Trapeziometacarpal Ligament Reconstruction and Arthroplasty: A Comprehensive Guide
Key Takeaway
Trapeziometacarpal ligament reconstruction, pioneered by Eaton and Littler, is a cornerstone procedure for addressing basal joint instability and early-stage arthrosis. This technique utilizes a distally based strip of the flexor carpi radialis (FCR) tendon to reconstruct the volar beak ligament, restoring biomechanical stability. Advanced modifications, including the Calandruccio interposition arthroplasty, offer robust solutions for end-stage pantrapezial arthritis by combining ligamentous reconstruction with biological interposition.
Comprehensive Introduction and Patho-Epidemiology
The trapeziometacarpal (TMC) joint of the thumb represents an evolutionary masterpiece, characterized by a highly specialized biconcave saddle configuration that affords the first digit its unique, wide-ranging multi-planar mobility. This mobility encompasses flexion, extension, abduction, adduction, and the critical compound movement of opposition, which is fundamental to human prehension, precision pinch, and power grasp. However, this extraordinary kinematic freedom comes at the steep physiological cost of inherent osseous instability. The bony architecture relies heavily on a complex network of static capsuloligamentous restraints and dynamic musculotendinous forces to maintain joint congruity during functional loading. When these stabilizing mechanisms fail, the cascade of trapeziometacarpal arthrosis begins, representing one of the most ubiquitous and debilitating degenerative joint conditions encountered by orthopedic hand surgeons.
Pathophysiologically, the genesis of TMC osteoarthritis is intimately linked to the attenuation or traumatic rupture of the primary static stabilizers, historically considered to be the anterior oblique ligament (AOL), often referred to as the volar beak ligament. Attenuation of the AOL leads to dorsal and radial subluxation of the first metacarpal base. This subluxation is exacerbated by the unyielding deforming forces exerted by the abductor pollicis longus (APL) and the adductor pollicis muscles. Over time, this altered joint kinematics results in a dramatic shift in contact mechanics, concentrating joint reaction forces onto the volar aspect of the trapezium. This eccentric loading accelerates cartilage wear, precipitates volar beak osteophyte formation, and drives progressive, end-stage osteoarthritis.
Epidemiologically, trapeziometacarpal arthrosis exhibits a striking demographic predilection, disproportionately affecting postmenopausal women. The prevalence of radiographic TMC arthritis approaches 30% in women over the age of 50, though a smaller subset will present with clinically symptomatic disease requiring surgical intervention. The etiology is considered multifactorial, encompassing genetic predisposition, hormonal variations altering ligamentous laxity, and repetitive biomechanical microtrauma associated with occupational or recreational activities. The profound functional impairment and socioeconomic burden associated with thumb basal joint arthritis necessitate a deep understanding of its patho-anatomy to guide appropriate surgical reconstruction, ranging from isolated ligament reconstruction in early-stage instability to complex interposition arthroplasty in advanced pantrapezial disease.
Detailed Surgical Anatomy and Biomechanics
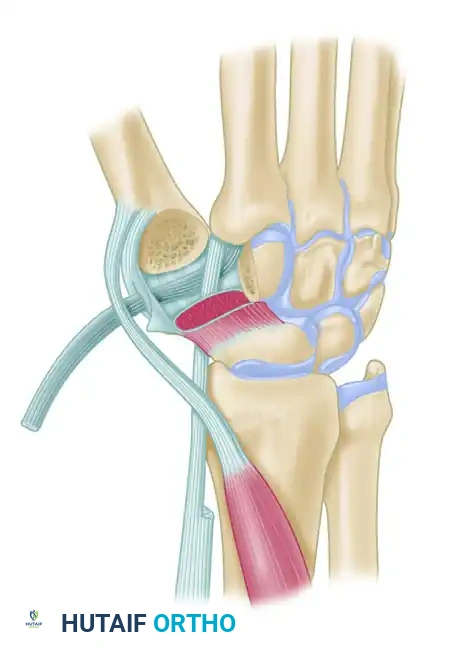
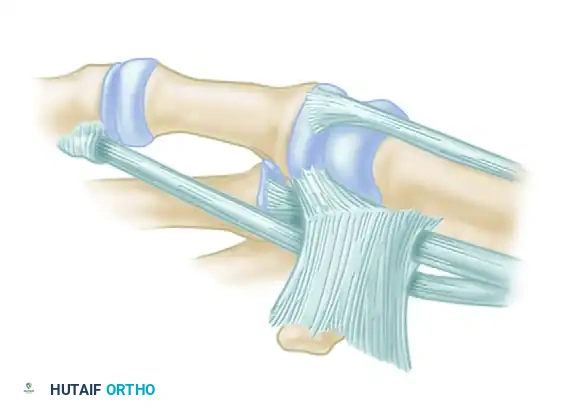
The osseous anatomy of the trapeziometacarpal joint is classically described as a saddle joint (articulatio sellaris), featuring two reciprocally concavoconvex surfaces. The distal articular surface of the trapezium is concave in the radioulnar plane and convex in the dorsovolar plane, articulating with the complementary base of the first metacarpal. This unique geometry allows for two primary degrees of freedom, while a third degree of freedom—axial rotation—is achieved passively through capsular laxity during the compound motion of opposition. This "screw-home" mechanism is essential for bringing the thumb pulp into direct contact with the fingers, but it generates immense shear forces across the articular cartilage.
Biomechanical studies have demonstrated that the joint reaction forces at the TMC joint are exponentially magnified during normal hand function. Due to the lever-arm mechanics of the thumb, a simple 1-kilogram pinch force generated at the thumb tip translates to an astonishing 12 to 13 kilograms of compressive and shear force at the basal joint. To counteract these forces, the joint relies on a robust capsuloligamentous complex. While early literature, including the foundational work by Eaton and Littler, emphasized the anterior oblique ligament (AOL) as the paramount stabilizer preventing dorsal subluxation, contemporary biomechanical investigations by Bettinger and others have identified up to 16 distinct ligaments supporting the trapeziometacarpal articulation.
Modern anatomical consensus highlights the dorsoradial ligament (DRL) as the primary restraint to dorsal dislocation, being thicker, shorter, and more cellular than the AOL. The AOL, conversely, is critical in preventing volar subluxation and excessive pronation. Furthermore, the intermetacarpal ligament (IML) and the posterior oblique ligament (POL) play vital synergistic roles in maintaining the spatial relationship between the first and second metacarpals. Surgical reconstruction must respect this complex interplay. Trapeziometacarpal ligament reconstruction aims to restore the stabilizing function of these attenuated volar and dorsal structures using a distally based strip of the flexor carpi radialis (FCR) tendon, effectively recreating a functional tether that resists the proximal and dorsal migration of the metacarpal base under dynamic load.
Exhaustive Indications and Contraindications
Surgical intervention for trapeziometacarpal arthrosis is dictated by a careful synthesis of the patient's subjective symptom severity, functional demands, clinical instability, and radiographic staging. The foundational classification systems proposed by Burton, Eaton, Littler, and Dell remain the gold standard for staging thumb carpometacarpal arthrosis and guiding the surgical algorithm. Isolated ligament reconstruction (the classic Eaton-Littler technique) is strictly indicated for patients with symptomatic hypermobility, painful subluxation, and early-stage disease (Stage I or early Stage II) where the articular cartilage remains largely pristine. In these cases, the goal is to halt the progression of eccentric wear by restoring joint kinematics.
Conversely, patients presenting with advanced disease (Stage III or IV), characterized by significant joint space narrowing, subchondral sclerosis, large osteophytes (>2 mm), and pantrapezial involvement, are not candidates for isolated ligament reconstruction. In these scenarios, the articular surface is irreversibly damaged, and stabilizing a destroyed joint will only exacerbate pain. These patients require joint-sacrificing procedures, most notably the Calandruccio modification of ligament reconstruction and tendon interposition (LRTI), complete trapeziectomy with suspensoplasty, or arthrodesis. Arthrodesis is typically reserved for young, high-demand manual laborers who require absolute stability and power pinch, provided the scaphotrapezial joint is completely free of arthritic changes.
| Indication / Contraindication | Isolated Ligament Reconstruction (Eaton-Littler) | Trapeziectomy with LRTI (Calandruccio / Burton-Pellegrini) |
|---|---|---|
| Primary Indications | Eaton Stage I & early Stage II; Symptomatic instability; Positive stress test with preserved joint space; Failed conservative management (splinting, NSAIDs, injections). | Eaton Stage III & IV; Severe joint destruction; Pantrapezial arthritis; Chronic fixed subluxation; Failed conservative management. |
| Absolute Contraindications | Eaton Stage III & IV (cartilage destruction); Pantrapezial arthritis; Active joint infection; Uncorrected carpal tunnel syndrome (relative). | Active localized or systemic infection; Medically unfit for surgery; Charcot arthropathy; Young heavy manual laborer (relative - consider arthrodesis). |
| Relative Contraindications | Scaphotrapezial-trapezoid (STT) arthritis; Severe baseline stiffness; Poor patient compliance with postoperative immobilization. | Severe proximal migration requiring extensive distraction; Concurrent profound neurological deficits affecting thumb musculature. |
| Expected Outcomes | Restoration of stability, preservation of motion, prevention of early arthrosis progression. | Excellent pain relief, maintenance of functional thumb length, reliable pinch strength, elimination of bone-on-bone crepitus. |
Clinical and Radiographic Staging
While radiographic staging is indispensable, it must be interpreted with caution. A critical clinical pearl is that radiographic severity does not always reliably correlate with a patient’s subjective symptoms. Many patients with advanced Stage IV radiographic changes function well with minimal pain, while those with subtle Stage I instability may be completely debilitated. Surgical intervention must be tailored to the patient's pain level, functional demands, and degree of clinical instability, rather than radiographs alone.
Table: Classification Systems of Thumb Carpometacarpal Arthrosis
| Stage | Eaton / Burton | Dell |
|---|---|---|
| STAGE I | No joint destruction. Joint space widened if effusion is present. Less than one-third subluxation. | Ligamentous laxity, pain, positive grind test. Dorsoradial metacarpal subluxation. |
| STAGE II | Slight decrease in joint space. Marginal osteophytes < 2 mm. May be one-third subluxation. | Symptoms with heavy use, positive grind test. Narrowed joint space, subchondral sclerosis. |
| STAGE III | Significant joint destruction with cysts and sclerosis. Osteophytes > 2 mm. Greater than one-third subluxation. | Pain with normal use, crepitus. Ulnar osteophyte, less than one-third subluxation. |
| STAGE IV | Pantrapezial degenerative changes. Involvement of multiple joint surfaces. | CMC adduction deformity, MCP joint hyperextension. May have pantrapezial arthritis. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative evaluation begins with a meticulous clinical examination. The hallmark of TMC arthritis is pain localized to the base of the thumb, exacerbated by pinch and grasp activities (e.g., opening jars, turning keys). The "grind test," performed by applying axial compression with circumduction of the first metacarpal, will elicit crepitus and sharp pain in advanced stages. For early-stage instability, the "lever test" or dorsal-volar translation stress testing is critical to assess the integrity of the AOL and DRL. Evaluation of the metacarpophalangeal (MCP) joint is equally crucial; a compensatory MCP hyperextension deformity (often >30 degrees) must be addressed concurrently (via volar capsulodesis, EPB transfer, or arthrodesis) to prevent failure of the basal joint reconstruction.
Radiographic planning requires specialized views to accurately profile the TMC and surrounding pantrapezial joints. Standard posteroanterior and lateral views of the hand are insufficient due to the 30-degree pronated posture of the thumb relative to the hand. A true anteroposterior view of the TMC joint (Robert's view), obtained with the hand in maximum pronation and the dorsal aspect of the thumb resting on the cassette, is mandatory to assess joint space narrowing and subluxation. Stress views, taken while the patient forcefully pinches the thumb and index finger together, can unmask dynamic instability characteristic of Stage I disease. Additionally, a Bett's view or a 30-degree pronated lateral view helps evaluate the scaphotrapezial-trapezoid (STT) articulation, which dictates whether a simple trapeziectomy or a more extensive resection is required.
Surgical execution demands optimal patient positioning and anesthesia. The procedure is typically performed under regional anesthesia (supraclavicular or axillary brachial plexus block) combined with intravenous sedation, providing excellent intraoperative muscle relaxation and postoperative analgesia. The patient is positioned supine with the operative arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mmHg following exsanguination with an Esmarch bandage. Fluoroscopy (C-arm) must be available and positioned either parallel to the table or coming in from the head of the bed to allow for unencumbered intraoperative imaging during bone tunnel creation and joint reduction.
Step-by-Step Surgical Approach and Fixation Technique
Eaton and Littler Trapeziometacarpal Ligament Reconstruction
This classic technique is primarily indicated for Stage I and early Stage II disease where articular cartilage is largely preserved, but symptomatic instability or painful subluxation is present. The objective is to recreate the stabilizing vector of the anterior oblique ligament using a robust autograft.
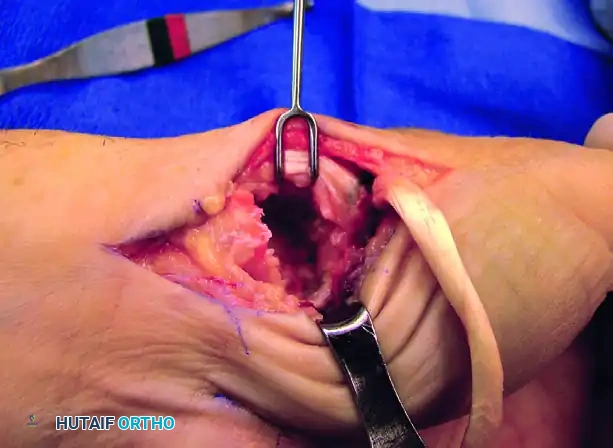
Approach and Exposure:
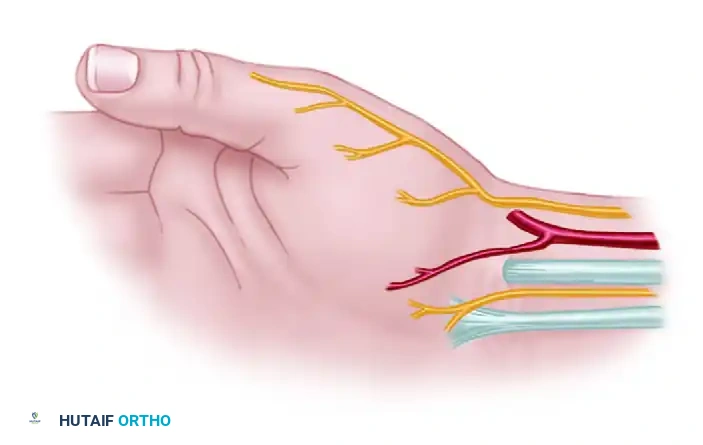
Expose the thumb carpometacarpal joint through a Wagner-type incision along the radial border of the first metacarpal. The incision should curve ulnarly within the distal wrist flexion crease, extending proximally as far as the flexor carpi radialis (FCR) tendon. Meticulous superficial dissection is absolutely critical to avoid devastating neuropathic complications. Three specific structures must be identified, mobilized, and protected with vessel loops: the superficial branch of the radial nerve (SBRN), the superficial branch of the radial artery, and the palmar cutaneous sensory branches, particularly those originating from the median nerve.
Reflect the thenar musculature (abductor pollicis brevis and opponens pollicis) extraperiosteally from the metacarpal shaft and the volar aspect of the trapezium to expose the joint capsule. Deep dissection at the proximal border of the trapezium reveals a sheet of transverse fascial fibers. These fibers form the roof over the separate fibro-osseous tunnel of the FCR. This tunnel is anatomically distinct, separated from the main carpal tunnel by a vertical septum located between the FCR and the flexor pollicis longus (FPL).
Joint Preparation and Tunnel Creation:
Incise the reflection of the transverse carpal ligament longitudinally to expose the FCR tendon. The tendon disappears distally beneath a horizontal trapezial ridge projection. Free the tendon approximately 0.5 cm distal to this point by sharp release of the overlying muscle origins. Perform a longitudinal arthrotomy of the radial capsule. This allows for thorough débridement of hypertrophic synovium, excision of marginal osteophytes, and direct inspection of the articular cartilage to confirm the absence of advanced arthrosis. Remove as much diseased synovium as possible using a rongeur.
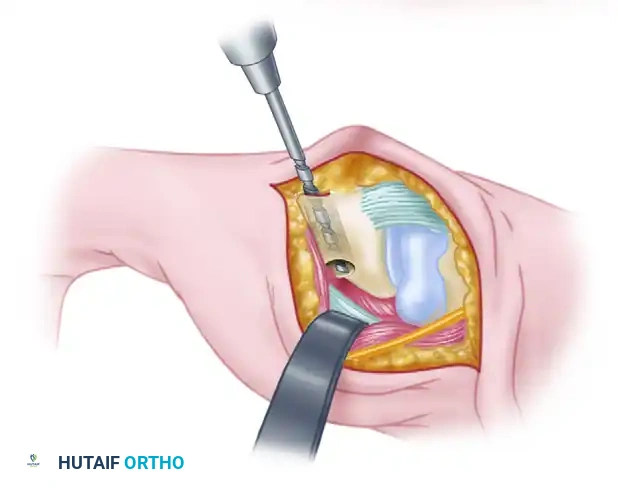
Next, create an extraarticular bone tunnel from the dorsal base of the metacarpal to the volar beak apex. The vector of this tunnel is critical: it must be in a plane strictly perpendicular to the thumb nail. Start the drill hole just distal to the dorsal base of the metacarpal, carefully positioning it between the extensor pollicis brevis (EPB) and extensor pollicis longus (EPL) tendons. Direct the drill or gouge to exit precisely at the volar beak of the metacarpal, ensuring the subchondral bone and articular surface are not breached.
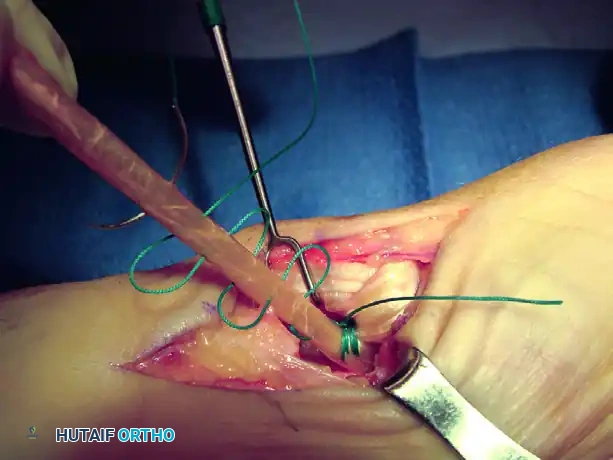
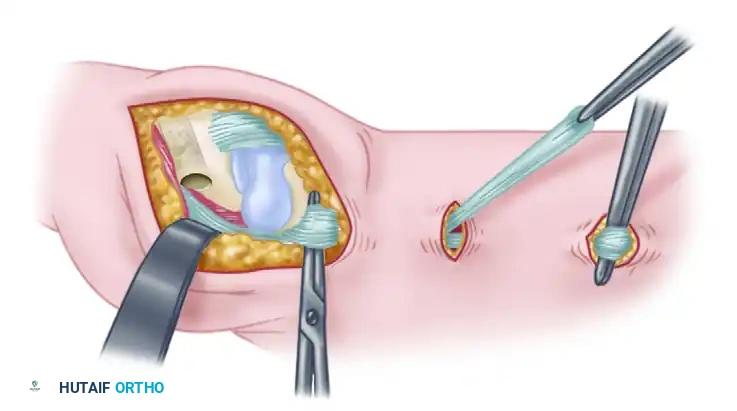
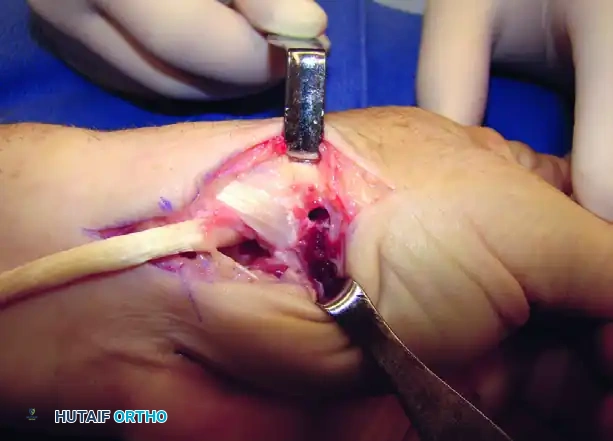
Tendon Harvest and Routing:
To obtain the "new ligament," make two transverse step-incisions over the FCR tendon—one at 3 cm and another at 6 cm proximal to the wrist crease. Split a strip comprising exactly half the width of the FCR tendon, reliably taking the radial half to preserve the structural integrity of the remaining tendon. Tunnel this strip beneath the skin bridges to emerge beyond the wrist crease, ensuring it remains in absolute continuity at its distal insertion at the base of the second metacarpal.
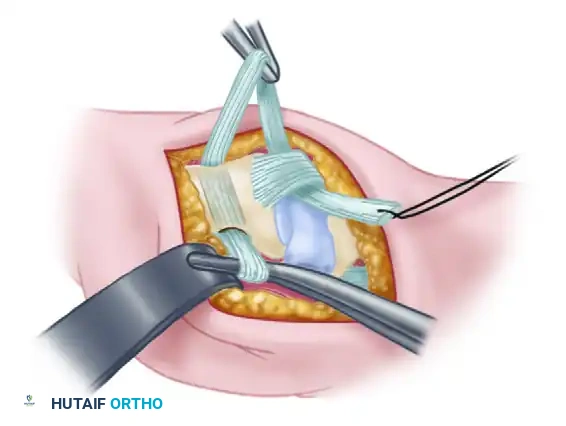
Continue the split 5 mm distal to the crest of the trapezium. Redirect the free end of the tendon strip across the crest to enter the volar portion of the previously created intramedullary channel at the thumb metacarpal beak. Draw the tendon dorsally through the metacarpal tunnel using a previously placed wire loop, Hewson suture passer, or a small curved hemostat.
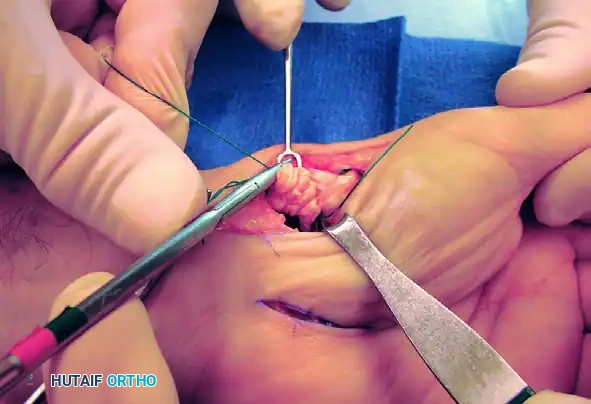
Joint Reduction and Fixation:
Accurately reduce the TMC joint under direct vision and fluoroscopic guidance. Hold the thumb in extension and palmar abduction, firmly seating the metacarpal base against the deep facet of the trapezium to eliminate dorsal subluxation. Insert a 0.045-inch or 0.062-inch Kirschner wire (K-wire) from the dorsum of the metacarpal into the trapezium to rigidly maintain the reduction.
Surgical Warning: It is imperative to ensure the K-wire does not impale the intramedullary portion of the tendon strip. Impalement would compromise the ability to appropriately tension the graft and could lead to tendon necrosis or premature rupture.
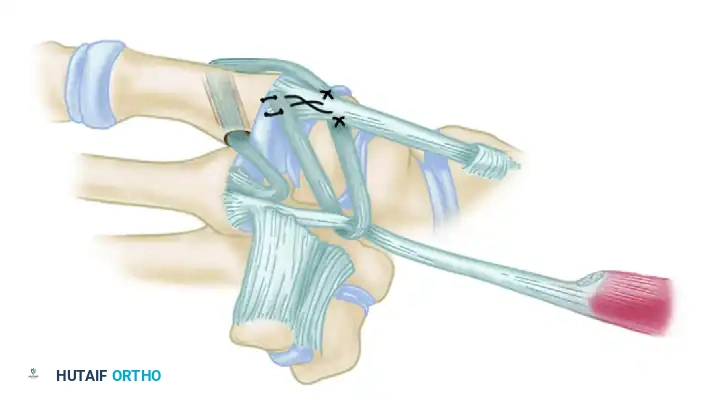
With the joint stabilized, draw the tendon strip taut. Verify that it courses directly from its emergence at the FCR tunnel to the volar beak of the metacarpal, effectively recreating the anatomical vector of the anterior oblique ligament.

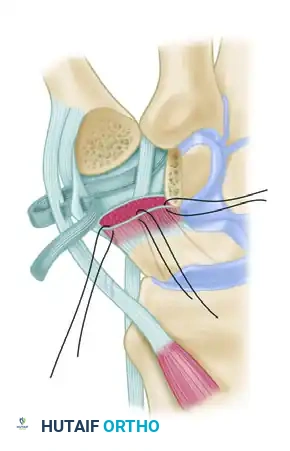
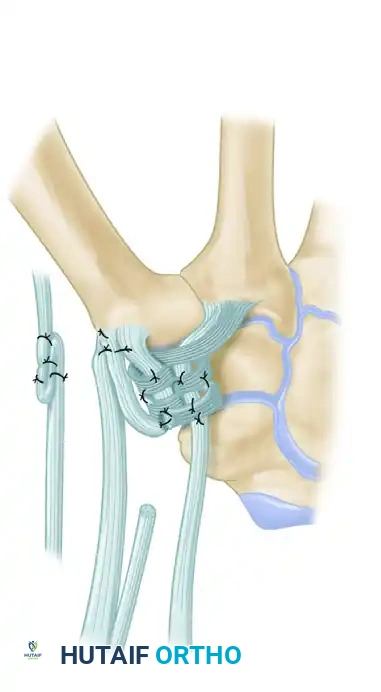
Final Ligament Weaving:
Suture the taut tendon to the dorsal periosteum of the metacarpal using non-absorbable 2-0 or 3-0 sutures. Route the remainder of the tendon proximally across the dorsal basal joint capsule to provide dorsal capsular reinforcement, passing it beneath the EPB and APL insertions. Suture the strip under tension to the APL bony insertion. Pass the remaining tail beneath or through a short split in the intact FCR tendon just proximal to the trapezium. Route it back across the radial margin of the joint to insert into the metacarpal periosteum. Suture the tendon securely at every point where its direction changes to lock the tension into the construct.
Technique Modification: Calandruccio Interposition Arthroplasty (LRTI)
For patients with Stage III or IV disease presenting with significant joint destruction and pantrapezial arthritis, isolated ligament reconstruction is insufficient and will lead to persistent pain. The Calandruccio modification, a variation of the Burton-Pellegrini technique, combines complete trapeziectomy with ligament reconstruction and tendon interposition (LRTI).
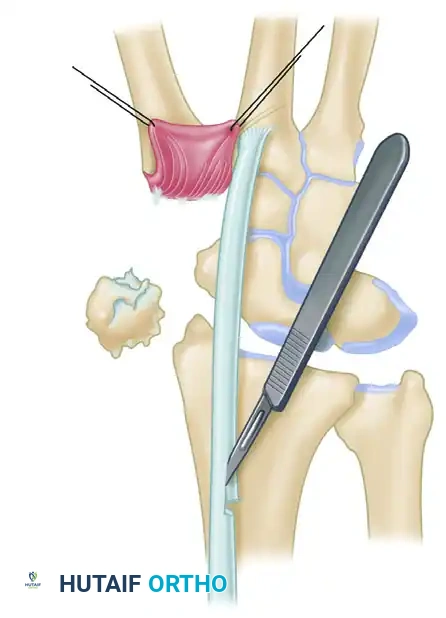
Trapezial Excision and Metacarpal Preparation:
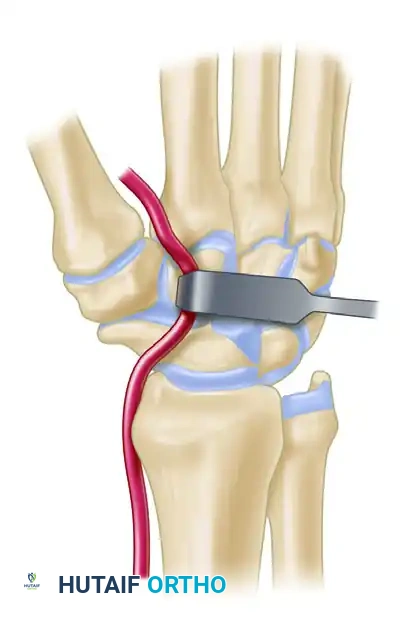
After exposing the joint through a similar volar-radial incision and reflecting the thenar muscles, perform a complete excision of the trapezium. This can be done piecemeal using a rongeur or en bloc using an osteotome, depending on the degree of osteophyte formation. Extreme care must be taken to protect the underlying FCR tendon, which lies immediately deep to the medial trapezial facet. Once the trapezium is removed, inspect the base of the thumb metacarpal. Using a 4-mm rough burr, create holes through the base of the thumb metacarpal, directing them proximally and radially. Connect these holes using a series of curets (usually up to a No. 2) to form a smooth, continuous tunnel that will accommodate the tendon graft.

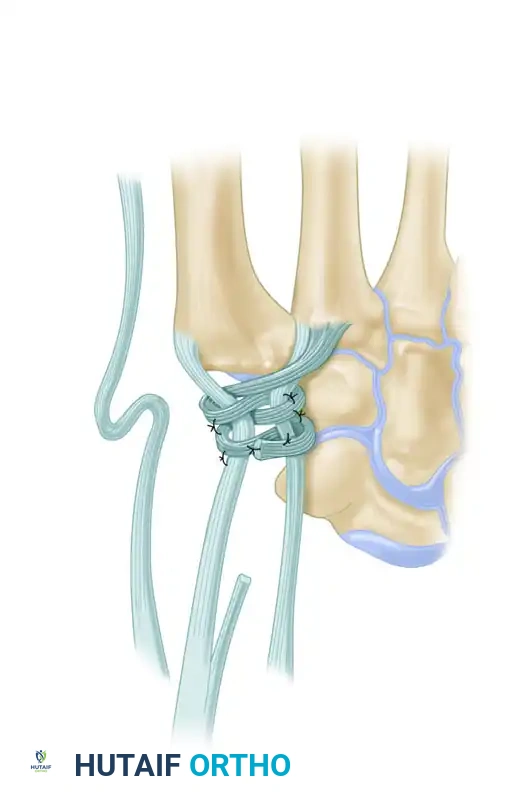
Tendon Routing and Suspensoplasty:
Pass the harvested FCR tendon strip through the newly created bone tunnel from volar to dorsal. Hold the tendon perpendicular to the index metacarpal shaft. The critical step in this procedure is the suspensoplasty, designed to prevent the proximal migration (subsidence) of the thumb metacarpal into the trapezial void. Approximate the index and thumb metacarpal bases by applying slight ulnarly directed pressure on the thumb metacarpal while distracting it distally. Firmly secure the FCR tendon to the APL bony insertion or the dorsal periosteum using robust 2-0 braided nonabsorbable sutures.
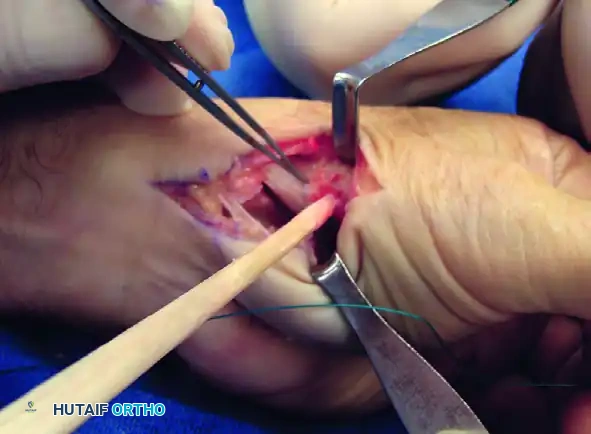

Intermetacarpal Securing and Interposition:
Pass the remaining FCR tendon between the thumb and index metacarpal bases, effectively creating a sling. Secure it to itself with the same nonabsorbable suture. The residual tail of the tendon is then folded upon itself to create an "anchovy" or biologic spacer, which is packed into the trapezial void. This interposition serves to maintain the joint space, provide a smooth gliding surface, and prevent bony impingement between the metacarpal base and the scaphoid.
Complications, Incidence Rates, and Salvage Management
Despite the high success rates of both isolated ligament reconstruction and LRTI, complications can and do occur. A comprehensive understanding of these pitfalls is essential for both prevention and salvage management. The most devastating complications are often iatrogenic, related to the surgical approach rather than the biomechanical construct itself.
Injury to the superficial branch of the radial nerve (SBRN) or the lateral antebrachial cutaneous nerve is the most frequent source of postoperative morbidity. Neuroma formation in this region is notoriously difficult to treat and can result in severe, chronic debilitating pain that overshadows any functional improvement gained from the joint reconstruction. Meticulous soft-tissue handling, the use of magnification loupes, and avoiding aggressive retraction are paramount.
Subsidence of the first metacarpal is a known radiographic phenomenon following trapeziectomy and LRTI. While some degree of proximal migration is expected and often well-tolerated clinically, severe subsidence can lead to impingement against the scaphoid, resulting in recurrent pain and weakness. This highlights the importance of a meticulous suspensoplasty and adequate K-wire fixation during the healing phase. Complex Regional Pain Syndrome (CRPS) Type I is another severe complication, presenting with disproportionate pain, swelling, stiffness, and vasomotor changes. Early recognition and aggressive multimodal intervention are required.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management |
|---|---|---|---|
| SBRN Neuroma / Neuritis | 5% - 10% | Meticulous superficial dissection; avoid self-retaining retractors on skin edges; identify and protect nerve branches. | Gabapentinoids; localized steroid injections; surgical exploration with nerve capping or targeted muscle reinnervation (TMR) for established neuromas. |
| Metacarpal Subsidence | 15% - 30% (Radiographic) | Robust suspensoplasty; adequate tensioning of FCR graft; K-wire fixation for 4-6 weeks; avoiding early heavy loading. | Often asymptomatic. If symptomatic (scaphoid impingement), consider revision suspension, distraction lengthening, or arthrodesis. |
| Complex Regional Pain Syndrome (CRPS) | 2% - 5% | Adequate postoperative analgesia; early mobilization of uninvolved digits; Vitamin C prophylaxis (500mg/day for 50 days post-op). | Aggressive hand therapy; stellate ganglion blocks; oral corticosteroids; neuropathic pain modulators. |
| Pin Tract Infection | 3% - 7% | Sterile pin insertion technique; avoiding thermal necrosis during drilling; meticulous pin site care. | Oral antibiotics; early pin removal if infection tracks deep or threatens joint space. |
| FCR Tendon Rupture | < 2% | Harvesting exactly 50% of tendon; avoiding K-wire impalement of graft; smooth edges on bone tunnels. | Conservative management (often well-tolerated); revision reconstruction with palmaris longus or allograft if instability recurs. |
Phased Post-Operative Rehabilitation Protocols
The success of trapeziometacarpal ligament reconstruction and arthroplasty is heavily dependent on a structured, phased postoperative rehabilitation protocol. The delicate balance between protecting the healing soft-tissue construct and preventing debilitating joint stiffness requires close collaboration between the orthopedic surgeon and a certified hand therapist (CHT).
Phase I: Immobilization and Protection (Weeks 0-4)
Immediately postoperatively, the patient is placed in a bulky, well-padded thumb spica splint or cast. The thumb is positioned in palmar abduction and slight extension to minimize tension on the reconstructed ligaments and suspensoplasty. The interphalangeal (IP) joint of the thumb and the metacarpophalangeal (MCP) joints of the fingers are left free to allow for immediate active range of motion, which is critical for edema control and preventing tendon adhesions. The K-wire, if placed, provides rigid internal immobilization. During this phase, strict elevation and digital motion are emphasized.
**Phase II: Early Controlled Motion (
Clinical & Radiographic Imaging Archive