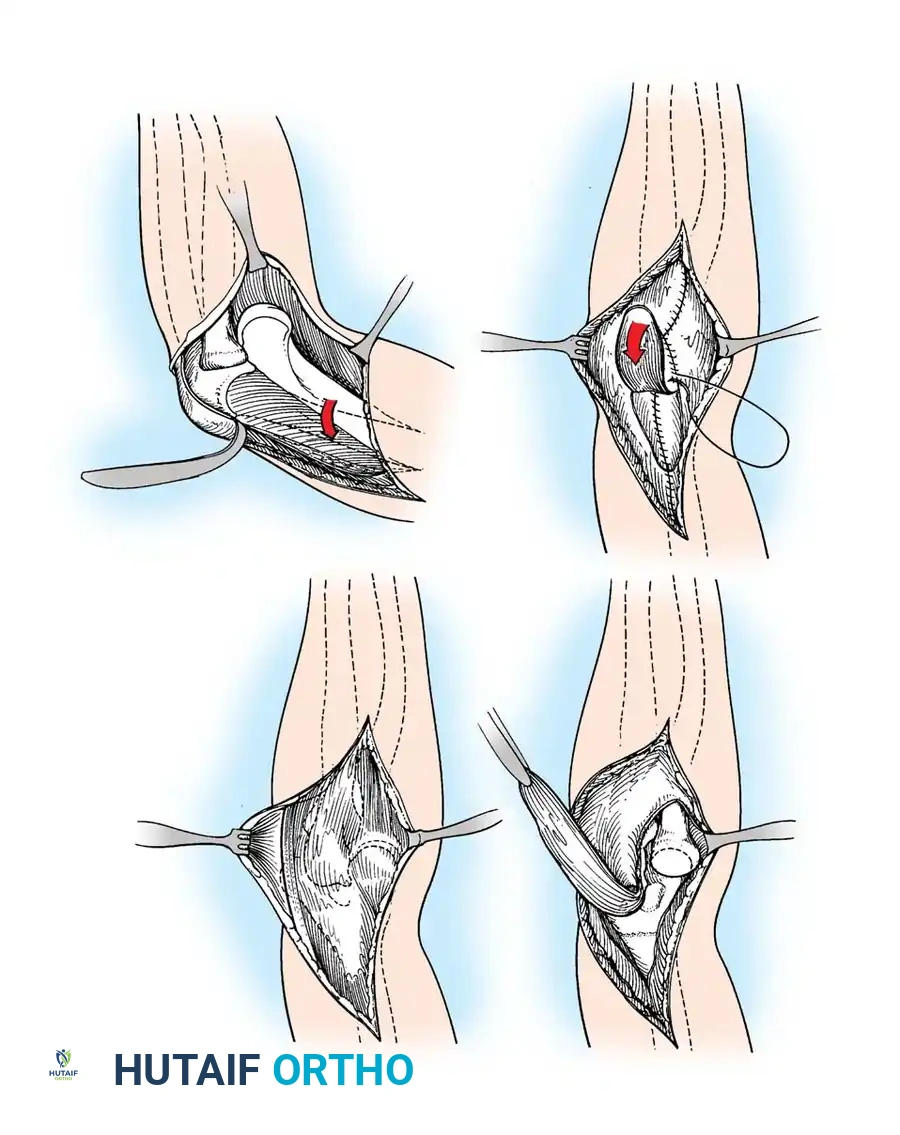
Utilize a Cobb elevator to subperiosteally free all muscle attachments from the distal humerus, moving systematically from posterior to anterior. Aggressive subperiosteal elevation is required to mobilize the distal humerus completely. Release the heavily scarred attachments of the joint capsule and the contracted medial and lateral collateral ligaments directly off the humeral epicondyles. Mobilizing the tissues around the medial condyle and anterior humerus can be exceptionally difficult due to dense fibrosis and heterotopic ossification, but complete, circumferential mobilization of the distal humerus is absolutely non-negotiable to achieve a tension-free reduction.
Joint Debridement, Excision of Ossification, and Reduction
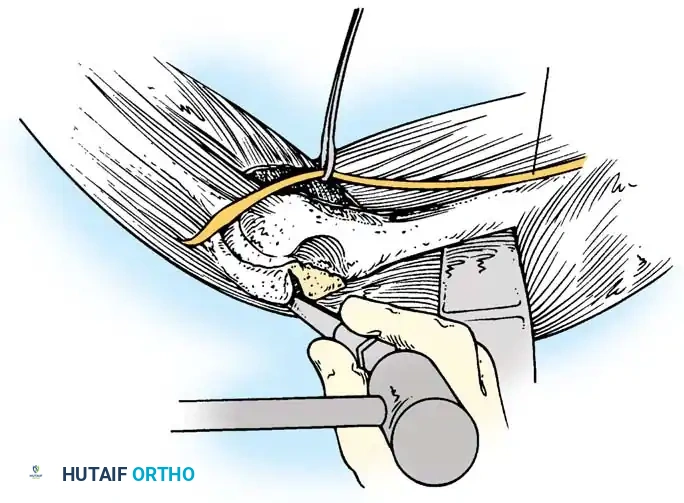
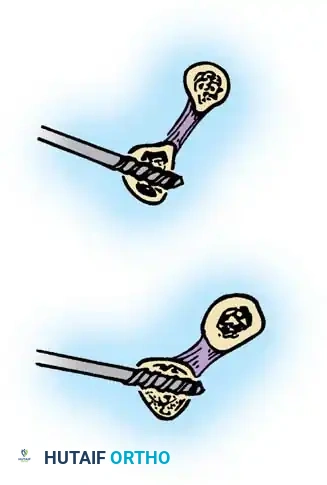
Extensive callus, organized hematoma, and heterotopic ossification are universally found bridging the posterior humerus and completely obliterating the olecranon and coronoid fossae. Use a combination of rongeurs, curettes, and a high-speed burr to meticulously clear these fossae of all fibrous tissue and ectopic bone. The fossae must be completely empty to accommodate the olecranon and coronoid processes during terminal extension and flexion, respectively.
Identify the "radial humeral horn" anterior to the radiocapitellar joint. This bony block must be sharply divided at its base with an osteotome and completely removed. Once the distal humerus is entirely free and the fossae are cleared, expose the radial head and meticulously clear the greater sigmoid notch (trochlear notch) of the ulna, removing any fibrillated cartilage or organized scar tissue.
To reduce the joint, apply steady, sustained longitudinal traction to the forearm, gently rotate the forearm through pronation and supination to stretch the interosseous membrane, and press firmly on the anterior surface of the capitellum to lever the radial head posteriorly and anteriorly into its native position. If significant resistance is met, do not use excessive force; instead, systematically re-evaluate and widen the soft-tissue releases to prevent catastrophic iatrogenic cartilage damage or distal humerus fracture. Once the radial head is concentrically reduced, gently slip the coronoid process distally and anteriorly over the trochlea.
Stabilization, Advanced Fixation, and Closure
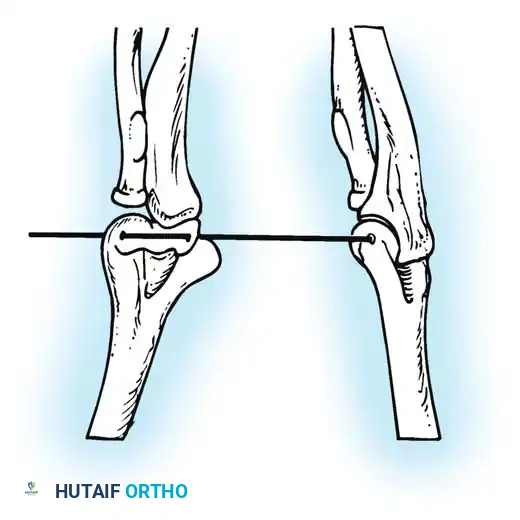
Carry the joint through a full range of motion under direct visualization. Because the collateral ligaments and capsule have been entirely released or excised, the elbow is frequently grossly unstable, particularly in extension. While static pinning with smooth Steinmann pins crossing the ulnohumeral joint at 90 degrees of flexion is a historical standard for profound instability, modern orthopedics strongly favors dynamic stabilization to permit early motion and prevent recurrent ankylosis.

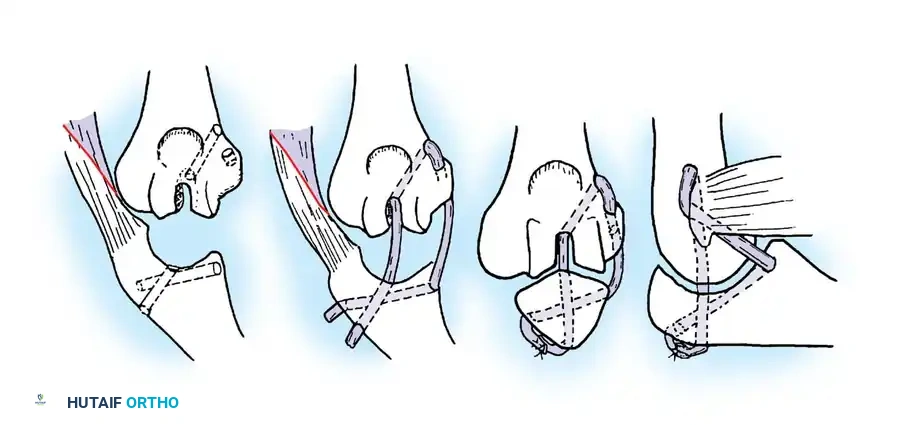
Arafiles described the creation of an intraarticular "cruciate" ligament using autologous tendon grafts (such as palmaris longus) passed through drill holes in the trochlea and greater sigmoid notch to stabilize the joint while allowing guarded flexion-extension exercises as early as 6 days postoperatively.
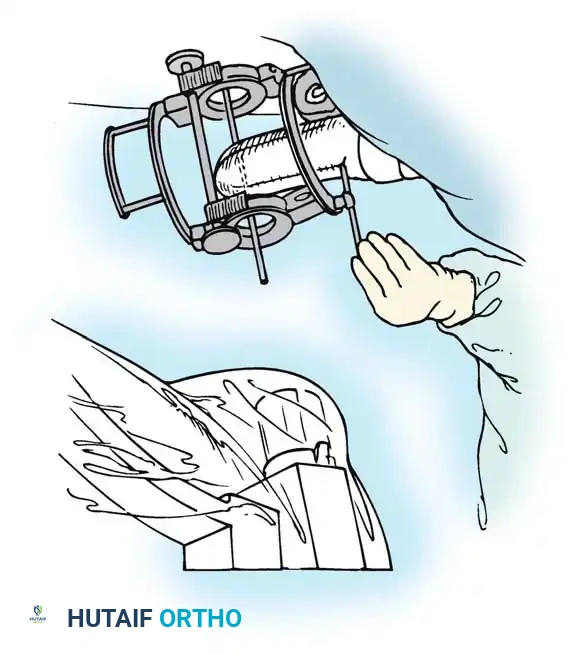
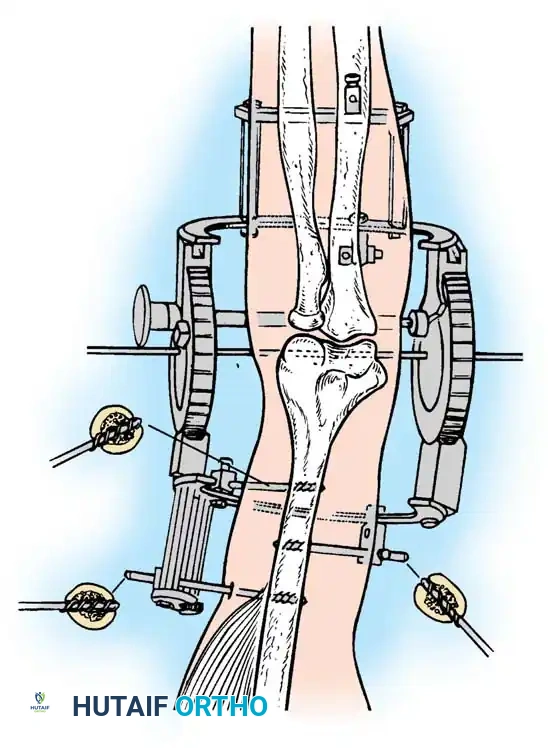
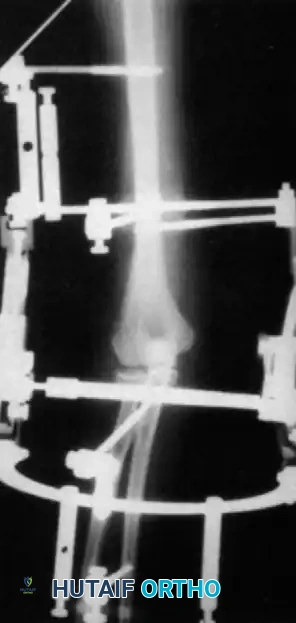
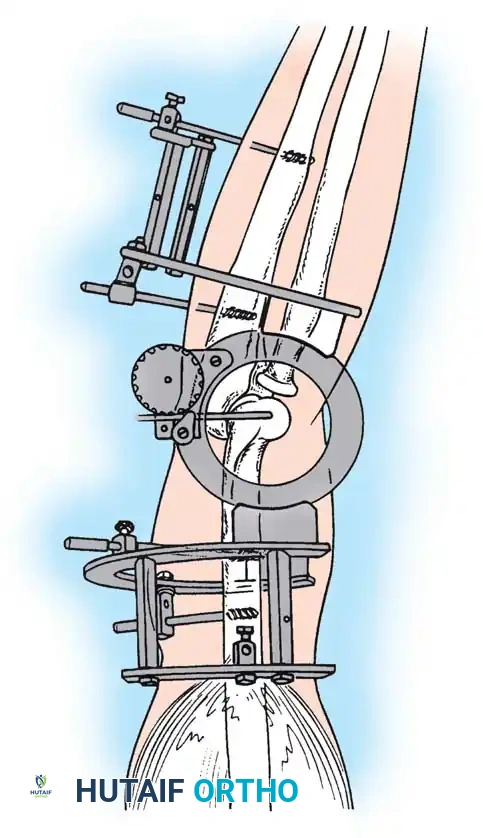
However, the current gold standard for managing instability following extensive open reduction is the application of a hinged elbow external fixator. Jupiter, Ring, and Hotchkiss have demonstrated excellent, reproducible results using hinged fixators (e.g., the Compass hinge) to maintain concentric joint reduction, permit early active and passive motion, and provide a rigid framework for continuous muscle-tendon stretching.
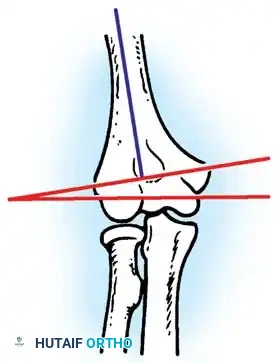
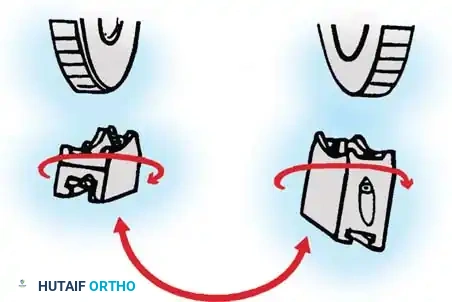
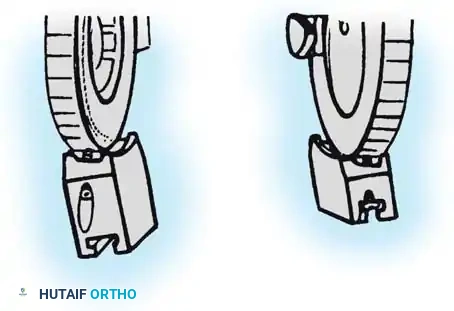
The ulnohumeral articulation is a highly constrained hinge joint. Locating the exact instant center of rotation is the most critical step in applying a dynamic fixator; this axis passes from the center of the capitellum laterally to the anteroinferior aspect of the medial epicondyle. The Compass hinge utilizes a precision worm gear to provide controlled displacement. Preoperative assembly is vital. The hinge block must be configured so the large block sits medially, accommodating the average 7 degrees of distal humeral valgus.
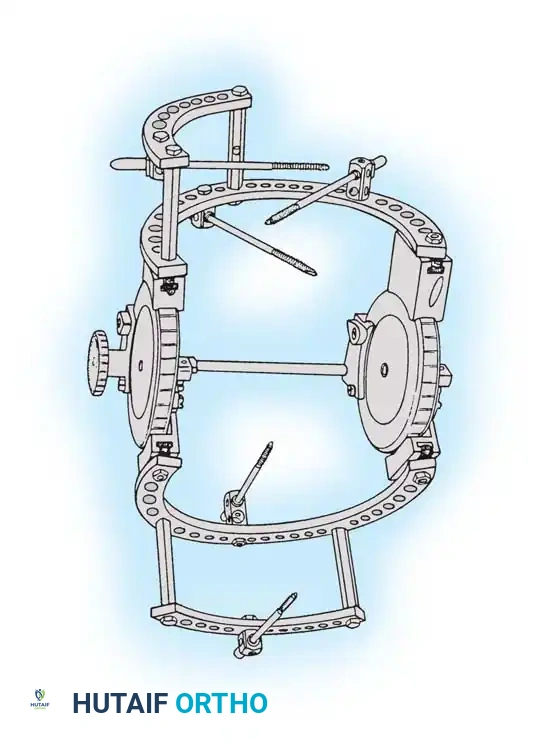
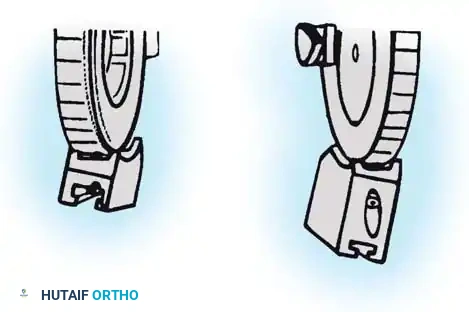
To convert the fixator for the appropriate laterality, the surgeon must manipulate the proximal blocks. Remove the proximal 5/8-inch ring by loosening the T-bolts, remove the proximal blocks using a hex wrench, switch the blocks to the opposite wheel, and rotate each block 180 degrees so the valgus tilt is reversed.
Following stabilization, closure is performed meticulously. Suture the periosteum and deep triceps fibers over the posterior humerus. Advance the V-Y tongue of the triceps aponeurosis and suture it into its normal position, or slightly more distally to accommodate the newly lengthened state of the extensor mechanism. Decompress the extensive surgical wound with a closed suction drain to prevent hematoma formation, and close the skin in layered, tension-free fashion.
Complications, Incidence Rates, and Salvage Management
The surgical management of old unreduced elbow dislocations is fraught with potential complications, owing to the extreme soft-tissue contractures, altered anatomy, and the necessity for aggressive, extensile surgical releases. Surgeons embarking on these procedures must be intimately familiar with potential pitfalls and possess the technical repertoire to execute immediate salvage strategies.
Heterotopic ossification (HO) is arguably the most pervasive complication, driven by the extensive surgical trauma superimposed on an already inflamed, chronic injury bed. The recurrence of massive HO can rapidly obliterate the newly restored joint space, leading to recurrent, profound stiffness. Prophylactic measures, including meticulous surgical hemostasis, immediate postoperative administration of non-steroidal anti-inflammatory drugs (NSAIDs) such as Indomethacin, and single-fraction localized radiation therapy, are strongly recommended in high-risk patients.
Ulnar neuropathy is another frequent complication, arising either from excessive intraoperative traction during the reduction maneuver or from postoperative perineural fibrosis. Meticulous anterior transposition of the ulnar nerve during the initial exposure significantly mitigates this risk. Iatrogenic fractures of the distal humerus or radial head can occur if excessive force is applied during the reduction of the osteopenic bone; this necessitates immediate internal fixation with low-profile locking plates.
| Complication | Estimated Incidence | Pathophysiology & Risk Factors | Salvage Management & Prevention |
|---|---|---|---|
| Recurrent Stiffness / Ankylosis | 25% - 40% | Inadequate release; failure of early rehab; recurrent HO. | Aggressive CPM; static progressive splinting; revision release. |
| Heterotopic Ossification (HO) | 30% - 50% | Extensive periosteal stripping; hematoma organization. | Indomethacin prophylaxis; targeted radiation; delayed excision (>6 mo). |
| Ulnar Neuropathy | 10% - 20% | Traction during reduction; encasement in scar tissue. | Prophylactic anterior transposition; delayed neurolysis if symptomatic. |
| Iatrogenic Fracture | 5% - 15% | Forceful levering of osteopenic bone during reduction. | Avoid excessive force; immediate ORIF with locking plates if occurs. |
| Deep Joint Infection | 2% - 5% | Extensile exposure; prolonged operative time; poor soft tissue. | Aggressive I&D; targeted IV antibiotics; potential hardware removal. |
Phased Post-Operative Rehabilitation Protocols
The ultimate success of an open reduction for a neglected elbow dislocation relies as much on the postoperative rehabilitation protocol as it does on the surgical execution. The rehabilitation must strike a delicate, continuous balance between protecting the tenuous soft-tissue repairs (particularly the lengthened triceps and any collateral ligament reconstructions) and aggressively combating the overwhelming biological drive toward recurrent stiffness.
Phase I: Immediate Postoperative Phase (Weeks 0-2)
Rehabilitation begins on postoperative day one. If a dynamic hinged external fixator has been applied, the hinge is unlocked to permit immediate active-assisted and passive range of motion within a safe arc determined intraoperatively. Continuous Passive Motion (CPM) machines are frequently utilized to maintain joint mobility and facilitate the clearance of intra-articular hematoma. Edema control is paramount; the extremity must remain strictly elevated. If static pinning was utilized instead of a dynamic fixator, the elbow remains immobilized in a posterior splint at 90 degrees of flexion to allow the soft tissues to quiet down, though this significantly increases the risk of permanent stiffness.
Phase II: Intermediate Mobilization Phase (Weeks 2-6)
During this phase, the focus shifts to maximizing the arc of motion. The hinged external fixator remains in place, acting as a dynamic stretching device. The patient is instructed to perform frequent, short sessions of active flexion and extension. The worm gear on the Compass hinge can be utilized by the therapist to incrementally stretch the joint into terminal extension and flexion, holding the position for prolonged periods to induce plastic deformation of the maturing scar tissue. Supination and pronation exercises are aggressively pursued, as the interosseous membrane and radiocapitellar articulation are highly prone to contracture.
Phase III: Fixator Removal and Strengthening (Weeks 6-12+)
The hinged external fixator is typically removed between 4 and 6 weeks postoperatively in the clinic setting. Following removal, the patient transitions to custom-molded static progressive or turnbuckle splints, worn primarily at night, to maintain the gains achieved during the day. Progressive resistance exercises are initiated to rebuild the atrophied triceps and biceps musculature. The lengthened triceps is particularly weak and requires dedicated, progressive eccentric and concentric loading. Maximum medical improvement is rarely achieved before 9 to 12 months postoperatively, and patients must be counseled preoperatively regarding the grueling nature of this protracted rehabilitation journey.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for old unreduced elbow dislocations is chronicled through several landmark publications that have shaped modern orthopedic paradigms.
Speed's seminal description in 1925 of the V-Y triceps lengthening technique remains the foundational surgical approach for overcoming the massive posterior contracture that defines these injuries. His technique of creating a broad aponeurotic flap allowed for the necessary extensile exposure while preserving the functional continuity of the extensor mechanism.
Silva's comprehensive review in 1958 provided the definitive documentation of the pathoanatomy, detailing the progression of myositis ossificans, capsular obliteration, and the critical tethering of the ulnar nerve. His work underscored the futility and danger
