Open Reduction of Chronic Elbow Dislocations: A Comprehensive Surgical Guide

Key Takeaway
Open reduction of chronic elbow dislocations is a complex orthopedic challenge. Success is inversely proportional to the time elapsed since injury. The procedure requires meticulous ulnar nerve decompression, extensive capsuloligamentous release, and triceps lengthening. Post-reduction stability is often compromised, necessitating transarticular pinning, ligament reconstruction, or hinged external fixation to permit early range of motion and optimize functional recovery in the neglected elbow.
Comprehensive Introduction and Patho-Epidemiology
Neglected or chronic posterior dislocations of the elbow represent a formidable and technically demanding challenge in advanced orthopedic surgery. While acute elbow dislocations are relatively common and typically managed with closed reduction and brief immobilization in modern healthcare systems, chronic presentations are exceedingly rare in developed nations due to the ubiquity of advanced imaging and prompt acute care protocols. However, they remain a significant source of severe upper extremity morbidity in developing regions, rural environments, or in poly-traumatized patients where the initial injury was overlooked due to life-threatening neurosurgical or visceral trauma. By strict definition, an elbow dislocation is considered "chronic" or "neglected" when it remains unreduced for greater than three weeks, at which point profound and often irreversible pathoanatomical changes begin to occur within the joint architecture.
Although early historical literature and some isolated modern case series have reported that patients can regain a highly useful, functional arc of flexion and extension following the open reduction of old posterior dislocations—regardless of the patient's chronological age or the absolute duration of the unreduced state—the overwhelming consensus in contemporary orthopedic literature dictates a far more cautious and guarded prognosis. Most evidence-based reports and systematic reviews confirm that the likelihood of restoring useful, pain-free kinematics by open reduction alone is inversely proportional to the length of time from the initial injury to the surgical intervention. The longer the joint remains dislocated, the more extensive the required surgical release, and the higher the risk of post-operative stiffness, recurrent instability, or catastrophic cartilage failure.
Prolonged dislocation initiates a cascade of deleterious biological and mechanical events. This includes severe soft-tissue contractures, progressive articular cartilage degradation due to the absence of physiological loading and synovial fluid nutrition, and the rampant formation of heterotopic ossification (HO). The joint spaces, specifically the olecranon and coronoid fossae, become obliterated by dense, organized fibrous pannus. Consequently, managing these injuries necessitates a highly systematic, extensive, and meticulously executed surgical approach to restore joint congruity, re-establish the anatomical axes of rotation, and reconstruct the stabilizing capsuloligamentous constraints.
Pathophysiology of the Neglected Dislocation
Understanding the evolving pathophysiology of a chronic elbow dislocation is critical for anticipating intraoperative difficulties and formulating a successful surgical strategy. Over time, the displaced joint undergoes profound structural and biological changes that transform a simple mechanical dissociation into a complex fibro-osseous deformity. The most immediate and functionally limiting change is the severe contracture of the triceps brachii muscle. As the olecranon remains displaced posteriorly and proximally, the triceps muscle-tendon unit shortens significantly, acting as a massive, unyielding tether that physically prevents anatomical reduction without extensive surgical lengthening.
Concurrently, the capsuloligamentous structures undergo severe fibrotic transformation. The medial collateral ligament (MCL) and lateral collateral ligament (LCL) complexes, which are typically avulsed or ruptured during the initial trauma, heal in a shortened, non-anatomical position. They become densely scarred to the displaced humeral condyles and the surrounding muscular fascia, effectively locking the proximal ulna and radial head in their dislocated posterior position. The anterior capsule, now devoid of its normal tension, contracts and thickens, further resisting any attempt at anterior translation of the forearm.
Furthermore, the articular environment degrades rapidly. The normal articular cartilage of the trochlea, capitellum, and greater sigmoid notch, deprived of normal contact pressures and synovial fluid circulation, undergoes chondromalacia and eventual necrosis. Dense fibrous pannus proliferates extensively, filling the olecranon and coronoid fossae, entirely obliterating the normal articular spaces required to accommodate the proximal ulna during terminal flexion and extension. Additionally, heterotopic ossification, frequently manifesting as a "radial humeral horn" or extensive periarticular bridging bone, develops due to chronic periosteal stripping, organized fracture hematomas, and sustained inflammatory cascades.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the surgical anatomy and biomechanics of the elbow is an absolute prerequisite for undertaking the open reduction of a chronic dislocation. The elbow is a highly constrained, complex hinge joint comprising three distinct articulations: the ulnohumeral, radiohumeral, and proximal radioulnar joints. The primary stabilizer of the elbow is the highly congruent ulnohumeral articulation. The greater sigmoid notch of the ulna tightly wraps around the spool-shaped trochlea of the distal humerus, providing inherent osseous stability against both anteroposterior translation and varus-valgus angulation. In a chronic posterior dislocation, this critical osseous lock is bypassed, and the proximal ulna rests abnormally on the posterior metaphysis of the humerus, leading to remodeling and distortion of the bony landmarks.
The secondary stabilizers are the collateral ligament complexes. The lateral collateral ligament (LCL) complex, specifically the lateral ulnar collateral ligament (LUCL), is the primary restraint to posterolateral rotatory instability (PLRI). It originates from the lateral epicondyle and inserts on the supinator crest of the ulna. The medial collateral ligament (MCL) complex, primarily its anterior bundle, originates from the anteroinferior surface of the medial epicondyle and inserts on the sublime tubercle of the coronoid process, acting as the primary restraint to valgus stress. In chronic dislocations, these ligaments are not only contracted but their anatomical footprints are frequently obscured by massive scar tissue and heterotopic bone, complicating both release and subsequent reconstruction.
The musculotendinous units crossing the elbow joint also play a dual role as dynamic stabilizers and, in the chronic setting, major deforming forces. The triceps brachii, inserting broadly onto the olecranon, is the primary extensor and the chief impediment to reduction in neglected cases. Anteriorly, the brachialis and biceps brachii muscles cross the joint; while they may also contract, they are typically less problematic to overcome than the triceps. However, the brachialis muscle belly is often intimately scarred to the anterior capsule, requiring careful elevation to avoid iatrogenic injury to the anterior neurovascular bundle.
Neurovascular Considerations and Kinematics
The neurovascular anatomy surrounding the elbow is perilous, particularly when normal anatomical planes are distorted by chronic dislocation and heterotopic ossification. The ulnar nerve is at the highest risk. As it courses through the cubital tunnel posterior to the medial epicondyle, it becomes stretched, encased in dense scar tissue, or physically distorted by heterotopic bone in a chronic posterior dislocation. The median nerve and brachial artery, located anteriorly, are relatively protected by the brachialis muscle, but they can be compromised during aggressive anterior capsular releases or if the surgeon inadvertently strays anterior to the brachialis muscle belly during subperiosteal dissection.
Biomechanically, the elbow functions through a complex kinematic chain. The axis of flexion and extension is not a simple hinge but rather a highly specific isometric axis that passes through the center of the capitellum laterally and the anteroinferior aspect of the medial epicondyle medially. Restoring this precise anatomical axis of rotation is the ultimate goal of open reduction. If the joint is reduced but the axis remains slightly eccentric due to incomplete clearance of the fossae or asymmetric ligamentous tension, the joint will experience abnormal contact stresses, leading to rapid cartilage wear, recurrent subluxation, and inevitable failure of the surgical intervention.
Exhaustive Indications and Contraindications
The decision algorithm for treating a chronic elbow dislocation is highly nuanced and must be individualized based on patient-specific factors, the chronicity of the injury, the state of the articular cartilage, and the patient's functional demands. Open reduction with extensive soft-tissue release and potential ligamentous reconstruction remains the gold standard for young, high-demand patients who require a stable, load-bearing upper extremity. The primary indication is a patient presenting with a neglected dislocation (typically >3 weeks to several months old) who exhibits a painful, stiff, and functionally useless elbow, provided they have adequate bone stock and a viable articular surface.
Conversely, total elbow arthroplasty (TEA) has emerged as the most predictable and reliable surgical option for older, low-demand patients, particularly those presenting with extreme chronicity (e.g., >1-2 years), severe articular destruction, or profound osteopenia. In these patients, the extensive surgical release required for open reduction often results in a persistently stiff, painful, or grossly unstable joint, whereas TEA provides immediate stability and a functional arc of motion. However, TEA imposes strict lifetime lifting restrictions (typically limited to 5-10 lbs), making it an unacceptable option for young laborers or active individuals.
The presence of active infection or severe, medically unmanageable comorbidities constitutes an absolute contraindication to major joint reconstruction. Relative contraindications include profound neurological deficits (e.g., a complete, irreversible brachial plexus injury) where a mobile elbow would not improve overall limb function, or severe psychiatric conditions precluding adherence to the rigorous, prolonged postoperative rehabilitation protocol. In cases of massive bone loss or prior failed surgical attempts, salvage procedures such as elbow arthrodesis or resection arthroplasty may be considered, though these are generally viewed as last resorts due to their significant functional limitations.
| Parameter | Indications for Joint-Preserving Open Reduction | Contraindications / Indications for TEA or Salvage |
|---|---|---|
| Patient Age/Demand | Young, active, high-demand laborers. | Elderly, low-demand, sedentary lifestyle. |
| Chronicity of Injury | 3 weeks to 12 months (relative). | > 12 to 24 months with severe deformity. |
| Articular Cartilage | Viable, minimal to moderate chondromalacia. | Severe destruction, advanced osteoarthritis, necrosis. |
| Bone Stock | Adequate for potential anchor/pin fixation. | Profound osteopenia, massive structural bone loss. |
| Neurological Status | Intact or recovering motor/sensory function. | Irreversible paralysis of the upper extremity. |
| Patient Compliance | Highly motivated for prolonged rehabilitation. | Inability to comply with complex postoperative protocols. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful surgical outcome in chronic elbow dislocations. The foundation of this planning relies on comprehensive, multi-modality imaging. Standard anteroposterior (AP) and lateral radiographs of the elbow are mandatory to confirm the direction of the dislocation, assess overall bone quality, and identify gross heterotopic ossification or associated intra-articular fractures (e.g., radial head or coronoid fractures). However, plain radiographs are often insufficient for detailed surgical planning due to the overlapping of distorted bony landmarks.
A high-resolution Computed Tomography (CT) scan with 3-dimensional (3D) reconstructions is considered the gold standard and is absolutely essential. The 3D CT allows the surgeon to meticulously map the precise location and extent of heterotopic ossification, particularly the frequently encountered "radial humeral horn" or bridging bone across the radioulnar joint. It also facilitates the assessment of the olecranon and coronoid fossae to determine the volume of osseous and fibrous debris that must be excavated. While Magnetic Resonance Imaging (MRI) can provide information regarding the state of the articular cartilage and the collateral ligaments, its utility is often limited by the severe anatomical distortion and is generally not routinely required unless a specific soft-tissue pathology (like an isolated nerve entrapment) needs further elucidation.
Preoperative templating involves anticipating the required stabilization method. The surgeon must have immediate access to various fixation modalities, including heavy Kirschner wires and Steinmann pins for static transarticular fixation, a sterile hinged external fixator system for dynamic stabilization, and tendon allografts (e.g., palmaris longus or plantaris) if ligament reconstruction via the Arafiles technique is anticipated. Furthermore, in borderline cases where the viability of the joint is questionable, the surgeon must have a total elbow arthroplasty system available in the operating room as a definitive backup plan, fully consented by the patient beforehand.
Anesthesia and Patient Positioning
Optimal patient positioning and anesthesia are critical to facilitate the extensive exposure required. General anesthesia is typically employed, strongly supplemented by a regional anesthetic technique, such as a supraclavicular or axillary brachial plexus block. The regional block provides profound intraoperative muscle relaxation—essential for overcoming the severe triceps contracture—and excellent postoperative analgesia, which facilitates early rehabilitation.
The patient is most commonly placed in the lateral decubitus position, securely stabilized with a beanbag or pelvic positioners. The operative arm is draped free and rested over a padded L-bar or bolster, allowing the elbow to flex freely to 120 degrees and providing the surgeon with unobstructed, 360-degree access to the posterior, medial, and lateral compartments of the joint. Alternatively, the prone position can be utilized, though it may complicate airway management. A sterile, non-exsanguinating tourniquet is applied as high as possible on the brachium. Exsanguination is typically performed via gravity elevation for 3 to 5 minutes rather than using an Esmarch bandage, particularly if there is any concern for deep venous thrombosis due to the chronic immobility of the limb, though standard Esmarch exsanguination is acceptable in healthy patients.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution requires a systematic, unhurried approach, typically utilizing the Speed procedure, which combines a V-Y lengthening of the triceps with a radical, circumferential capsular release.
Step 1: Incision and Extensile Exposure
The operation commences with a generous, universal posterior longitudinal incision. Begin in the posterior midline of the arm approximately 10 to 12 cm proximal to the tip of the olecranon. Continue the incision distally, curving slightly laterally over the lateral humeral condyle and the radial head to avoid crossing directly over the tip of the olecranon, thereby minimizing the risk of postoperative wound breakdown and painful scar formation. Extend the incision further distally for about 5 to 7 cm onto the proximal posterior forearm.
Thick full-thickness fasciocutaneous flaps are undermined and retracted medially and laterally to expose the entire tendinous insertion and aponeurosis of the triceps muscle, the medial and lateral epicondyles, and the proximal ulnar crest.
Step 2: Mandatory Ulnar Nerve Neurolysis
Before any deep dissection, contracture release, or triceps lengthening is performed, it is an absolute, non-negotiable surgical mandate to identify, decompress, and protect the ulnar nerve. The nerve is located proximally along the medial border of the triceps and traced distally into the cubital tunnel. In a chronic dislocation, the nerve is frequently encased in dense perineural fibrosis, stretched taut over the displaced medial epicondyle, or severely distorted by heterotopic bone.
Meticulous, sharp dissection is required to free the nerve from the arcade of Struthers proximally to the flexor carpi ulnaris fascia distally. Once completely mobilized, the nerve is protected with a vessel loop. Given the severe tension the nerve will experience once the elbow is reduced and flexed, and the high likelihood of a compromised vascular bed, a routine anterior subcutaneous or submuscular transposition is highly recommended, as originally advocated by Silva and other leading authorities.
Step 3: Triceps V-Y Lengthening (The Speed Technique)
With the ulnar nerve protected, attention is turned to overcoming the primary deforming force: the contracted triceps. Beginning proximally and utilizing sharp dissection, the aponeurosis of the triceps is reflected distally to form a robust flap of tissue that remains firmly attached to the olecranon.
To perform the formal V-Y lengthening, begin the apex of the inverted "V" approximately 7.5 to 10 cm proximal to the joint line in the midline of the triceps muscle belly. Make full-thickness incisions through the muscle and aponeurosis, diverging distally toward the medial and lateral epicondyles. The lateral limb of the incision curves around the lateral edge of the olecranon, meeting the distal extent of the initial exposure. This creates a mobile, distally based tongue of triceps tendon and muscle that can slide distally during joint reduction, later to be repaired in a "Y" configuration.
Step 4: Radical Subperiosteal Release and Joint Debridement
Following the triceps release, the distal humerus must be completely skeletonized. Proceed with a radical subperiosteal elevation of all muscular and capsular attachments from the distal humerus, progressing from posterior to anterior. The posterior capsule, which is often thickened and adherent, is excised. The olecranon fossa is meticulously cleared of all dense fibrous pannus and organized hematoma using curettes and rongeurs until the normal cortical bone is visible.
The dissection then proceeds medially and laterally to release the severely contracted and malpositioned collateral ligaments. The attachments of the joint capsule and the shortened collateral ligaments around the medial and lateral condyles are sharply released or elevated with a periosteal elevator. Extreme caution is required when dissecting anteriorly over the medial condyle and the anterior distal humerus to avoid catastrophic iatrogenic injury to the median nerve and brachial artery, which may be tethered to the anterior capsule. All heterotopic ossification, particularly the radial humeral horn, must be identified via preoperative CT mapping and aggressively excised using osteotomes or a high-speed burr to remove any physical osseous blocks to reduction.
Step 5: Joint Reduction and Stabilization Strategies
Once the distal humerus is entirely mobilized, the fossae are cleared, and all osseous blocks are removed, gentle, sustained longitudinal traction is applied to the forearm. The ulnohumeral and radiohumeral joints are carefully manipulated into anatomical reduction. The surgeon must strictly avoid excessive, forceful levering, as the chronically disused, osteopenic bone is highly susceptible to iatrogenic crush fractures or condylar shear fractures.
Following successful reduction, the elbow is invariably grossly unstable due to the mandatory, extensive release of the collateral ligaments and capsule. Achieving immediate postoperative stability is paramount. The surgeon must choose between static pinning, dynamic external fixation, or formal ligament reconstruction.
Transarticular Pinning:
For straightforward stability, heavy Kirschner wires or Steinmann pins can be driven transarticularly. Typically, one pin transfixes the olecranon to the distal humerus, and another may transfix the capitellum to the radial head. While highly stable, this method completely prevents early motion, risking recurrent stiffness. Pins are generally left in place for 2 to 3 weeks before removal to initiate motion.

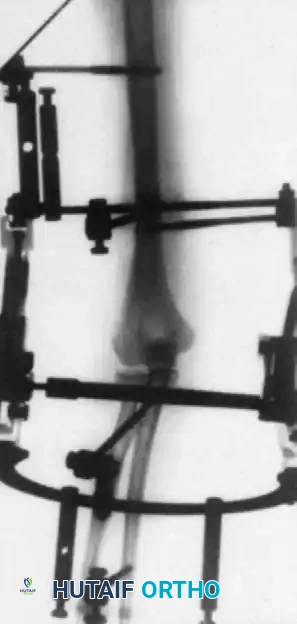
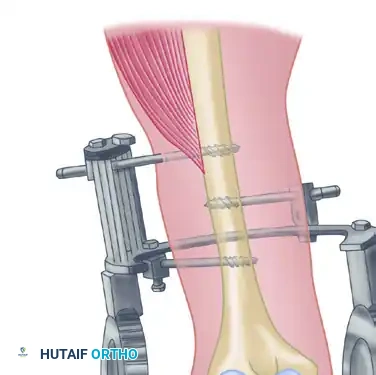
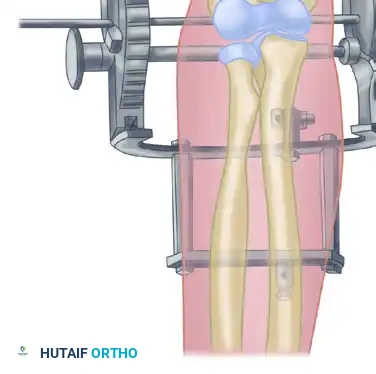
Hinged External Fixation:
The contemporary gold standard for stabilization is the application of a hinged external fixator. This device maintains concentric joint reduction while allowing immediate, guided active and passive range of motion. The critical technical challenge is perfectly aligning the axis of the fixator hinge with the anatomical axis of elbow rotation (passing through the center of the capitellum and the anteroinferior medial epicondyle). Even minor malalignment will lead to eccentric joint loading, cartilage shear, subluxation, and rapid pin-tract loosening.
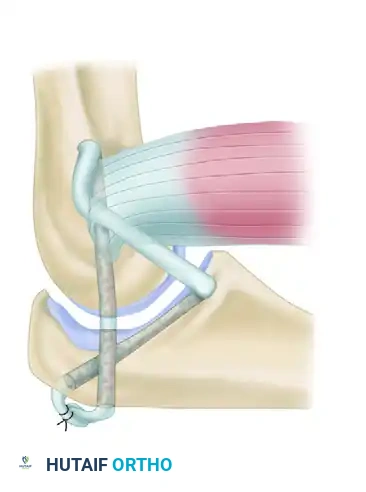
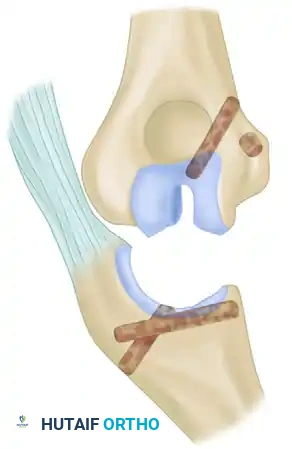
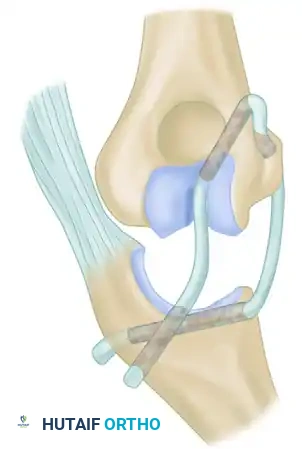
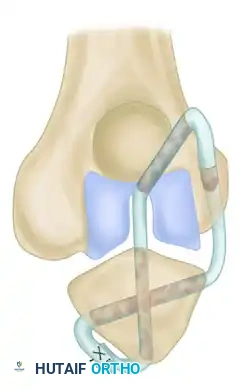
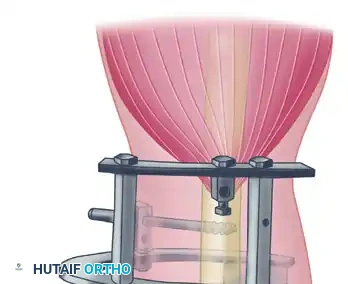
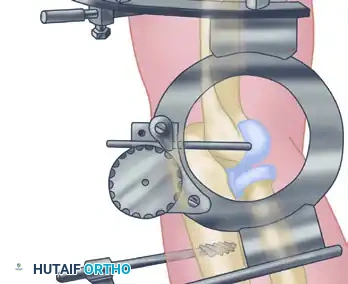
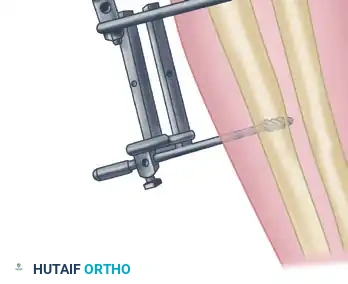
Ligament Reconstruction (The Arafiles Technique):
In cases of profound, unmanageable instability where a hinged fixator is unavailable or deemed insufficient, formal ligament reconstruction is required. The Arafiles technique is a complex, highly effective method utilizing a tendon autograft or allograft routed through precisely drilled osseous tunnels to recreate the stabilizing vectors of both the medial and lateral collateral ligaments simultaneously. The graft is passed through a slot created in the trochlea and routed in a figure-of-eight fashion to lock the joint anatomically while permitting flexion and extension.
The following sequence illustrates the meticulous steps of the Arafiles reconstruction, demonstrating the specific osseous tunnels and graft routing:



Complications, Incidence Rates, and Salvage Management
The open reduction of a chronic elbow dislocation is fraught with potential complications, and surgeons must be prepared to manage these complex sequelae. The extensive nature of the surgical exposure, combined with the compromised physiological state of the chronically dislocated joint, inherently elevates the risk profile compared to acute trauma surgery.
The most frequent complication is recurrent or persistent stiffness, affecting up to 50% of patients to varying degrees. Despite aggressive release and V-Y lengthening, the severe fibrotic tendency of the elbow often results in a functional arc of motion (typically 30 to 130 degrees) rather than full anatomical motion. Recurrent instability or subluxation occurs in 10-15% of cases, usually secondary to inadequate ligamentous reconstruction, premature pin removal, or malalignment of a hinged external fixator.
Ulnar neuropathy is a significant risk, occurring in 5-10% of cases despite prophylactic transposition, often due to intrinsic neural ischemia or traction injury during the reduction maneuver. Heterotopic ossification is a massive threat, given the extensive periosteal stripping and muscle trauma. Without rigorous prophylaxis, clinically significant HO can develop in up to 30% of patients, leading to bony ankylosis. Iatrogenic fractures of the osteopenic condyles or olecranon during the reduction maneuver are catastrophic complications that immediately compromise the stability of the reconstruction and often necessitate transition to an arthroplasty.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Persistent Stiffness | 30% - 50% | Inadequate release, prolonged immobilization, HO. | Aggressive PT, static progressive splinting, secondary arthrolysis. |
| Recurrent Instability | 10% - 15% | Failure of ligament repair, ex-fix malalignment. | Revision stabilization, hinged bracing, potential TEA if chronic. |
| Heterotopic Ossification | 15% - 30% | Extensive soft-tissue trauma, lack of prophylaxis. | Excision after maturation (typically > 6 months), radiation therapy. |
| Ulnar Neuropathy | 5% - 10% | Traction during reduction, inadequate transposition. | Observation, secondary neurolysis, and submuscular transposition. |
| Iatrogenic Fracture | < 5% | Forceful levering on osteopenic bone. | Internal fixation if possible; immediate Total Elbow Arthroplasty (TEA). |
| Deep Infection | 2% - 4% | Extensive exposure, prolonged operative time. | Aggressive I&D, hardware removal, targeted IV antibiotics. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is arguably as critical to the final clinical outcome as the surgical procedure itself. The regimen must strike a highly delicate, constantly monitored balance between protecting the tenuous soft-tissue capsuloligamentous repairs and preventing the rapid onset of recurrent fibro-osseous stiffness.
Phase I: Immediate Postoperative Period (0-2 Weeks)
The initial phase depends heavily on the chosen method of intraoperative stabilization. If static transarticular pins were utilized, the elbow is immobilized in a well-padded, rigid posterior splint at approximately 90 degrees of flexion with the forearm in neutral rotation. Elevation and aggressive edema control are paramount. If a hinged external fixator was applied, the approach is radically different. Continuous passive motion (CPM) or active-assisted range of motion (AAROM) under the direct supervision of a specialized physical therapist may begin within 24 to 48 hours postoperatively. This early motion is only permitted provided that immediate postoperative fluoroscopy or plain radiographs confirm that the joint reduction remains perfectly concentric throughout the arc of motion.
Phase II: Intermediate Mobilization (2-6 Weeks)
At the 2-to-3-week mark, transarticular pins (if used) are removed in the outpatient clinic. The patient is immediately transitioned to a custom-molded hinged elbow brace. Active and active-assisted exercises are formally initiated. The focus is on regaining the functional arc of motion (30 to 130 degrees of flexion, and 50 degrees of pronation/supination). A sling is utilized strictly for comfort between exercise sessions and during sleep to prevent inadvertent stress on the healing tissues. Passive, forceful stretching by the therapist is strictly contraindicated during this phase, as it incites an inflammatory response that paradoxically exacerbates stiffness and promotes heterotopic ossification.
Phase III: Strengthening and Maturation (6+ Weeks)
Beyond 6 weeks, the hinged brace is gradually weaned, first during the day and eventually at night. Isometric and isotonic strengthening exercises for the biceps, triceps, and forearm musculature are progressively introduced. The
