Thumb Metacarpal Extension Osteotomy: A Masterclass in Early CMC Arthritis Management

Key Takeaway
This masterclass guides fellows through the thumb metacarpal extension osteotomy, a crucial procedure for early carpometacarpal (CMC) joint arthritis. We meticulously cover surgical anatomy, preoperative planning, and step-by-step intraoperative execution, including staple and tension band fixation. Learn critical pearls, pitfalls, and comprehensive postoperative care to restore stability and function in the thumb.
Comprehensive Introduction and Patho-Epidemiology
The trapeziometacarpal (TM) joint of the thumb represents a marvel of evolutionary engineering, granting the human hand its unparalleled dexterity and capacity for forceful prehension. However, this evolutionary advantage comes at a significant biomechanical cost. The inherent architecture of the TM joint—a highly mobile, biconcave-convex saddle joint with minimal intrinsic bony constraint—renders it profoundly dependent on its surrounding capsuloligamentous envelope for stability. When these ligamentous restraints undergo attritional failure, the joint becomes susceptible to abnormal kinematics, leading to the early onset of osteoarthritis. The thumb metacarpal extension osteotomy has emerged as a biomechanically sound, joint-preserving intervention specifically designed to address this early-stage pathology, effectively halting or significantly delaying the degenerative cascade.
To fully appreciate the rationale behind the extension osteotomy, one must understand the precise pathophysiology of early CMC arthritis. Matthew Tomaino and colleagues demonstrated definitively that attritional changes in the anterior oblique ligament (AOL), frequently referred to as the "beak ligament," at its metacarpal attachment often precede any macroscopic degeneration of the articular cartilage. The AOL serves as the primary palmar stabilizer of the joint. When this critical restraint is compromised, the functional demands of lateral pinch and power grip subject the joint to unconstrained shear forces. This leads to a painful clinical syndrome characterized by synovitis, dynamic hypermobility, and a subjective "slipping" sensation as the metacarpal translates abnormally on the trapezium.
This abnormal translation generates excessive, localized contact pressures, particularly within the palmar compartment of the joint. Over time, these concentrated shear and compressive forces initiate the degradation of the palmar articular cartilage, marking the transition from dynamic instability to established early arthritis (Eaton-Littler Stage 1 and early Stage 2). While traditional interventions for early disease have included ligament reconstruction or arthroscopic synovectomy with temporary pinning, the thumb metacarpal extension osteotomy offers a uniquely powerful alternative. By surgically altering the mechanical axis of the first metacarpal, the procedure directly addresses the underlying pathomechanics, fundamentally redistributing joint contact forces and restoring dynamic stability without violating the joint capsule itself.
The biomechanical efficacy of this procedure was elegantly elucidated by Pellegrini and his contemporaries. By executing a dorsally based closing wedge osteotomy at the metacarpal base, the surgeon effectively unloads the compromised palmar contact area. The mechanical load is deliberately shifted dorsally onto the relatively pristine, intact articular cartilage. Consequently, the success of this procedure hinges entirely on appropriate patient selection: it is exclusively indicated when arthrosis does not extend beyond the palmar midpoint of the trapezium. Optimally, the degenerative changes should involve less than one-third of the palmar joint surfaces, ensuring that the newly loaded dorsal cartilage can withstand the transferred functional demands.
Detailed Surgical Anatomy and Biomechanics
Mastery of the thumb metacarpal extension osteotomy requires an intimate understanding of the complex functional anatomy and biomechanics of the trapeziometacarpal articulation. The procedure relies on leveraging osseous realignment to achieve secondary soft-tissue stabilization.
Osseous Architecture and Articular Geometry
The osseous foundation of the TM joint consists of the articulation between the first metacarpal base and the distal articular surface of the trapezium. The trapezium presents a saddle-shaped articular surface that is concave in the radioulnar plane and convex in the dorsovolar plane. Conversely, the base of the first metacarpal is convex in the radioulnar plane and concave in the dorsovolar plane. The palmar aspect of the metacarpal base features a distinct bony prominence known as the palmar "beak," which serves as the critical insertion site for the anterior oblique ligament. The osteotomy is strategically planned approximately 1 cm distal to this articular base. This specific location provides sufficient bony stock for hardware fixation while offering the necessary mechanical leverage to alter the joint's loading profile without directly violating the articular capsule.
Capsuloligamentous Stabilizers
The stability of the TM joint is governed by a complex network of ligaments. Bettinger et al. meticulously identified 16 distinct ligaments stabilizing the trapezium and the TM joint, with seven primary ligaments directly responsible for trapeziometacarpal stability.
The Anterior Oblique Ligament (AOL) is traditionally recognized as the primary restraint against dorsal radial subluxation. Bettinger further subdivided this structure into a superficial (sAOL) and deep (dAOL) component. The dAOL, the true intracapsular beak ligament, acts as the primary pivot point of the joint. It tightens during pronation, opposition, and palmar abduction, and serves to limit pronation in flexion. When the metacarpal is surgically placed into extension via the osteotomy, this ligamentous complex is indirectly tensioned, restoring a degree of its stabilizing function.
Equally important in the context of the extension osteotomy is the Dorsoradial Ligament (DRL). This wide, robust ligament spans a significant portion of the dorsal joint capsule, originating on the trapezium and inserting broadly onto the dorsum of the metacarpal base. While historically underappreciated, the DRL is now recognized as a critical primary stabilizer. It becomes taut under dorsoradial and dorsal translational forces, as well as during supination and pronation with joint flexion. Biomechanical studies have demonstrated that placing the metacarpal base in extension—the exact mechanical outcome of this osteotomy—significantly reduces joint laxity in multiple planes. Specifically, dorsal-volar laxity is reduced by up to 40%, radial-ulnar by 23%, and pronation-supination by 29%. This profound stabilization is largely attributed to the obligatory tightening of the DRL that occurs when the metacarpal is extended, effectively counteracting the palmar destabilization caused by an attenuated AOL.
Neurovascular and Musculotendinous Topography
Navigating the dorsal approach to the thumb metacarpal requires meticulous attention to regional neurovascular and musculotendinous structures. The most critical hazard is the Radial Sensory Nerve (RSN). The superficial branches of the RSN exhibit high anatomic variability as they course distally over the extensor retinaculum and the first dorsal compartment to provide sensation to the dorsal thumb. These branches frequently cross the surgical field directly over the extensor pollicis longus (EPL) tendon. Careless dissection, aggressive retraction, or stray electrocautery can result in neurapraxia, complete transection, or the formation of a debilitating, painful neuroma, which can easily overshadow the benefits of the osteotomy.
Additionally, the terminal branches of the lateral antebrachial cutaneous nerve may extend radially into the proximal aspect of the surgical field, necessitating careful subcutaneous dissection. The dorsal metacarpal arteries and veins, while small, must be systematically identified and coagulated to maintain the pristine, bloodless field required for precise osseous work. Muscularly, the interval of dissection lies adjacent to the tendons of the first and third dorsal compartments. The Extensor Pollicis Longus (EPL) courses obliquely across the dorsum of the first metacarpal and must be gently mobilized and protected during subperiosteal exposure. The Abductor Pollicis Longus (APL) and Extensor Pollicis Brevis (EPB) define the radial boundary of the safe working zone. Subperiosteal dissection must cleanly elevate the periosteum without placing undue traction on these tendinous insertions.
Exhaustive Indications and Contraindications
Patient selection is the single most critical determinant of success for the thumb metacarpal extension osteotomy. The procedure is not a salvage operation for advanced arthritis; rather, it is a highly specific, joint-preserving intervention tailored for early-stage disease. The ideal candidate is typically a younger, high-demand patient presenting with localized pain at the base of the thumb, particularly exacerbated by forceful pinch or grip activities.
Clinically, these patients often describe a subjective sensation of weakness or "giving way" in the thumb, corresponding to the dynamic instability caused by AOL attenuation. Physical examination may reveal localized tenderness directly over the palmar aspect of the TM joint. The trapeziometacarpal stress test—performed by applying axial compression and circumduction to the thumb metacarpal—frequently elicits sharp pain and a palpable dorsal subluxation. The classic "grind test" may be only subtly positive or manifest primarily as pain rather than coarse crepitance, reflecting the preservation of the dorsal articular cartilage.
Radiographic staging is paramount. The procedure is strictly indicated for Eaton-Littler Stage 1 disease, characterized by a normal joint space contour, potential slight widening due to effusion or synovitis, and a distinct absence of osteophytes or joint space narrowing. In highly selected cases of very early Eaton Stage 2 disease, where osteophytes are smaller than 2 mm and strictly limited to the palmar compartment, the procedure may still be considered. However, any evidence of dorsal cartilage wear, diffuse joint space narrowing, or concomitant scaphotrapezial-trapezoid (STT) arthritis serves as an absolute contraindication, as shifting the load onto already compromised dorsal cartilage will inevitably lead to rapid clinical failure.
| Indication / Contraindication | Specific Criteria | Biomechanical / Clinical Rationale |
|---|---|---|
| Primary Indication | Eaton-Littler Stage 1 CMC Arthritis | Joint space is preserved; symptoms are driven by dynamic instability and palmar shear forces. The osteotomy effectively redistributes these forces. |
| Secondary Indication | Early Eaton Stage 2 CMC Arthritis | Palmar osteophytes < 2mm. Dorsal cartilage must remain pristine to accept the transferred mechanical load following the extension osteotomy. |
| Clinical Indication | Painful hypermobility / AOL attenuation | Patient experiences "slipping" or weakness during lateral pinch. The osteotomy indirectly tightens the Dorsoradial Ligament (DRL) to restore stability. |
| Absolute Contraindication | Eaton Stage 3 or 4 CMC Arthritis | Diffuse cartilage loss and significant osteophytosis. Shifting load to degenerate dorsal cartilage will exacerbate pain and accelerate failure. |
| Absolute Contraindication | Scaphotrapezial (STT) Arthritis | The osteotomy alters mechanics across the entire trapeziometacarpal complex; pre-existing STT arthritis will become highly symptomatic. |
| Absolute Contraindication | Inflammatory Arthropathies (e.g., Rheumatoid) | Disease process involves global capsular destruction and pan-articular cartilage loss, negating the mechanical benefits of focal load shifting. |
| Relative Contraindication | Significant Metacarpophalangeal (MCP) Hyperextension | Pre-existing MCP hyperextension (>30 degrees) may be exacerbated by placing the metacarpal base in extension, requiring concurrent MCP stabilization. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning ensures precise execution and predictable outcomes. The diagnostic workup must first definitively exclude other common etiologies of radial-sided wrist and thumb pain, including De Quervain tenosynovitis, Flexor Carpi Radialis (FCR) tendinitis, intersection syndrome, and isolated STT arthritis. Once early TM joint arthritis is confirmed, a comprehensive trial of nonoperative management is mandatory. This includes non-steroidal anti-inflammatory drugs (NSAIDs), rigid thumb spica splinting, targeted thenar isometric strengthening to enhance dynamic muscular stability, and judicious use of intra-articular corticosteroid injections. Surgical intervention is reserved for patients who remain highly symptomatic despite a minimum of three to six months of dedicated conservative therapy.
High-quality, standardized radiographic imaging is the cornerstone of surgical templating. A standard posteroanterior (PA) view, a true lateral view of the thumb, and a Robert (pronated anteroposterior) view are required. The Robert view is particularly valuable for profiling the trapeziometacarpal joint space and identifying subtle palmar osteophytes that might preclude the procedure. Furthermore, a PA 30-degree oblique stress view, obtained by having the patient forcefully press the tips of the thumbs together, is excellent for dynamically assessing joint space narrowing and the degree of radial subluxation.

Figure 1A: Preoperative Robert (AP) radiograph of the thumb, demonstrating preserved joint space indicative of early-stage disease suitable for osteotomy.
Figure 1B: Preoperative lateral radiograph of the thumb. Note the relationship of the metacarpal to the trapezium, which will be altered via the closing wedge osteotomy.
Surgical templating is performed directly on the lateral radiograph. The surgeon measures the total length of the first metacarpal. A mark is placed exactly 1 cm distal to the articular surface of the metacarpal base. From this point, a 30-degree dorsally based closing wedge is templated. The apex of the wedge must terminate precisely at the volar cortex, ensuring the volar periosteal hinge remains intact. This intact hinge is critical for maintaining stability during hardware placement and promoting rapid osseous union.
On the day of surgery, the patient is placed in the supine position on the operating table. A standard, stable hand table is attached, and the operative extremity is prepped and draped in a standard sterile fashion. Anesthesia is typically achieved via a regional axillary or supraclavicular block, which provides profound intraoperative anesthesia and excellent postoperative pain control, minimizing the need for systemic opioids. A pneumatic tourniquet is applied high on the brachium. The C-arm fluoroscopy unit is positioned parallel to the hand table, entering from the distal or contralateral side, ensuring unimpeded access for obtaining true AP, lateral, and oblique views of the thumb metacarpal throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the thumb metacarpal extension osteotomy demands meticulous soft-tissue handling and precise osseous geometry. Following exsanguination of the limb with an Esmarch bandage, the pneumatic tourniquet is inflated to 250 mmHg.
A straight or slightly curved dorsal longitudinal incision, approximately 3 to 4 cm in length, is made over the proximal aspect of the first metacarpal, beginning just proximal to the TM joint line and extending distally. The initial subcutaneous dissection must be performed with extreme caution using blunt techniques (e.g., tenotomy scissors or a mosquito hemostat) to identify and protect the superficial branches of the radial sensory nerve. These nerve branches are mobilized gently and retracted radially or ulnarly using vessel loops, keeping them entirely out of the zone of injury.
Once the sensory nerves are secured, the deep fascia is incised. The interval between the extensor pollicis longus (EPL) and the extensor pollicis brevis (EPB) is developed. The EPL is retracted ulnarly, and the EPB/APL complex is retracted radially. A longitudinal incision is made through the periosteum along the dorsal midline of the metacarpal. Using a sharp Freer or small Cobb elevator, a subperiosteal dissection is performed circumferentially around the proximal metacarpal. It is imperative to expose the bone adequately while maintaining the integrity of the volar soft tissues to protect the vital volar periosteal hinge.
A 25-gauge needle is inserted into the trapeziometacarpal joint to serve as a definitive radiographic landmark. Under fluoroscopic guidance, a surgical marker or a fine K-wire is used to mark the planned osteotomy site exactly 1 cm distal to the joint line.

Figure 2A: Intraoperative fluoroscopy confirming the position of the joint line and the planned osteotomy site 1 cm distally.
With the site confirmed, the osteotomy is executed. A microsagittal saw equipped with a fine blade is utilized. The distal cut is typically made first, perpendicular to the long axis of the metacarpal shaft. The proximal cut is then made at a 30-degree angle to the distal cut, originating dorsally and converging exactly at the volar cortex. Continuous saline irrigation is mandatory during sawing to prevent thermal necrosis of the bone, which could lead to nonunion.
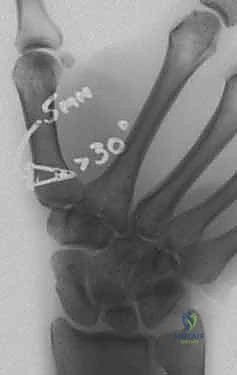
Figure 2B: Execution of the 30-degree dorsally based closing wedge osteotomy using a microsagittal saw. Note the protection of surrounding soft tissues.
The critical maneuver is the closure of the osteotomy. The dorsal wedge of bone is carefully removed. Gentle dorsal pressure is applied to the distal metacarpal shaft, closing the gap and compressing the osteotomy site. The volar cortex acts as a dynamic hinge. If the volar cortex is inadvertently breached, the construct becomes highly unstable, and rigid plate fixation becomes mandatory.
Once reduced, the osteotomy is provisionally stabilized with a 0.045-inch K-wire driven obliquely across the osteotomy site. Fluoroscopy is utilized to confirm the anatomic reduction, the complete closure of the dorsal gap, and the appropriate extension posture of the metacarpal base.
Definitive fixation can be achieved via multiple modalities, including intraosseous wiring, crossed K-wires, low-profile titanium plates, or shape-memory nitinol staples. Staple fixation is highly favored in modern practice due to its low profile, dynamic compressive properties, and ease of insertion. If utilizing a staple, a drill guide is placed across the closed osteotomy, and holes are drilled into the proximal and distal segments. The appropriately sized staple is inserted and tamped flush with the dorsal cortex.

Figure 3: Final fluoroscopic lateral view demonstrating a closed extension osteotomy securely fixed with a shape-memory compression staple.
Following final fluoroscopic verification of hardware placement and joint congruency, the surgical site is copiously irrigated. The periosteum is closed over the hardware using fine absorbable suture, provided it does not cause tension. The skin is closed with interrupted non-absorbable sutures. A sterile compressive dressing is applied, and the thumb is immobilized in a rigid, well-padded thumb spica splint with the interphalangeal joint left free.
Complications, Incidence Rates, and Salvage Management
While the thumb metacarpal extension osteotomy is highly effective, it is technically demanding and carries a specific complication profile. Meticulous surgical technique and rigorous adherence to indications are the primary defenses against adverse outcomes.
The most devastating soft-tissue complication is injury to the Radial Sensory Nerve (RSN). Even minor traction neuropraxia can result in profound dysesthesia, while partial or complete transection frequently leads to the formation of a terminal neuroma. A neuroma in this highly mobile, superficially exposed area can cause debilitating pain that eclipses the original arthritis symptoms. Prevention relies entirely on careful, blunt subcutaneous dissection and gentle retraction. If a neuroma develops and fails conservative management (desensitization, gabapentinoids, targeted injections), surgical excision and proximal transposition of the nerve end into the brachioradialis muscle belly may be required.
Osseous complications include delayed union, nonunion, and malunion. Nonunion is relatively rare (occurring in <5% of cases) due to the excellent vascularity of the metaphyseal bone, provided the volar periosteal hinge remains intact and thermal necrosis is avoided during the saw cuts. If the volar hinge is violated, the risk of nonunion or dorsal apex malunion increases significantly. Hardware prominence is another potential issue, particularly in thin individuals or if bulky plates are utilized. Symptomatic hardware may necessitate removal after complete radiographic consolidation of the osteotomy (typically at 4 to 6 months postoperatively).
Ultimately, the most common long-term "complication" is the natural progression of the underlying osteoarthritis. While the osteotomy alters mechanics to delay degeneration, it does not cure the disease. Patients must be counseled that salvage procedures may be required 10 to 15 years postoperatively.
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management / Treatment |
|---|---|---|---|
| Radial Sensory Nerve Injury / Neuroma | 5% - 10% | Blunt subcutaneous dissection; avoid electrocautery near superficial fascia; gentle vessel loop retraction. | Gabapentinoids; localized steroid injection; surgical excision and proximal muscular embedding of the nerve end. |
| Nonunion / Delayed Union | < 5% | Preserve the volar periosteal hinge; utilize copious saline irrigation during saw cuts; ensure rigid compression. | Prolonged immobilization; bone stimulator; revision surgery with rigid plate osteosynthesis and autologous bone grafting. |
| Hardware Prominence / Irritation | 10% - 15% | Utilize low-profile implants (e.g., compression staples or specialized mini-fragment plates); ensure hardware is flush with cortex. | Hardware removal after definitive radiographic union (minimum 4-6 months post-op). |
| Malunion (Dorsal Apex Angulation) | < 5% | Accurate templating; provisional K-wire fixation before final hardware placement; intraoperative fluoroscopic verification. | Corrective osteotomy (rarely indicated); usually managed expectantly unless causing severe biomechanical deficit. |
| Progression of CMC Arthritis | 20% - 30% at 10 years | Strict adherence to indications (Eaton Stage 1 only); avoid in patients with dorsal cartilage wear. | Trapeziectomy with or without Ligament Reconstruction and Tendon Interposition (LRTI); CMC Arthrodesis. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a thumb metacarpal extension osteotomy must carefully balance the need for rigid osseous protection with the goal of restoring functional mobility. A phased, closely monitored protocol guided by a certified hand therapist (CHT) is essential for optimizing outcomes.
Phase I: Immediate Postoperative Protection (Weeks 0-4)
Immediately following surgery, the thumb is immobilized in a rigid, custom-molded thermoplastic thumb spica splint or a short-arm thumb spica cast. The wrist is positioned in slight extension, and the thumb is placed in palmar abduction, with the interphalangeal (IP) joint left completely free. The primary goals during this phase are to control edema, protect the osteotomy site, and prevent stiffness of the uninvolved joints. Patients are instructed to perform active range of motion (AROM) exercises for the IP joint of the thumb, as well as the metacarpophalangeal and interphalangeal joints of the fingers, multiple times daily. Heavy lifting and gripping are strictly prohibited.
Phase II: Controlled Mobilization (Weeks 4-8)
At approximately 4 weeks postoperatively, clinical and radiographic evaluations are performed. If radiographs demonstrate early bridging callus and the patient is non-tender over the osteotomy site, the rigid immobilization is transitioned to a removable, custom-molded thumb spica orthosis. The patient begins a supervised program of active and active-assisted range of motion for the wrist and the thumb CMC joint. Therapy focuses on restoring palmar abduction, radial abduction, and opposition. The splint is worn at all times between exercise sessions and at night. Passive stretching and forceful pinch activities remain contraindicated to avoid stressing the healing bone and the newly tensioned ligamentous complex.
Phase III: Strengthening and Functional Return (Weeks 8-12+)
By week 8, assuming definitive radiographic union is confirmed, the protective splint is gradually discontinued. The rehabilitation focus shifts toward progressive strengthening. Isometric exercises for the thenar musculature are initiated, followed by dynamic strengthening using therapy putty and hand grippers. Proprioceptive training and dynamic stabilization exercises are crucial to re-educate the neuromuscular control of the thumb. Patients are gradually transitioned back to their normal activities of daily living. Return to heavy manual labor, forceful repetitive gripping, or contact sports is typically permitted between 10 and 12 weeks, contingent upon the complete resolution of pain and the restoration of near-normal grip and pinch strength.
Summary of Landmark Literature and Clinical Guidelines
The foundation of the thumb metacarpal extension osteotomy rests upon a robust body of biomechanical and clinical literature. The procedure represents a paradigm shift from salvage to joint preservation, supported by rigorous anatomical studies.
The seminal work by Pellegrini et al. in the early 1990s provided the biomechanical justification for the procedure. Through elegant cadaveric contact-pressure studies, they demonstrated that a 30-degree extension osteotomy significantly unloads the palmar compartment of the trapezium—the epicenter of early degenerative change—and redistributes the forces to the thicker, preserved dorsal cartilage. Their work established the fundamental geometric parameters (a 30-degree closing wedge) that remain the gold standard today.
Tomaino's clinical investigations further validated the procedure, highlighting the critical role of the anterior oblique ligament (AOL). His studies emphasized that early CMC arthritis is primarily a disease of ligamentous attrition and dynamic instability. By altering the metacarpal axis, the osteotomy compensates for this laxity. Long-term clinical follow-up studies by Tomaino and others have demonstrated excellent pain relief and preservation of grip strength in appropriately selected patients, with survivorship of the native joint exceeding 80% at 10-year follow-up.
Finally, the exhaustive anatomical mapping by Bettinger et al. clarified the complex ligamentous anatomy of the TM joint. Their identification of the dorsoradial ligament (DRL) as a primary stabilizer provided the missing biomechanical link, explaining how an extension osteotomy achieves secondary soft-tissue stabilization. By extending the metacarpal, the DRL is placed under tension, effectively creating a dorsal tether that resists the palmar subluxation forces generated during lateral pinch.
Current clinical guidelines strongly support the use of the thumb metacarpal extension osteotomy as a Level III/Grade B recommendation for young, high-demand patients with painful, symptomatic Eaton Stage 1 trapeziometacarpal arthritis who have failed comprehensive nonoperative management. Strict adherence to these indications, combined with meticulous surgical technique, ensures that this masterclass procedure remains a highly effective tool in the orthopedic surgeon's armamentarium.
