Thumb Metacarpophalangeal Joint Reconstruction in Rheumatoid Arthritis
Key Takeaway
Thumb metacarpophalangeal (MCP) joint reconstruction in rheumatoid arthritis aims to restore stability, alleviate pain, and correct deformity. The Inglis technique involves dorsal synovectomy, preservation of collateral ligaments, and meticulous reattachment of the extensor pollicis brevis and intrinsic muscles to rebalance the joint. When joint destruction is severe, silicone implant arthroplasty or arthrodesis may be indicated, depending on bone stock, capsuloligamentous integrity, and the status of the adjacent interphalangeal and carpometacarpal joints.
Comprehensive Introduction and Patho-Epidemiology
Rheumatoid arthritis (RA) is a systemic autoimmune disorder that profoundly and predictably affects the hand and wrist, with the thumb being involved in up to 70% of the patient population. Because the thumb is responsible for approximately 40% to 50% of overall hand function—facilitating precision pinch, key pinch, and power grip—preserving its stability, mobility, and painless function is a paramount objective in rheumatoid reconstructive surgery. The metacarpophalangeal (MCP) joint is frequently the epicenter of pathologic changes in the rheumatoid thumb, acting as the primary locus of synovial hypertrophy that leads to predictable, cascading patterns of biomechanical collapse. Understanding the patho-epidemiology of these deformities is essential for the orthopedic surgeon, as the progression of the disease dictates the timing and nature of surgical intervention.
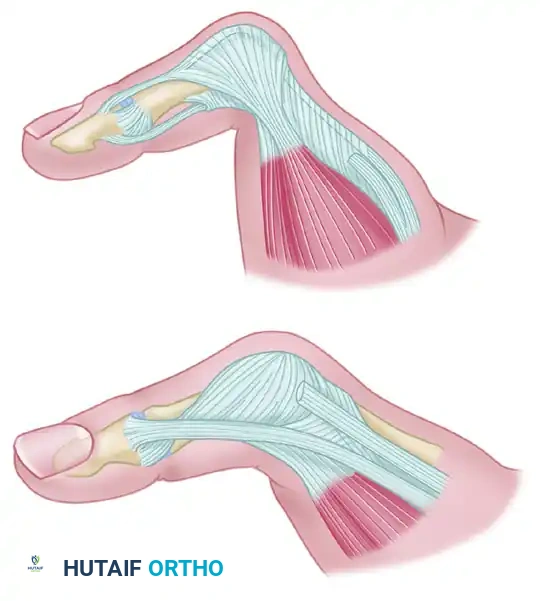
The most common deformity encountered in the rheumatoid thumb is the Nalebuff Type I, or boutonnière, deformity. This classic presentation is characterized by MCP joint flexion and secondary interphalangeal (IP) joint hyperextension. The pathogenesis is initiated by aggressive, proliferative synovial hypertrophy (pannus) within the MCP joint. This pannus enzymatically degrades articular cartilage and mechanically distends the dorsal capsule, leading to the progressive attenuation and eventual rupture of the insertion of the extensor pollicis brevis (EPB) tendon at the base of the proximal phalanx. As the primary extensor of the MCP joint is compromised, a profound muscular imbalance ensues, setting the stage for rapid structural deterioration.
As the EPB becomes detached and retracts proximally, the dorsal extensor hood stretches and loses its structural integrity. This laxity allows the extensor pollicis longus (EPL) tendon to subluxate ulnarly and volarly, slipping below the axis of rotation of the MCP joint. Concurrently, the intrinsic muscles—specifically the abductor pollicis brevis (APB) radially and the adductor pollicis ulnarly—migrate volarly. Consequently, these powerful muscles transition from being dynamic stabilizers of the joint to active flexors, exacerbating the flexion deformity at the MCP joint. The reciprocal hyperextension at the IP joint occurs due to the increased tension on the EPL as it is displaced, combined with the volar subluxation of the proximal phalanx which functionally shortens the path of the flexor pollicis longus (FPL).
The key to successful rheumatoid thumb reconstruction lies in addressing the entire kinematic chain. The status of the carpometacarpal (CMC) and IP joints must be meticulously evaluated before intervening at the MCP joint. A fused or stiff IP joint often necessitates motion preservation (arthroplasty) at the MCP joint to maintain functional dexterity, whereas a severely unstable or subluxated CMC joint must be addressed prior to or concurrently with MCP reconstruction. Failure to recognize and treat adjacent joint pathology will inevitably lead to the failure of the MCP joint reconstruction, as abnormal biomechanical forces will rapidly compromise the surgical repair.
Detailed Surgical Anatomy and Biomechanics
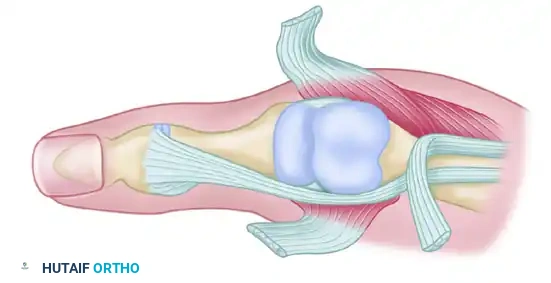
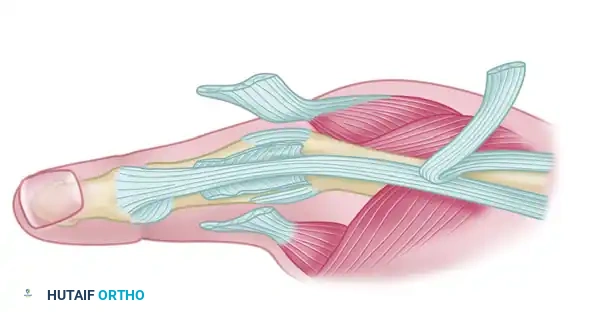
A thorough, three-dimensional understanding of the dorsal apparatus and the intrinsic musculature of the thumb is mandatory for the reconstructive hand surgeon. The extensor mechanism of the thumb is a complex, delicate interplay of extrinsic tendons and intrinsic muscle expansions. The extensor pollicis brevis (EPB) originates from the posterior surface of the radius and the interosseous membrane, traveling through the first dorsal compartment to insert into the dorsal base of the proximal phalanx. Its primary biomechanical role is the extension of the MCP joint. The extensor pollicis longus (EPL), routing around Lister's tubercle through the third dorsal compartment, inserts into the base of the distal phalanx. While its primary function is IP joint extension, it also significantly contributes to MCP extension through its robust connections to the dorsal hood.
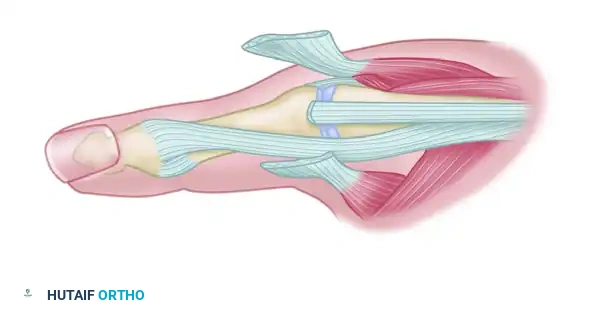
The intrinsic muscles play a critical role in both the stability and the dynamic function of the thumb MCP joint. The abductor pollicis brevis (APB), located on the radial aspect, and the adductor pollicis, located on the ulnar aspect, send transverse fibers that weave into the extensor mechanism, forming the extensor hood. In a healthy joint, these intrinsic expansions stabilize the EPL directly over the dorsal midline of the MCP joint and assist in MCP extension when the joint is near full extension. The collateral ligaments (radial and ulnar) provide essential static coronal plane stability, while the volar plate prevents hyperextension and provides a congruent articular surface for the metacarpal head.
In the rheumatoid thumb, the biomechanical equilibrium is catastrophically disrupted. The attenuation of the dorsal capsule by synovial pannus allows the intrinsic expansions to slip volarly, dropping below the joint's transverse axis of rotation. This shift changes their moment arm, converting them from stabilizers and weak extensors into powerful, deforming flexors. Furthermore, the volar subluxation of the proximal phalanx on the metacarpal head alters the joint's center of rotation, increasing the mechanical advantage of the flexor pollicis longus (FPL) and the displaced intrinsics, thereby locking the joint into a fixed flexion posture.
Surgical reconstruction, particularly soft tissue rebalancing procedures like the Inglis technique, must meticulously reverse this biomechanical collapse. It is not sufficient to merely perform a synovectomy; the surgeon must anatomically repair the EPB to restore the primary MCP extensor force vector. Equally critical is the dorsal advancement and reattachment of the intrinsic muscles (APB and adductor pollicis) to the reconstructed extensor mechanism. This critical step restores their mechanical advantage, pulling them back above the axis of rotation, and converting them back into dynamic stabilizers that maintain the EPL centralized over the dorsal metacarpal head.
Exhaustive Indications and Contraindications
Surgical intervention at the thumb MCP joint in the rheumatoid patient is dictated by a careful calculus involving the severity of articular destruction, the flexibility or rigidity of the deformity, the condition of the adjacent joints (CMC and IP), and the patient's overall functional demands. The decision-making process requires a nuanced understanding of when to employ soft tissue reconstruction versus joint sacrificing or implant-based procedures.
Soft tissue reconstruction, encompassing radical synovectomy and tendon rebalancing (the Inglis technique), is strictly indicated for early-stage disease. The ideal candidate presents with a Nalebuff Type I deformity that is passively correctable. Radiographic evaluation must demonstrate preserved articular cartilage with minimal to no erosive changes, and adequate joint space must be maintained. The goal here is prophylactic and restorative: to halt the progression of joint destruction by removing the offending synovium and to restore the biomechanical balance of the extensor mechanism before fixed contractures or severe bone loss occur.
Silicone implant arthroplasty is indicated for older, lower-demand patients who present with advanced joint destruction, significant articular erosions, or early fixed deformities, but who still retain adequate bone stock and restorable capsuloligamentous stability. It is particularly invaluable when the IP joint is severely damaged and requires arthrodesis. In such scenarios, preserving MCP motion becomes critical to allow the patient to maneuver the thumb for pulp-to-pulp pinch. The implant acts as a dynamic spacer rather than a stabilizing hinge; therefore, the collateral ligaments must be competent or meticulously reconstructed to prevent post-operative subluxation.
Arthrodesis remains the most predictable, durable, and reliable procedure for severe, fixed deformities characterized by profound bone loss, gross collateral ligament instability, or severe subluxation. It provides a stable, pain-free post for pinch grip and is highly recommended for high-demand patients, younger patients with aggressive disease, or in cases where soft tissue reconstruction has failed or is doomed to fail due to inadequate tissue quality. Contraindications to arthrodesis include a fused or stiff IP and CMC joint in the same ray, as a completely rigid thumb severely compromises hand dexterity.
Indications and Contraindications Summary
| Procedure | Primary Indications | Absolute/Relative Contraindications |
|---|---|---|
| Soft Tissue Reconstruction (Inglis) | Passively correctable Nalebuff Type I deformity; Preserved articular cartilage; Minimal radiographic erosions. | Fixed, rigid deformities; Severe articular destruction; Gross collateral ligament instability. |
| Silicone Implant Arthroplasty | Advanced joint destruction; Low-demand patient; IP joint requires arthrodesis; Adequate bone stock. | High functional demands; Active infection; Inadequate bone stock; Unreconstructable collateral ligaments. |
| MCP Joint Arthrodesis | Severe, fixed deformity; Profound bone loss; Gross instability; High-demand patient; Failed prior arthroplasty. | Ipsilateral CMC and IP joint arthrodesis (relative); Active infection (until cleared). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of successful rheumatoid thumb reconstruction. The clinical examination must systematically evaluate the entire thumb ray. The surgeon must assess the active and passive range of motion of the CMC, MCP, and IP joints. The flexibility of the MCP flexion deformity is tested; if the joint cannot be passively extended to neutral, soft tissue reconstruction alone will be insufficient, and osseous procedures (arthrodesis or arthroplasty) must be planned. The stability of the ulnar and radial collateral ligaments is assessed by applying varus and valgus stress in both extension and 30 degrees of flexion. Furthermore, the functional status of the EPL and FPL tendons must be verified to rule out spontaneous ruptures, which are common in advanced rheumatoid disease.
Radiographic assessment requires high-quality, true anteroposterior (AP), lateral, and oblique views of the thumb, as well as a standard posteroanterior (PA) view of the entire hand and wrist to assess the global rheumatoid burden. The surgeon must meticulously scrutinize the MCP joint for joint space narrowing, periarticular osteopenia, subchondral cysts, and marginal erosions. The bone stock of the metacarpal head and the base of the proximal phalanx is evaluated to determine if it can support a silicone implant or accommodate the hardware required for arthrodesis. If arthroplasty is considered, pre-operative templating using digital overlays is essential to estimate the appropriate size of the silicone elastomer implant, ensuring the stems will fit snugly within the medullary canals without causing cortical blowout.
Patient positioning and anesthesia are standardized to optimize surgical exposure and patient safety. The procedure is typically performed under regional anesthesia, such as an axillary or supraclavicular brachial plexus block, which provides excellent intraoperative anesthesia and prolonged postoperative analgesia. The patient is positioned supine with the operative arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the upper arm and inflated after exsanguination with an Esmarch bandage to ensure a bloodless surgical field, which is critical for identifying delicate neurovascular structures and performing a meticulous synovectomy.
The surgical site is prepped and draped in a standard sterile fashion. The surgeon sits in the axilla, providing a direct, unobstructed view of the dorsal aspect of the thumb. Intraoperative fluoroscopy (C-arm) must be readily available in the operating room, positioned to enter from the distal or contralateral side of the hand table. Fluoroscopy is indispensable for verifying the placement of transfixing Kirschner wires during soft tissue reconstruction, confirming the seating of silicone implants, or assessing the alignment and hardware placement during an arthrodesis.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach for the rheumatoid thumb MCP joint requires meticulous soft tissue handling and a deep understanding of the altered pathoanatomy. The Inglis technique for soft tissue reconstruction serves as the foundational approach, focusing on radical synovectomy, relocation of the displaced intrinsic muscles, and reattachment of the EPB to restore active MCP extension.
Incision and Exposure
Make a longitudinal or slightly curved incision over the dorsum of the metacarpophalangeal joint. The incision should extend from the middle of the proximal phalanx to the midshaft of the first metacarpal. Meticulous blunt dissection in the subcutaneous tissues is absolutely critical to identify, mobilize, and protect the terminal branches of the superficial radial nerve. Injury to these delicate sensory branches can result in debilitating, painful neuromas that severely compromise patient satisfaction. Retract the skin flaps and superficial tissues using fine skin hooks or a self-retaining retractor, taking care not to crush the skin edges, which are often fragile in patients on chronic systemic corticosteroids.
Tendon Dissection and Extensor Hood Release
Deepen the dissection to expose the extensor apparatus. Observe the extensor pollicis brevis (EPB) to determine the extent of its pathology. In advanced Nalebuff Type I deformities, the EPB will have become detached from the proximal phalangeal bone and retracted proximally, often embedded in a mass of hypertrophic synovium.
Split the extensor hood longitudinally between the extensor pollicis longus (EPL) and the extensor pollicis brevis (EPB). To mobilize the volarly displaced intrinsic muscles, systematically detach the abductor pollicis brevis from the extensor hood on the radial side. Proceed to detach the adductor pollicis from the ulnar side. This release is crucial for correcting the flexion deforming forces acting on the joint and allowing for the eventual dorsal advancement of these structures.
Radical Synovectomy and Joint Preparation
Retract the remaining tendon structures laterally to fully expose the dorsal capsule and the underlying, often exuberant, synovium. Perform a meticulous and radical synovectomy. Excision of all synovium within the joint is often facilitated by gently flexing the MCP joint, which opens the dorsal joint space and allows access to the volar pouch. It is imperative to preserve the radial and ulnar collateral ligaments during this debridement to maintain the coronal stability of the MCP joint. Use a combination of sharp dissection and rongeurs to clear the gutters and the recess between the collateral ligaments and the metacarpal head.
Tendon Reattachment and Skeletal Stabilization
Prepare the dorsal base of the proximal phalanx for tendon reinsertion. Create a bony trough by removing a small window of cortical bone. Drill a small hole for sutures on each side of the dorsum of the base of the proximal phalanx. Make a larger central hole just distal to and between these suture holes to serve as the insertion point for the extensor pollicis brevis tendon. Advance the EPB and attach it into the bony trough using robust, non-absorbable sutures (e.g., 3-0 or 4-0 braided polyester) passed through the drill holes. The EPB must be attached with sufficient tension to maintain full extension of the metacarpophalangeal joint against gravity.
Next, reattach the abductor pollicis brevis and adductor pollicis dorsally to the reconstructed extensor mechanism. This dorsal advancement restores the balance of the joint, converting these muscles back into dynamic stabilizers.
To protect the tendon repairs and maintain the joint in the corrected position, the metacarpophalangeal joint must be temporarily immobilized. Maintain the MCP joint in 0 degrees of extension by driving two transfixing Kirschner wires (typically 0.045-inch) across the joint, verifying their placement with fluoroscopy.
Alternative: Arthrodesis and Arthroplasty Techniques
If soft tissue reconstruction is contraindicated due to cartilage destruction, arthrodesis or arthroplasty is performed through the same dorsal approach. For an arthrodesis, the metacarpal head and the base of the proximal phalanx are prepared using cup-and-cone reamers or flat saw cuts to expose bleeding cancellous bone. The joint is positioned in 10 to 15 degrees of flexion, slight pronation, and 10 to 15 degrees of abduction. Fixation is rigidly achieved using crossed K-wires, a tension band construct, or a low-profile dorsal plate and screws.
For a silicone implant arthroplasty, the metacarpal head is resected just proximal to the collateral ligament origins. The medullary canals of the metacarpal and proximal phalanx are broached to accept the stems of a Swanson silicone implant. The implant is inserted using a no-touch technique, and the dorsal capsule and extensor mechanism are meticulously imbricated over the implant to provide stability and prevent dorsal extrusion.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, reconstruction of the rheumatoid thumb MCP joint carries a distinct profile of complications, largely driven by the progressive nature of the underlying systemic disease and the inherently compromised soft tissue envelope. The most common complication following soft tissue reconstruction is the recurrence of the flexion deformity. This usually results from progressive rheumatoid disease attacking the reconstructed tissues, mechanical failure of the tendon repair (often due to patient non-compliance with post-operative splinting), or unrecognized, progressive CMC joint disease leading to secondary MCP collapse. Salvage for recurrent deformity typically mandates conversion to an MCP joint arthrodesis.
Infection is a devastating complication, particularly in patients on biologic disease-modifying antirheumatic drugs (DMARDs) or chronic corticosteroids. Pin tract infections associated with the temporary K-wires used in the Inglis technique are relatively common but usually superficial. They must be managed aggressively with local pin care and oral antibiotics; if erythema progresses, the pins must be removed prematurely. Deep peri-prosthetic infections following silicone implant arthroplasty are rare but catastrophic, requiring implant removal, aggressive debridement, placement of an antibiotic spacer, and eventual conversion to a resection arthroplasty or bone-grafted arthrodesis once the infection is eradicated.
Stiffness is a frequent sequela, particularly if the MCP joint is immobilized for an extended period or if the EPB is over-tensioned during reconstruction. While a stiff, straight MCP joint is highly functional and mimics the outcome of an arthrodesis, it may limit fine motor tasks if the adjacent IP or CMC joints are also compromised. Intensive hand therapy is the first line of management, though severe contractures may occasionally require secondary tenolysis or capsulotomy. Nerve injury, specifically to the superficial radial nerve branches, results in painful neuromas. Prevention through meticulous dorsal dissection is paramount. If a neuroma develops, management involves conservative measures (desensitization, gabapentinoids) followed by surgical excision and proximal burying of the nerve stump into muscle or bone if conservative measures fail.
Complications and Salvage Strategies
| Complication | Estimated Incidence | Etiology/Risk Factors | Salvage Management |
|---|---|---|---|
| Recurrent Deformity | 15% - 25% | Progressive RA; Failed tendon repair; Unaddressed CMC arthritis. | Conversion to MCP joint arthrodesis. |
| Pin Tract Infection | 5% - 10% | Poor local hygiene; Prolonged K-wire retention; Immunosuppression. | Oral antibiotics; Local wound care; Early pin removal. |
| Silicone Synovitis / Implant Failure | 10% - 20% (Long-term) | Particulate wear debris; High mechanical demand; Implant fracture. | Implant removal; Conversion to arthrodesis with structural bone graft. |
| Nonunion (Arthrodesis) | 2% - 5% | Poor bone stock; Inadequate fixation; Smoking; Corticosteroid use. | Revision arthrodesis with rigid plate fixation and autologous bone grafting. |
Phased Post-Operative Rehabilitation Protocols
The ultimate success of the Inglis soft tissue reconstruction, or any motion-preserving procedure at the rheumatoid thumb MCP joint, relies heavily on strict adherence to a meticulously phased postoperative rehabilitation protocol. The delicate balance between protecting the healing tendon repairs and preventing restrictive adhesions requires the close collaboration of the orthopedic surgeon, a certified hand therapist (CHT), and a compliant patient.
Immediate Postoperative Phase (0-2 Weeks):
Following wound closure in the operating room, a bulky, non-compressive dressing is applied, reinforced with a rigid volar thumb spica splint. The thumb is immobilized with the MCP joint in full (0 degrees) extension and the CMC joint in functional palmar abduction. The IP joint is intentionally left free. The patient is instructed to begin immediate active range of motion (ROM) exercises of the IP joint. This early motion is critical to prevent adhesions of the extensor pollicis longus (EPL) and flexor pollicis longus (FPL) tendons, which glide adjacent to the surgical site. Strict elevation is maintained to control edema, which can compromise wound healing.
First Clinic Visit and Splinting Phase (2-4 Weeks):
At approximately two weeks postoperatively, the initial surgical splint and skin sutures are removed. The surgical site is carefully inspected for any signs of infection, marginal necrosis, or wound dehiscence. A custom thermoplastic thumb spica splint is fabricated by the hand therapist. This splint must meticulously maintain the MCP joint in 0 degrees of extension to protect the EPB repair and the advanced intrinsic muscles. The transfixing Kirschner wires remain in place, providing rigid internal stabilization. The patient continues IP joint motion and is instructed on edema management techniques, including retrograde massage and compression garments if necessary.
Pin Removal and Mobilization Phase (4-7 Weeks):
The transfixing Kirschner wires are removed in the clinic at approximately 4 weeks postoperatively. Following K-wire removal, a structured, progressive rehabilitation program begins. The patient initiates active range of motion (ROM) exercises for the MCP joint under the direct guidance of the hand therapist. Passive flexion is strictly avoided to prevent stretching the dorsal reconstruction. Splinting is continued at all times, particularly at night, except during these dedicated, short-duration exercise periods. The goal during this phase is to achieve a functional arc of active motion while ensuring the extensor lag does not recur.
Strengthening and Maturation Phase (7+ Weeks):
As the tendon repairs gain tensile strength, the daytime use of the splint is gradually weaned, though night splinting may be continued for up to 12 weeks to prevent nocturnal flexion posturing. Gentle strengthening exercises, focusing on key pinch, tip pinch, and overall grip strength, are introduced using graded putty and dynamic splinting if necessary. Patients are counseled that heavy lifting, forceful pinching, and repetitive gripping should be avoided for at least 10 to 12 weeks to ensure complete biological maturation of the tendon transfers and capsular repairs. Maximum medical improvement is typically not realized until 6 to 12 months postoperatively.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of the rheumatoid thumb has evolved significantly, guided by landmark biomechanical studies and long-term clinical outcome papers. The classification system proposed by Nalebuff in 1968 remains the universally accepted framework for categorizing rheumatoid thumb deformities. Nalebuff's precise delineation of the pathoanatomy of the Type I (boutonnière), Type II, and Type III (swan neck) deformities provided the foundation for targeted, stage-specific surgical interventions. His assertion that the MCP joint is the primary driver of the Type I deformity underscored the necessity of early intervention at this level to prevent global ray collapse.
The soft tissue reconstruction technique detailed in this chapter was popularized by Inglis et al. in the 1970s. Their seminal work demonstrated that radical synovectomy combined with the rerouting of the EPB and dorsal advancement of the intrinsic musculature could reliably restore the biomechanical balance of the MCP joint. Long-term follow-up studies of the Inglis procedure have shown excellent pain relief and maintenance of correction in appropriately selected patients with early-stage disease, cementing its status as the gold standard for passively correctable Nalebuff Type I deformities.
For advanced disease, the development of the flexible silicone elastomer implant by Alfred Swanson revolutionized the treatment of the destroyed rheumatoid MCP joint. Swanson's concept of resection arthroplasty combined with a dynamic spacer provided a reliable method for maintaining motion while alleviating pain. While long-term studies by Terrono and others have highlighted the risks of silicone synovitis and implant fracture, silicone arthroplasty remains a vital tool in the armamentarium, particularly when adjacent joint stiffness precludes arthrodesis.
Contemporary clinical guidelines, endorsed by organizations such as the American Society for Surgery of the Hand (ASSH) and the American Academy of Orthopaedic Surgeons (AAOS), emphasize a multidisciplinary approach. Modern treatment paradigms stress the importance of aggressive medical management with biologic DMARDs to halt disease progression, combined with timely, prophylactic surgical intervention before irreversible bone loss and rigid contractures dictate the necessity for joint-sacrificing salvage procedures.
