Operative Management of Elbow Dislocations and Distal Radioulnar Joint Instability
Key Takeaway
Acute elbow dislocations are the second most common major joint dislocation in adults. While simple dislocations are typically managed nonoperatively with early mobilization, complex fracture-dislocations and irreducible radial head or distal radioulnar joint (DRUJ) injuries demand precise surgical intervention. This guide details the biomechanics, indications, and step-by-step operative techniques for annular ligament reconstruction, complex soft-tissue repair, and DRUJ stabilization to optimize functional recovery and prevent chronic instability.
Comprehensive Introduction and Patho-Epidemiology
The elbow is the second most common major joint dislocated in the adult population, superseded only by the glenohumeral joint, with an estimated annual incidence of 5.2 to 6.1 per 100,000 person-years. The demographic distribution is bimodal, peaking in young active males sustaining high-energy trauma or athletic injuries, and in elderly females secondary to low-energy falls on an outstretched hand (FOOSH) compounded by osteopenia. Approximately 20% of these dislocations are classified as complex, presenting with concomitant fractures of the radial head, coronoid process, or olecranon. The "terrible triad" of the elbow—a posterior dislocation combined with fractures of the radial head and coronoid process—represents a particularly devastating subset of complex instability that historically yielded abysmal outcomes prior to the advent of standardized surgical protocols.
Acute simple dislocations of the elbow, defined by the absence of associated fractures, are almost universally reducible via closed methods. Following concentric reduction, the majority of these joints demonstrate adequate stability through a functional arc of motion. Late elbow instability and chronic stiffness are exceedingly rare following simple dislocations, provided that appropriate, early rehabilitation protocols are instituted. However, the pathoanatomy of the dislocation event dictates that significant soft-tissue disruption has occurred. The mechanism typically involves a combination of axial loading, supination, and valgus stress, leading to a predictable sequence of capsuloligamentous failure.
Concurrently, injuries to the distal radioulnar joint (DRUJ) can occur in isolation or in association with complex forearm trauma, such as Galeazzi fracture-dislocations or Essex-Lopresti longitudinal radioulnar dissociations. The DRUJ is a highly specialized diarthrodial joint that facilitates the complex arc of forearm pronation and supination while transmitting loads from the carpus to the forearm axis. Disruption of the DRUJ profoundly alters the biomechanics of the upper extremity, leading to severe functional impairment, chronic ulnar-sided wrist pain, and early-onset osteoarthrosis if left unrecognized or inadequately treated. The epidemiology of DRUJ instability is frequently underreported, as simple ligamentous disruptions are often misdiagnosed as routine wrist sprains.
The overarching principle in managing both elbow and DRUJ instability is the restoration of congruent articular anatomy and the re-establishment of isometric ligamentous tension. Prolonged immobilization is historically associated with severe, recalcitrant arthrofibrosis, particularly in the elbow. The modern orthopedic surgeon must possess a profound understanding of the complex interplay between osseous constraints and dynamic soft-tissue stabilizers to navigate the operative and non-operative management of these challenging clinical entities successfully.
Detailed Surgical Anatomy and Biomechanics
The inherent stability of the elbow relies on a highly congruent osseous articulation—primarily the ulnohumeral joint—and a robust soft-tissue envelope. Morrey and colleagues elegantly categorized elbow stabilizers into primary, secondary, and tertiary constraints. The primary stabilizers consist of the ulnohumeral articulation, the medial ulnar collateral ligament (MUCL), and the lateral collateral ligament (LCL) complex. The ulnohumeral joint provides the critical osseous foundation, with the coronoid process acting as an anterior buttress against posterior subluxation. The MUCL, specifically its anterior bundle, is the primary restraint to valgus stress. It originates from the anteroinferior surface of the medial epicondyle and inserts onto the sublime tubercle of the proximal ulna.
The LCL complex is paramount in preventing posterolateral rotatory instability (PLRI). The lateral ulnar collateral ligament (LUCL), a critical component of this complex, originates from the isometric point on the lateral epicondyle and inserts onto the supinator crest of the ulna. O'Driscoll's concept of the "Horii circle" describes the sequential failure of these soft-tissue structures during a dislocation event. Disruption typically initiates laterally with the LUCL, progresses anteriorly and posteriorly through the capsule, and culminates medially with the MUCL. Secondary stabilizers include the radial head, which provides up to 30% of valgus stability (becoming the primary restraint if the MUCL is deficient), the anterior and posterior joint capsules, and the dynamic compressive forces generated by the common flexor and extensor muscle origins crossing the joint.
In the distal forearm, the primary biomechanical function of the DRUJ is to stabilize the radius as it rotates around the fixed distal ulna. The osseous architecture of the DRUJ—the articulation between the convex ulnar head and the shallow, concave sigmoid notch of the radius—confers minimal inherent stability. Therefore, stability is predominantly reliant on the triangular fibrocartilage complex (TFCC) and the extrinsic radioulnar ligaments. The volar and dorsal radioulnar ligaments are robust thickenings of the TFCC that dynamically tension during forearm rotation; the dorsal ligament tightens in pronation, while the volar ligament tightens in supination.
Further stabilization of the DRUJ is provided by the interosseous membrane (IOM), specifically its central band, which acts as a secondary restraint to proximal radial migration and DRUJ diastasis. The extensor carpi ulnaris (ECU) tendon and its associated subsheath also play a crucial dynamic role in stabilizing the ulnar aspect of the wrist. A catastrophic failure of the DRUJ, resulting in complete dislocation, necessitates the rupture of the radioulnar ligaments and significant disruption of the TFCC foveal attachments. Understanding the precise isometric points and tensioning patterns of these ligaments is absolutely critical when undertaking operative reconstruction, as non-anatomic repairs will inevitably lead to restricted rotation or recurrent instability.
Exhaustive Indications and Contraindications
The decision-making algorithm for operative intervention in elbow and DRUJ instability is dictated by the precise pathoanatomy, the chronicity of the injury, and patient-specific functional demands. For simple elbow dislocations, non-operative management with early, protected range of motion remains the gold standard. However, operative intervention is strictly indicated when concentric reduction cannot be achieved or maintained. A joint that subluxates or dislocates in greater than 30 to 45 degrees of extension following closed reduction is deemed grossly unstable and warrants surgical stabilization, typically via repair of the LCL complex. Complex fracture-dislocations, including the terrible triad, inherently demand aggressive surgical intervention to restore the osseous buttress (coronoid and radial head) and repair the capsuloligamentous structures.
In the context of the DRUJ, acute isolated dislocations that are concentrically reducible and stable in either pronation (for volar dislocations) or supination (for dorsal dislocations) are managed closed with cast immobilization for 4 to 6 weeks. Operative intervention becomes mandatory in the setting of irreducibility. The classic irreducible DRUJ dislocation is frequently caused by the interposition of the ECU tendon or its subsheath, the capsule, or an osteochondral fragment into the sigmoid notch. Furthermore, DRUJ instability occurring in conjunction with a radial shaft fracture (Galeazzi) that remains unstable following rigid anatomic fixation of the radius requires open exploration and TFCC repair or trans-osseous pinning.
Contraindications to operative intervention must be meticulously evaluated. Absolute contraindications include active local or systemic infection, severe medical comorbidities precluding safe anesthesia, and non-ambulatory patients with minimal functional demands where the risks of surgery outweigh the benefits of a stable joint. Relative contraindications include severe osteopenia or osteoporosis, which may compromise the purchase of internal fixation devices or suture anchors, and severe soft-tissue compromise (e.g., massive blistering or open wounds) that necessitates delayed intervention until the soft-tissue envelope has adequately recovered.
Indications and Contraindications Summary Table
| Clinical Entity | Primary Operative Indications | Non-Operative Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|---|
| Simple Elbow Dislocation | Irreducible by closed means; Unstable in >45° extension; Elite throwing athlete (MUCL repair). | Concentric reduction achieved; Stable through functional arc of motion. | Active systemic/local infection; Medically unfit for anesthesia. | Severe soft-tissue compromise (delay surgery); Low-demand elderly patient. |
| Complex Elbow Dislocation | "Terrible Triad"; Displaced coronoid/radial head fractures; Open fracture-dislocations. | Non-displaced fractures with stable congruent joint (rare). | Active infection; Medically unfit for anesthesia. | Severe osteopenia (consider arthroplasty over fixation). |
| Acute DRUJ Dislocation | Irreducible (ECU interposition); Unstable post-Galeazzi fixation; Essex-Lopresti injury. | Reducible and stable in pronation/supination; Isolated injury. | Active infection; Medically unfit for anesthesia. | Pre-existing severe DRUJ osteoarthritis (consider salvage). |
| Chronic DRUJ Instability | Persistent pain and instability >2 months; Failed conservative management. | Asymptomatic subluxation; Low functional demand. | Active infection; End-stage articular cartilage necrosis. | Fixed angular deformity of the radius (requires osteotomy first). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful surgical execution in complex joint instability. Standard radiographic evaluation must include true anteroposterior (AP) and lateral views of the elbow and wrist. In the setting of complex elbow instability, a non-contrast computed tomography (CT) scan with 3D reconstructions is mandatory. The CT scan delineates the precise fracture morphology of the coronoid process (O'Driscoll classification) and the radial head (Mason classification), dictates the requirement for specific implants (e.g., mini-fragment plates, suture lassos, or radial head prostheses), and identifies occult intra-articular osteochondral fragments. Digital templating should be performed to anticipate the size of a potential radial head arthroplasty, ensuring that overstuffing of the radiocapitellar joint—a common cause of post-operative stiffness and capitellar erosion—is avoided.
For DRUJ injuries, bilateral posteroanterior (PA) and lateral radiographs of the wrists are essential for comparison. Ulnar variance must be meticulously assessed. A true lateral radiograph, taken with the shoulder abducted 90 degrees, elbow flexed 90 degrees, and forearm in neutral rotation, is required to accurately diagnose dorsal or volar subluxation of the ulnar head. In subacute or chronic cases, magnetic resonance imaging (MRI) is highly sensitive and specific for evaluating the integrity of the TFCC, the radioulnar ligaments, and the interosseous membrane. If an Essex-Lopresti injury is suspected, imaging of the entire forearm axis is obligatory to assess for proximal migration of the radius.
Patient positioning is critical for optimal surgical exposure and fluoroscopic access. For elbow reconstructions, the patient is typically positioned supine with the arm draped over a radiolucent hand table, or in the lateral decubitus position with the operative arm resting over a padded post. The lateral decubitus position affords excellent access to the posterior, medial, and lateral aspects of the elbow, allowing gravity to assist in joint reduction. A sterile tourniquet is applied high on the brachium. For DRUJ procedures, the patient is positioned supine with the arm extended on a radiolucent hand table. The C-arm fluoroscopy unit should be positioned parallel to the table, allowing for dynamic, multi-planar imaging without compromising the sterile field. The surgeon must ensure that the entire upper extremity, from the axilla to the fingertips, is prepped and draped free to allow for unobstructed assessment of joint kinematics and forearm rotation intra-operatively.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of complex elbow instability typically utilizes a universal posterior skin incision. This approach allows access to both the medial and lateral aspects of the joint through full-thickness fasciocutaneous flaps, minimizing the risk of cutaneous nerve injury and avoiding multiple incisions. Once the deep fascia is exposed, the lateral side is addressed first.
Step-by-Step Operative Approach for Radial Head and LCL
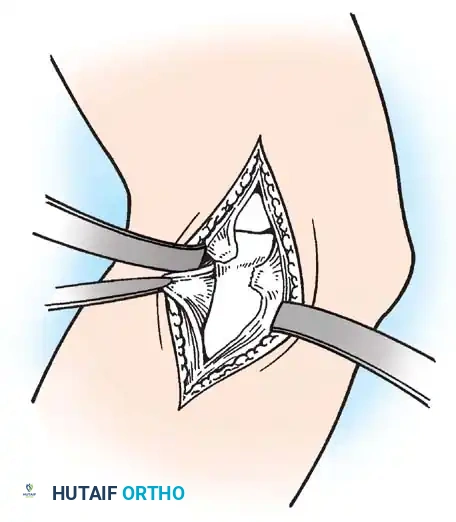
- Incision and Exposure: Make a longitudinal incision over the posterolateral aspect of the elbow, utilizing the Kocher interval between the anconeus (innervated by the radial nerve) and the extensor carpi ulnaris (innervated by the posterior interosseous nerve).
- Deep Dissection: Incise the common extensor origin and the underlying capsule anterior to the LUCL to preserve any remaining ligamentous integrity. Carefully expose the radiocapitellar joint and identify the remnants of the ruptured annular ligament and LUCL.
- Joint Clearance and Reduction: Meticulously debride any interposed capsular tissue, osteochondral fragments, or hematoma blocking the joint. Anatomically reduce the radial head into the radial notch of the ulna. If the radial head is fractured beyond repair, proceed with prosthetic replacement, ensuring the implant precisely matches the native head's height and diameter.
- Primary Repair: If the tissue quality permits, repair the annular ligament and the disrupted lateral capsule using fine, non-absorbable interrupted sutures. The LUCL must be reattached to its isometric origin on the lateral epicondyle using suture anchors.
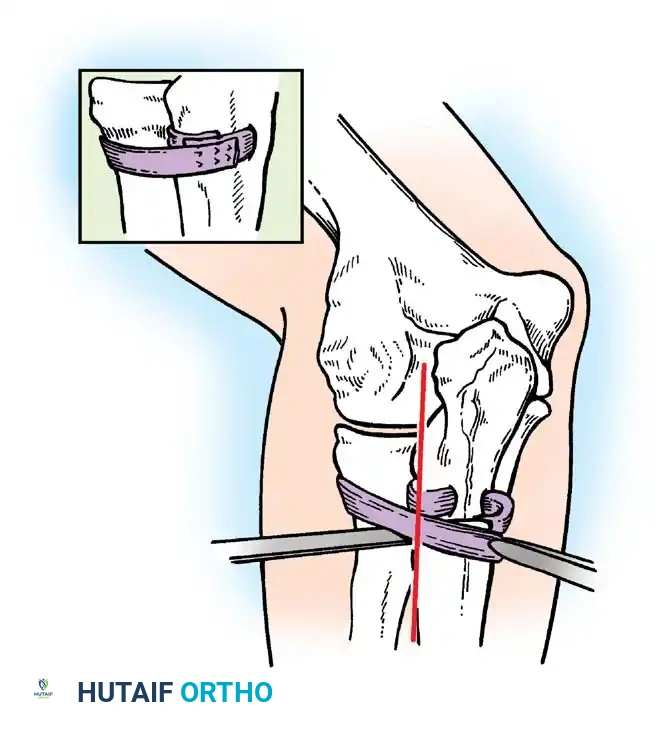
- Ligament Reconstruction (If Primary Repair Fails): If the native annular ligament is irreparable or deficient in chronic cases, harvest a fascial graft (1.3 cm wide × 10 cm long) from the ipsilateral fascia lata of the thigh or the deep dorsal fascia of the forearm.
- Ulnar Tunnel Preparation: Expose the posterior surface of the proximal ulna. Drill a transverse osseous tunnel through the ulnar metaphysis, precisely 1.3 cm distal to the articular level of the radial head, avoiding penetration of the radioulnar articulation.
- Graft Passage and Fixation: Pass the strip of fascia lata through this ulnar tunnel, loop it circumferentially around the radial neck, and suture its ends together under appropriate tension to create a robust, neo-annular ligament. The surgeon must dynamically test the construct to ensure the forearm can fully pronate and supinate without impingement or subluxation.
Management of the DRUJ
For DRUJ dislocations, Dameron emphasized classification based on the position of the ulna relative to the radius: dorsal or volar.
When open reduction is mandated—most commonly due to ECU tendon entrapment in a dorsal dislocation—a dorsal longitudinal incision is made over the distal ulna, centered over the 5th and 6th extensor compartments. The extensor retinaculum is incised, and the ECU is carefully mobilized and extricated from the sigmoid notch. The joint is irrigated, and the TFCC is inspected. If the TFCC is avulsed from the fovea, it is repaired using trans-osseous sutures or a bone anchor placed directly into the fovea at the base of the ulnar styloid.
In cases of chronic instability where the articular surfaces remain pristine, complex soft-tissue reconstructions are indicated. The Bunnell technique is a classic historical method used to tether the distal ulna and prevent dorsal subluxation.
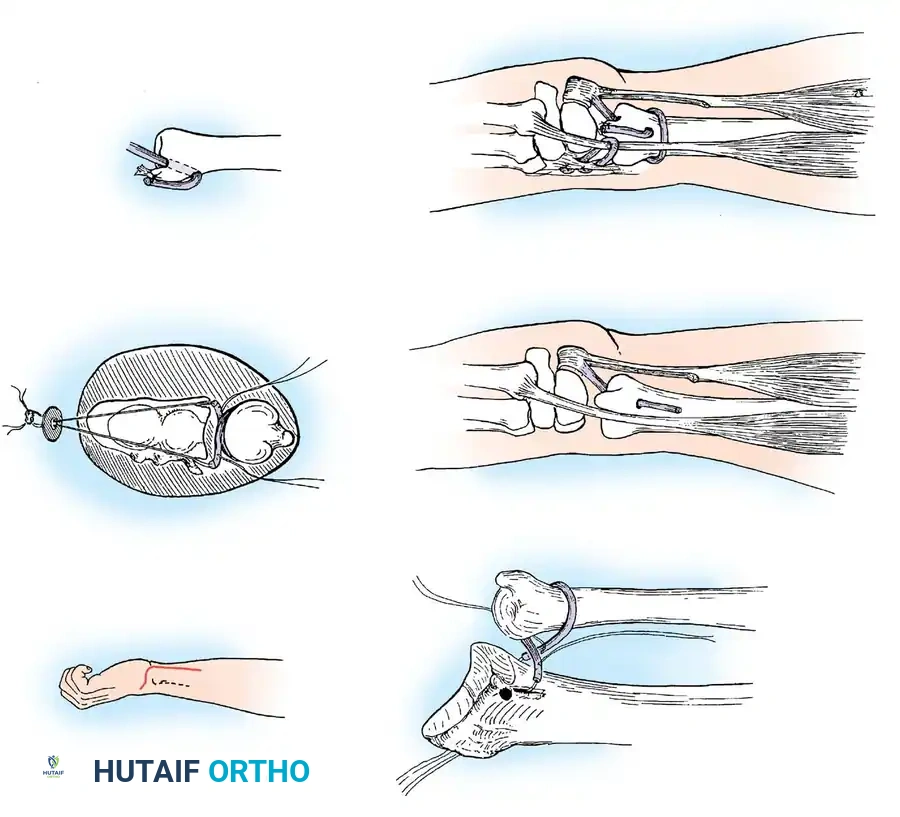
The Bunnell Stabilization Technique:
As illustrated, this procedure involves creating a dynamic and static tether to stabilize the distal ulna:
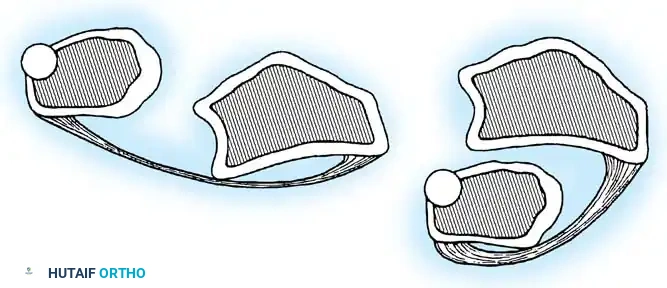
* A small tendon graft (often palmaris longus) is looped circumferentially around the neck of the ulna and anchored securely into the distal radius to recreate the radioulnar ligaments.
* A tenodesis of the distal ulna is performed using a split portion of the flexor carpi ulnaris (FCU) tendon.
* The extensor carpi ulnaris (ECU) tendon is anchored dorsally via a separate tendon loop to prevent volar subluxation of the tendon during active flexion and pronation of the wrist.
Following any DRUJ reconstruction, the joint must be pinned with a 0.062-inch Kirschner wire in the position of maximum stability (usually neutral rotation) for 4 weeks to protect the soft-tissue repair.
Complications, Incidence Rates, and Salvage Management
The operative management of elbow and DRUJ instability is fraught with potential complications, demanding meticulous surgical technique and vigilant post-operative care. In the elbow, the most ubiquitous complication is post-traumatic stiffness, or arthrofibrosis. The elbow capsule is highly sensitive to trauma and immobilization, rapidly developing dense fibrotic adhesions. Immobilization exceeding 3 weeks exponentially increases the risk of a permanent flexion contracture. Heterotopic ossification (HO), or myositis ossificans, is another severe complication, occurring in up to 20% of complex fracture-dislocations. Prophylaxis with Indomethacin or single-dose localized radiation therapy is strongly recommended in high-risk patients. If HO causes a mechanical block, surgical excision is delayed until the bone is metabolically mature (typically 6 to 9 months post-injury).
Recurrent instability is a devastating complication, usually resulting from failure to recognize and address all components of the "Horii circle," particularly the coronoid process or the LUCL. Chronic posterolateral rotatory instability (PLRI) presents with mechanical catching, snapping, and apprehension when pushing off a chair. Salvage management for PLRI requires formal ligamentous reconstruction using a palmaris longus or triceps fascia autograft. Neurological complications, particularly ulnar neuropathy, occur in up to 15% of complex elbow trauma. The ulnar nerve may be injured during the initial trauma, stretched during reduction, or entrapped in post-operative scar tissue. Routine in situ decompression or anterior transposition of the ulnar nerve is often performed during the index procedure for complex dislocations to mitigate this risk.
Complications following DRUJ reconstruction include chronic ulnar-sided wrist pain, restricted forearm rotation, and early-onset osteoarthrosis of the sigmoid notch. Failure of TFCC healing or graft attenuation leads to recurrent diastasis. If the articular cartilage of the DRUJ becomes necrotic or severely arthritic, soft-tissue reconstructions are definitively contraindicated. Salvage procedures must then be employed to eliminate the painful articulation while preserving forearm rotation. The Darrach procedure (resection of the distal ulnar head) is reserved for low-demand, elderly patients due to the high risk of painful radioulnar impingement. The Sauvé-Kapandji procedure (arthrodesis of the DRUJ with a proximal ulnar pseudoarthrosis) provides a more stable construct for higher-demand patients, preserving the ulnocarpal ligaments and preventing ulnar translation of the carpus.
Complications and Salvage Management Table
| Complication | Estimated Incidence | Etiology / Pathophysiology | Salvage Management / Treatment |
|---|---|---|---|
| Elbow Arthrofibrosis | 15% - 30% | Prolonged immobilization; capsular contracture. | Aggressive physical therapy; Open or arthroscopic capsular release (after 6 months). |
| Heterotopic Ossification | 10% - 20% | Severe soft-tissue trauma; forced passive stretching. | NSAID prophylaxis; Surgical excision once metabolically mature (normal alk phos/bone scan). |
| Recurrent PLRI | 5% - 10% | Unrecognized LUCL rupture; non-anatomic repair. | Formal LUCL reconstruction with autograft (palmaris longus/triceps fascia). |
| Ulnar Neuropathy | 10% - 15% | Traction injury; scar entrapment; prominent hardware. | Neurolysis; Anterior subcutaneous or submuscular transposition. |
| DRUJ Osteoarthrosis | 20% - 40% (Chronic) | Chronic instability; altered joint kinematics; cartilage necrosis. | Sauvé-Kapandji procedure; Ulnar head arthroplasty; Darrach procedure (elderly). |
Phased Post-Operative Rehabilitation Protocols
The rehabilitation following operative stabilization of elbow and DRUJ instability represents a delicate balance between protecting the surgical repair and preventing debilitating arthrofibrosis. A phased, meticulously structured protocol is mandatory. For simple elbow dislocations treated non-operatively, or those with secure ligamentous repairs, Phase I (0 to 2 weeks) involves immobilization in a posterior splint at 90 degrees of flexion. However, as emphasized by Mehlhoff et al., immobilization should rarely exceed 2 weeks. During this phase, active range of motion of the shoulder, wrist, and digits is initiated immediately to reduce edema and prevent distal stiffness.
Phase II (2 to 6 weeks) marks the initiation of protected, active, and active-assisted range of motion of the elbow. The patient is frequently transitioned to a hinged elbow brace. To protect a lateral collateral ligament repair, the forearm is maintained in pronation during elbow flexion and extension, which uses the intact medial structures and the radial head to buttress the lateral side. Conversely, if the MUCL was repaired, the forearm is maintained in supination. Extension is typically blocked at 30 degrees initially, with the block advanced by 10 to 15 degrees weekly. Gravity-assisted overhead motion protocols are highly effective; the patient lies supine with the shoulder flexed to 90 degrees, allowing gravity to gently assist elbow extension while minimizing triceps contraction, which can subluxate the joint.
Phase III (6 to 12 weeks) focuses on the restoration of terminal motion, progressive strengthening, and endurance. Passive stretching by a therapist is strictly prohibited, as forceful manipulation induces microtrauma, exacerbates inflammation, and dramatically increases the risk of heterotopic ossification. Strengthening of the dynamic stabilizers—the brachialis, biceps, triceps, and common flexor/extensor masses—is initiated using isometric and progressive resistive exercises. Return to heavy labor or elite athletics is generally restricted until 4 to 6 months post-operatively, contingent upon the restoration of functional motion and symmetric strength.
Rehabilitation for DRUJ reconstructions follows a distinct trajectory. Following TFCC repair or Bunnell stabilization, the forearm is immobilized in a Muenster or long-arm cast for 4 to 6 weeks to strictly prevent pronation and supination. The position of immobilization depends on the direction of instability: supination for dorsal dislocations and pronation for volar dislocations. After 6 weeks, the cast and trans-articular K-wires are removed, and active forearm rotation is initiated. Progressive strengthening of the ECU and pronator quadratus—vital dynamic stabilizers of the DRUJ—begins at 8 weeks. Full unrestricted activity is typically permitted at 3 to 4 months, provided there is no clinical evidence of recurrent diastasis.
Summary of Landmark Literature and Clinical Guidelines
The evolution of treatment protocols for elbow and DRUJ instability is deeply rooted in several landmark biomechanical and clinical studies. Josefsson et al. provided the foundational evidence for the non-operative management of simple elbow dislocations. In their prospective, randomized trials, they demonstrated that primary surgical repair of ruptured collateral ligaments in the setting of simple dislocations yielded no functional advantage over closed reduction and early functional mobilization. Indeed, the operative cohort frequently exhibited increased stiffness and inferior subjective outcomes. This established the current paradigm that the primary complication of simple dislocations is stiffness, not recurrent instability.
Mehlhoff and colleagues further refined non-operative protocols in their comprehensive review of 52 patients. They definitively correlated prolonged immobilization (greater than 3 weeks) with severe, recalcitrant flexion contractures. Their recommendation to initiate unprotected flexion and extension exercises within 2 weeks of the dislocation remains a cornerstone of modern conservative management. Conversely, in the high-demand athletic population, particularly overhead throwers, Burra and Andrews demonstrated that acute operative repair of the MUCL is often necessary to restore elite-level kinematics and prevent chronic valgus overload.
In the realm of complex instability, the contributions of O'Driscoll, Jupiter, and Ring are paramount. O'Driscoll's description of the "Horii circle" provided a unified biomechanical theory for the sequential soft-tissue failure in elbow dislocations, guiding the surgeon to systematically address the lateral, anterior, and medial constraints. Jupiter and Ring's extensive work on the "terrible triad" revolutionized its management. They established the absolute necessity of restoring the anterior osseous buttress (coronoid fixation) and the lateral column (radial head fixation or arthroplasty, combined with LUCL repair). Their standardized surgical protocol transformed a historically devastating injury into a manageable clinical entity with predictable, satisfactory outcomes.
Regarding the DRUJ, Dameron's classification system remains the standard for describing acute dislocations, while the anatomical studies by Palmer and Werner elucidated the critical stabilizing role of the TFCC. Milch's observations on radiographic diastasis of the DRUJ provided the diagnostic framework for identifying complete ligamentous ruptures. Collectively, this body of literature dictates that successful management of upper extremity instability requires an exacting anatomic diagnosis, rigid adherence to biomechanical principles during surgical reconstruction, and aggressive, structured post-operative rehabilitation.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been ---
