Thumb Opposition & Adduction Restoration: Surgical Techniques
Key Takeaway
Restoration of thumb opposition and adduction is critical in managing median and ulnar nerve palsies. The abductor digiti quinti (ADQ) transfer, popularized by Littler and Cooley, provides an excellent biomechanical substitute for the abductor pollicis brevis without requiring a pulley. For adductor paralysis, techniques such as the Boyes brachioradialis transfer or flexor digitorum sublimis routing effectively restore power pinch, mitigating compensatory deformities like Froment and Jeanne signs.
Comprehensive Introduction and Patho-Epidemiology
The human thumb represents a biomechanical marvel and the evolutionary cornerstone of advanced prehension, responsible for approximately 40% to 50% of overall hand function. Its unique spatial orientation, governed by the highly specialized trapeziometacarpal (CMC) joint, allows for complex spatial positioning primarily driven by the synergistic actions of opposition and adduction. When peripheral nerve injuries—specifically median and ulnar nerve palsies—compromise the intrinsic musculature of the thenar web, the resulting functional deficit is profound and immediately debilitating. Patients suffering from these deficits lose the ability to perform power pinch, precision handling, and forceful grasp, leading to severe occupational limitations and a drastic reduction in their activities of daily living.
The patho-epidemiology of intrinsic thumb paralysis is diverse, encompassing traumatic nerve lacerations, severe compressive neuropathies, brachial plexus avulsions, and systemic neuropathic conditions such as leprosy in endemic regions. High median nerve injuries eradicate the thenar musculature (abductor pollicis brevis, opponens pollicis, and the superficial head of the flexor pollicis brevis), completely abolishing true opposition. Conversely, ulnar nerve lesions paralyze the adductor pollicis, the deep head of the flexor pollicis brevis, and the first dorsal interosseous, obliterating the power pinch. When combined median and ulnar nerve palsies occur, the thumb is rendered entirely "intrinsic minus," resting in a non-functional posture of external rotation, adduction, and supination, completely incapable of interacting with the ulnar digits.
Surgical restoration of these critical functions requires a profound understanding of thumb kinematics, precise vector mechanics, and meticulous soft-tissue handling. The reconstructive surgeon must operate within a narrow therapeutic window; if nerve reconstruction or repair fails to reinnervate the target motor endplates within 12 to 18 months, irreversible muscle atrophy and fibrosis ensue, mandating tendon or muscle transfers. This masterclass details the premier tendon and muscle transfer techniques utilized to restore thumb opposition (via the Abductor Digiti Quinti transfer) and thumb adduction (via Flexor Digitorum Superficialis, Brachioradialis, or Extensor Carpi Radialis Brevis transfers).
The overarching goal of these complex reconstructive procedures is not merely the anatomical repositioning of tendons, but the dynamic restoration of the thumb's kinematic chain. Achieving this requires the surgeon to meticulously balance the forces acting across the CMC, metacarpophalangeal (MCP), and interphalangeal (IP) joints. Failure to respect the delicate interplay between extrinsic power and intrinsic stabilization will inevitably result in secondary deformities, transfer attenuation, and ultimate functional failure.
Detailed Surgical Anatomy and Biomechanics
To accurately reconstruct thumb motion, the orthopedic surgeon must first possess an intimate understanding of the planes of movement relative to the palm and the intricate articular geometry of the trapeziometacarpal joint. The CMC joint is a highly incongruous biconcave-biconvex saddle joint that permits movement in two primary planes, while capsular laxity allows for a crucial third degree of freedom: axial rotation.
As illustrated in the biomechanical model above, the fundamental motions of the thumb ray are defined relative to the plane of the palm:
* Adduction and Abduction: Occur in a plane perpendicular to the palm. Abduction moves the thumb away from the palm anteriorly, while adduction returns it.
* Flexion and Extension: Occur in a plane parallel to the palmar surface, moving the thumb across the palm toward the ulnar border.
* Pronation and Supination: Represent the longitudinal rotation of the thumb metacarpal around its own axis, an essential component for pulp-to-pulp contact.
* Opposition: A complex, multi-planar composite movement consisting of abduction, flexion, and pronation of the first metacarpal, coupled with flexion and abduction of the proximal phalanx, and extension of the distal phalanx.
When the adductor pollicis is paralyzed (typically due to a low or high ulnar nerve palsy), the biomechanical equilibrium of the thumb ray is catastrophically disrupted. The adductor pollicis normally provides a massive transverse vector force that pulls the first metacarpal toward the third metacarpal, stabilizing the MCP joint against the powerful extrinsic flexors during pinch. In its absence, the patient attempts to compensate during power pinch by hyper-recruiting the available extrinsic musculature, fundamentally altering the kinematic chain.
This compensatory mechanism manifests clinically as two classic, pathognomonic signs that every hand surgeon must recognize and understand biomechanically:
1. Froment Sign: The interphalangeal (IP) joint of the thumb becomes hyperflexed as the flexor pollicis longus (FPL) attempts to substitute for the paralyzed adductor pollicis to produce pulp pinch. Because the FPL lacks a transverse vector, it can only generate pinch force by acutely flexing the terminal phalanx against the index finger.
2. Jeanne Sign: The metacarpophalangeal (MCP) joint becomes hyperextended secondary to unbalanced extensor forces (Extensor Pollicis Longus and Extensor Pollicis Brevis) acting without the stabilizing volar flexion moment normally provided by the intrinsic thenar and adductor muscles.
The presence of a severe Jeanne sign indicates a profound intrinsic minus status at the MCP joint, characterized by volar plate attenuation and dorsal capsular contracture. When planning an adductor transfer, the surgeon must ensure the selected transfer vector provides a stabilizing flexion moment at the MCP joint to prevent persistent hyperextension during pinch. In cases of severe, fixed MCP hyperextension, a concomitant MCP joint arthrodesis or volar capsulodesis may be mandatory to provide a stable terminal post for the newly transferred tendon.
Exhaustive Indications and Contraindications
The decision to proceed with a tendon or muscle transfer for thumb opposition or adduction requires a rigorous preoperative assessment. The fundamental prerequisites for any tendon transfer must be met: the donor muscle must possess adequate strength (Medical Research Council Grade 4 or 5), sufficient excursion to replicate the lost function, and an expendable native function. Furthermore, the soft tissue bed through which the transfer will be routed must be free of extensive scarring to allow for unhindered gliding.
A critical, non-negotiable prerequisite for opposition and adduction transfers is the presence of full, passive range of motion at the trapeziometacarpal joint. A stiff, contracted, or arthritic CMC joint will completely negate the dynamic pull of a transferred tendon. If a first web space contracture exists, it must be surgically released (via Z-plasty, dorsal rotational flaps, or release of the adductor fascia) prior to or concurrently with the tendon transfer. Transferring a muscle against a fixed skeletal or fascial contracture will inevitably result in transfer failure and attenuation.
The selection of the specific donor motor depends entirely on the pattern of neurological loss, the availability of expendable donors, and the specific vector required to restore the disrupted kinematic chain. The Abductor Digiti Quinti (ADQ) transfer is highly favored in congenital hypoplasia, median nerve palsies where extrinsic flexors must be preserved, and severe trauma where the palmar fascia is intact. Conversely, FDS and wrist extensor transfers are favored when massive power is required for adduction reconstruction.
| Surgical Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| ADQ Transfer (Littler & Cooley) | Isolated median nerve palsy; Congenital thenar hypoplasia; Brachial plexus injuries sparing the ulnar nerve; Need for thenar cosmetic bulk. | Ulnar nerve palsy (ADQ paralyzed); Fixed CMC joint contracture; Severe palmar scarring preventing tunneling. | Pre-existing little finger dysfunction; Marginal ulnar nerve function (MRC Grade 3). |
| FDS Transfer (Groves & Goldner) | Combined median/ulnar nerve palsy; Need for simultaneous opposition and adduction restoration; High demand for power pinch. | Median nerve palsy affecting FDS to ring/middle fingers; Stiff ring finger PIP joint. | Occupations requiring independent, powerful ring finger flexion; FDS absence. |
| ECRB / Brachioradialis (Boyes/Brand) | Isolated ulnar nerve palsy requiring massive adduction power; High radial nerve intact with ulnar loss. | Radial nerve palsy; Lack of available tendon graft material (e.g., absent Palmaris Longus). | Severe dorsal wrist scarring (for Brand); Volar web space scarring (for Boyes). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the bedrock of successful tendon transfer surgery. The surgeon must meticulously map the functional status of every muscle in the hand and forearm, documenting the MRC grade. The principle of "tissue equilibrium" must be respected; the hand must be soft, supple, and free of acute edema or active inflammation. Pre-operative hand therapy is often instituted for 6 to 12 weeks to maximize passive range of motion, soften scars with silicone and massage, and begin motor re-education of the intended donor muscle.
When templating the transfer, the surgeon must calculate the required excursion and tension. The normal abductor pollicis brevis requires approximately 2 to 3 cm of excursion, while the adductor pollicis requires roughly 3 to 4 cm. The donor muscle must match or exceed these requirements. For example, the FDS has an excursion of 5 to 7 cm, making it an excellent, powerful donor, whereas the Brachioradialis has a shorter excursion (approx. 3 cm) and must be mobilized extensively proximal to its fascial investments to achieve adequate amplitude.
Vector analysis is equally critical. For opposition, the ideal vector pulls from the pisiform toward the thumb MCP joint, mimicking the APB. For adduction, the vector must pull transversely across the palm, mimicking the transverse head of the adductor pollicis. The surgeon must plan the exact location of the anatomical or constructed pulleys to achieve these precise mechanical lines of pull, knowing that a deviation of even a few degrees can result in a transfer that produces flexion or extension rather than true opposition or adduction.
Patient positioning is standardized for these procedures. The patient is placed supine with the operative extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Regional anesthesia (supraclavicular or axillary block) is highly preferred, as it provides excellent intraoperative vasodilation and profound postoperative analgesia, which prevents the patient from inadvertently firing antagonist muscles and rupturing the transfer during emergence from anesthesia. The surgeon operates seated, utilizing loupe magnification (typically 2.5x to 3.5x) and a headlight to ensure meticulous identification of delicate neurovascular pedicles, particularly during the ADQ transfer.
Step-by-Step Surgical Approach and Fixation Technique
Muscle Transfer (Abductor Digiti Quinti) to Restore Opposition
When standard motor units (such as the FDS or Extensor Indicis Proprius) are unavailable due to multi-nerve trauma, brachial plexus injury, or when they must be preserved for other reconstructive priorities, the Abductor Digiti Quinti (ADQ) muscle transfer, originally described by Littler and Cooley, is an elegant and highly effective solution. This transfer is unique because it utilizes a whole muscle belly rather than just a tendon, requiring meticulous microsurgical tissue handling.
The ADQ is an exceptional substitute for the paralyzed abductor pollicis brevis (APB) due to its remarkable biomechanical match. Its muscle mass, cross-sectional area, and excursion are nearly identical to those of the APB. Furthermore, unlike the FDS or EIP transfers, the ADQ transfer does not require the creation of a fascial or ligamentous pulley. Its anatomical origin on the pisiform provides an ideal, direct line of pull toward the thumb MCP joint. Aesthetically, the bulk of the transferred ADQ muscle belly fills the hollow space left by the wasted thenar muscles, significantly improving the cosmetic appearance of the paralyzed hand.
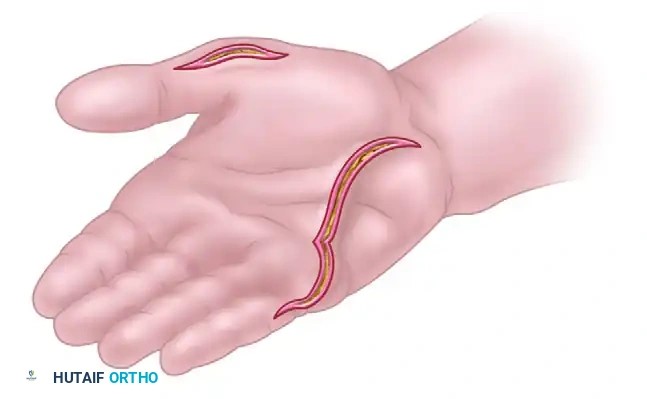
1. Incision and Exposure
The procedure begins with a carefully planned curved palmar incision along the radial border of the abductor digiti quinti muscle belly. This incision should extend from the proximal side of the pisiform, coursing distally along the hypothenar eminence to the ulnar border of the little finger at the level of the MCP joint.
The skin flaps are elevated with full-thickness subcutaneous fat to preserve the subdermal vascular plexus. The hypothenar fascia is incised, and the ADQ muscle belly is exposed. The surgeon must be cautious not to dissect too deeply on the radial aspect of the muscle to avoid injuring the ulnar neurovascular bundle as it passes through Guyon's canal.
2. Distal Mobilization
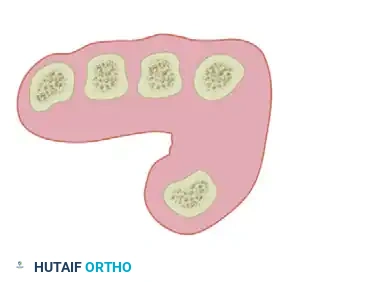
The distal aspect of the ADQ is identified, and both of its tendinous insertions are carefully freed. The muscle possesses a bifurcated insertion: one slip attaches to the ulnar aspect of the extensor expansion of the little finger, and the more robust slip attaches to the ulnar base of the proximal phalanx. Both slips are sharply detached from the bone and extensor hood, preserving as much tendinous length as possible to facilitate later weaving into the thumb.
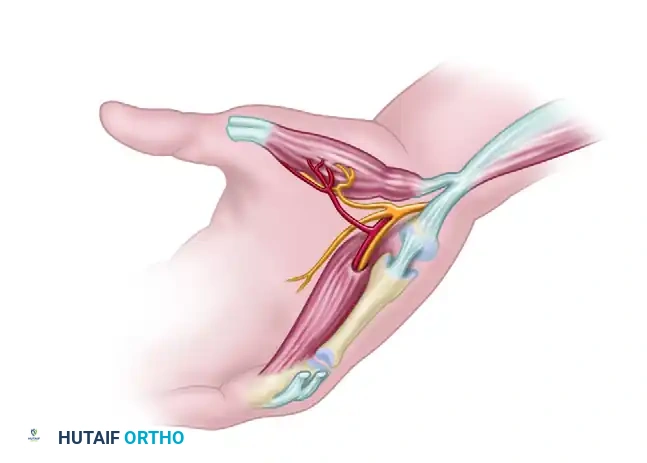
3. Neurovascular Isolation
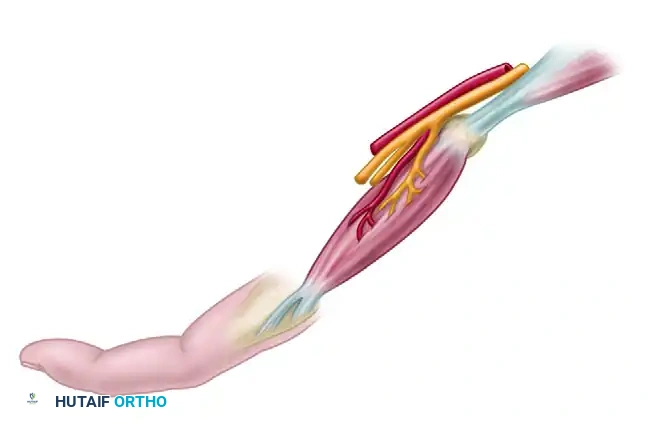
The muscle is then carefully lifted from its fascial compartment, working from distal to proximal. This is the most critical and perilous step of the procedure: the identification and preservation of the ADQ neurovascular bundle. This bundle, comprised of branches from the deep ulnar nerve and ulnar artery, enters the muscle on its deep, proximal-radial surface.

The surgeon must isolate the bundle with extreme care, utilizing blunt dissection and bipolar electrocautery for any competing small vessels. The venous drainage is particularly fragile; venous congestion due to twisting or stretching of the venae comitantes is a primary cause of transfer failure and muscle necrosis.
The neurovascular pedicle must be visualized circumferentially. Any fascial bands tethering the pedicle must be meticulously released to allow the muscle to pivot without placing tension on the vessels or the motor nerve branch.
4. Proximal Release
Once the pedicle is secure, the origin of the muscle is partially freed from the pisiform bone. A crucial technical point described by Littler is to retain the muscle's origin on the flexor carpi ulnaris (FCU) tendon expansion. This retained attachment preserves the proximal microvascular blood supply and provides a dynamic, stable anchor point for the transfer, effectively utilizing the FCU to augment the power of the transferred ADQ.
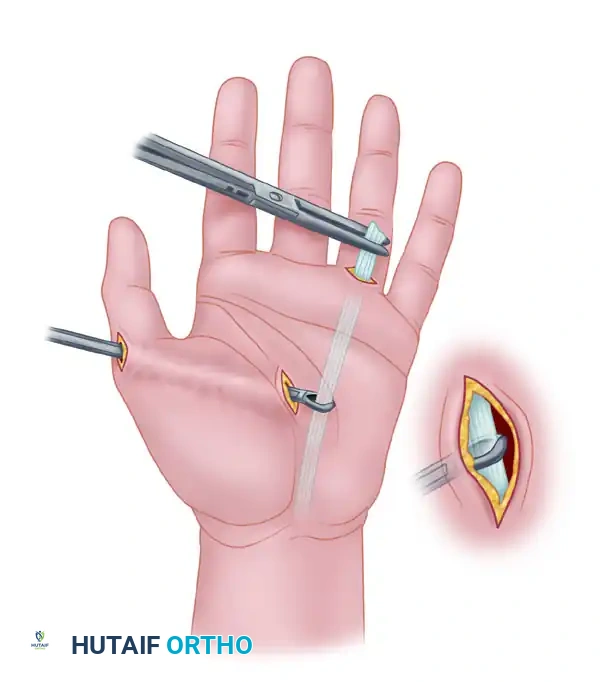
5. Subcutaneous Tunneling
A second curved incision is made on the radial border of the thenar eminence, exposing the insertion footprint of the paralyzed APB. Using blunt dissecting scissors, a wide subcutaneous pocket is created across the palm, connecting the hypothenar and thenar incisions. The tunnel must be extremely capacious—easily accommodating two fingers—to prevent any compression of the transposed muscle belly or its delicate neurovascular pedicle.
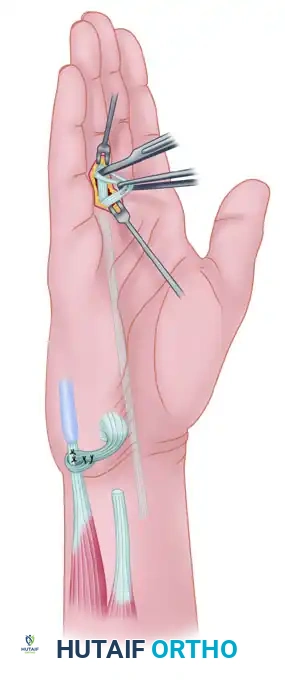
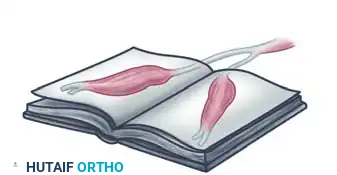
6. Muscle Transposition
The mobilized ADQ muscle is then gently folded over approximately 170 degrees. Littler famously described this elegant maneuver as turning the muscle "like a page of a book."
A passing suture is placed through the distal tendinous slips of the ADQ, and the folded muscle is passed subcutaneously through the prepared palmar pocket to the thumb incision. The surgeon must visually confirm that the muscle belly is not twisted during this passage.

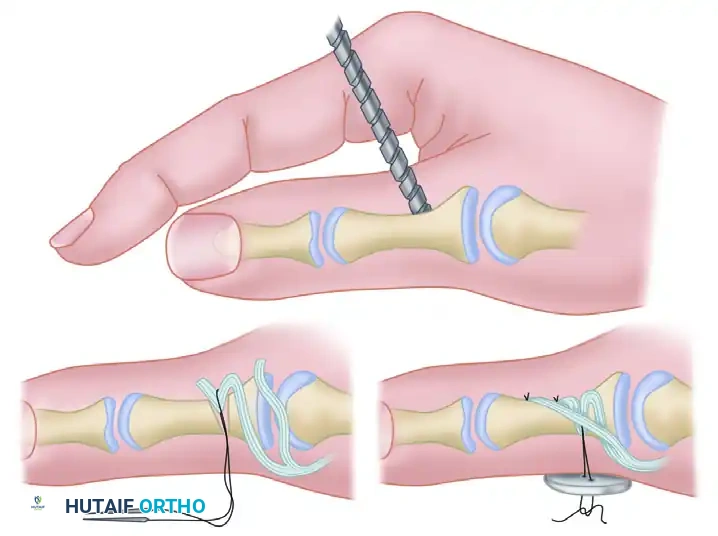
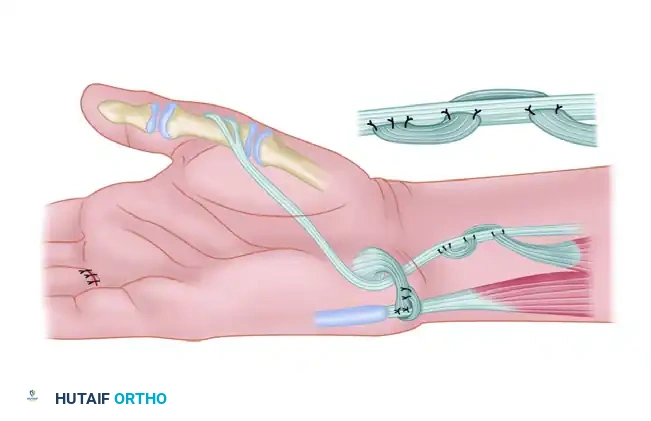
7. Insertion and Tensioning
The two tendinous insertions of the ADQ are interwoven into the insertion footprint of the abductor pollicis brevis and the radial lateral band of the thumb using a Pulvertaft weave or strong mattress sutures (e.g., 3-0 braided non-absorbable). Tension must be set with the thumb held in full palmar abduction and opposition, and the wrist in neutral to slight flexion.
Throughout the transposition and suturing process, the surgeon must continuously verify that the neurovascular pedicle is neither kinked, stretched, nor compressed. Undue tension will lead to ischemic necrosis of the transferred muscle, rendering the procedure a catastrophic failure.
Restoration of Adduction of the Thumb
Isolated loss of thumb adduction severely compromises key pinch strength, reducing it by up to 70-80%. While opposition transfers (like the ADQ or FDS to APB) restore the spatial positioning of the thumb for precision handling, they do not provide the sheer power required for forceful adduction against the index finger during key pinch.
If adduction alone is absent (as in an isolated low ulnar nerve palsy), restoring thumb abduction is unnecessary. However, the adductor transfer must often be combined with a procedure to restore index finger abduction (e.g., ECRB to first dorsal interosseous transfer) to provide a stable, rigid post for the thumb to pinch against. Without a stable index finger, the powerful new adductor transfer will simply push the index finger into ulnar deviation, failing to generate effective pinch force.
1. The Boyes Transfer (Brachioradialis or ECRB)
If a strong, expendable wrist motor is available, the brachioradialis or one of the radial wrist extensors (ECRL or ECRB) can be utilized. Because these muscles lack sufficient excursion and length to reach the thumb directly, they must be lengthened by a free tendon graft (often palmaris longus, plantaris, or a strip of fascia lata).

The lengthened tendon is routed palmarward through the third intermetacarpal space and carried across the deep palm to be inserted into the tendon of the adductor pollicis. This specific routing provides a direct, transverse line of pull that perfectly mimics the transverse head of the adductor pollicis, generating massive key pinch power.
2. The Brand Transfer
An alternative strategy utilizes the extensor carpi radialis brevis (ECRB) routed dorsally. The ECRB is detached from its insertion on the third metacarpal base, prolonged with a free tendon graft, and routed deep to the finger extensors.

It is then passed through the second intermetacarpal space to provide an adduction vector. This dorsal routing avoids the deep palmar structures, which is advantageous if the palm is heavily scarred from previous trauma.
3. The Royle-Thompson / Groves & Goldner Transfer (FDS Routing)
If both adduction and opposition are absent (combined median and ulnar palsy), a single tendon transfer can be ingeniously modified to restore both functions simultaneously. By locating the pulley more distally (using a window in the transverse carpal ligament or the palmar fascia rather than the pisiform), the transfer vector provides a combined moment of opposition and adduction.
The technique described by Groves and Goldner utilizes the Flexor Digitorum Superficialis (FDS) of the ring finger. This is often combined with an FCU to ECU transfer to stabilize the wrist and prevent the radial deviation that occurs when powerful flexors are recruited for pinch.
1. Incisions and Exposure (FDS Transfer)
The procedure requires multiple incisions. Two primary incisions are made at the wrist: one volar (over the carpal tunnel) and one ulnar (over the FCU).
Through the volar incision, the FDS tendon to the ring finger is identified and exposed, along with the FCU tendon. Through the ulnar incision, the extensor carpi ulnaris (ECU) is exposed for the optional stabilizing tenodesis.
2. Wrist Stabilization (Optional but Recommended)
To prevent destabilizing radial deviation during forceful pinch, the FCU tendon is divided approximately 4 cm proximal to its insertion on the pisiform. The free end of the distal segment is routed dorsally and sutured to the ECU tendon. This tenodesis provides a static checkrein against radial deviation.
3. FDS Harvest
The FDS tendon to the ring finger is exposed through a transverse incision at the proximal flexor crease of the digit. The tendon is identified, and its two slips are divided just proximal to Camper's chiasm to maximize length while preserving the FDP tendon's function.
4. Proximal Delivery and Routing
The divided FDS tendon is drawn proximally into the volar wrist wound. The surgeon must ensure that no lumbrical muscle belly is dragged into the carpal tunnel, which could
Clinical & Radiographic Imaging Archive