

Comprehensive Introduction and Patho-Epidemiology
Basal joint arthritis of the thumb, specifically involving the trapeziometacarpal (TM) joint, represents one of the most ubiquitous and functionally debilitating degenerative conditions encountered by the orthopedic hand surgeon. Epidemiologically, this pathology exhibits a profound predilection for postmenopausal females, typically presenting in the fifth and sixth decades of life. The disproportionate prevalence in women—often cited at a ratio of 6:1 compared to men—suggests a multifactorial etiology encompassing hormonal, anatomical, and genetic predispositions, including generalized ligamentous laxity and specific variations in trapezial morphology. The resultant functional deficit is severe, as the thumb accounts for approximately 40% to 50% of overall hand function, with TM joint arthritis profoundly compromising both powerful grip and precision pinch activities.
Historically, the surgical management of advanced basal joint arthritis has been dominated by trapeziectomy, either in isolation or combined with ligament reconstruction and tendon interposition (LRTI). While LRTI remains a reliable workhorse procedure with predictable long-term pain relief, it is not without significant drawbacks. These include prolonged postoperative rehabilitation, potential donor site morbidity, inevitable proximal subsidence of the metacarpal, and a measurable decrease in pinch strength over time. Consequently, the modern orthopedic paradigm has shifted toward joint-sparing and kinematic-restoring procedures for appropriately selected patients. This evolution has brought resurfacing arthroplasty (utilizing biologic or synthetic interpositional materials) and total joint replacement (TJR) to the forefront of our surgical armamentarium.
The primary objectives of these advanced surgical modalities are multifaceted: to eradicate pain, to restore the native center of rotation, to preserve trapezial bone stock (maintaining the length of the thumb ray), and to achieve superior postoperative kinematics compared to traditional resection techniques. By maintaining the anatomical length of the first ray, we optimize the resting tension of the intrinsic and extrinsic musculature, thereby maximizing pinch and grip strength. Furthermore, preserving the trapezium keeps future salvage options—such as a conversion to a standard trapeziectomy with LRTI—viable, effectively adhering to the surgical principle of avoiding "bridge-burning" interventions in younger or higher-demand patients.
In this comprehensive chapter, we will dissect the nuanced decision-making process, the intricate surgical anatomy, and the precise intraoperative execution required for both resurfacing arthroplasty (focusing on Artelon and Pyrocarbon implants) and total joint replacement of the thumb carpometacarpal joint. Mastery of these techniques demands not only a profound understanding of the complex biconcave-convex geometry of the saddle joint but also meticulous soft-tissue handling and exacting implant positioning.
Detailed Surgical Anatomy and Biomechanics
Before initiating any surgical intervention, a profound mastery of the trapeziometacarpal joint's surgical anatomy and biomechanical behavior is mandatory. The TM joint is universally classified as a biconcave-convex saddle joint. This unique articular geometry provides the thumb with an extraordinary six degrees of freedom: flexion-extension, abduction-adduction, and pronation-supination. This extensive mobility allows for the complex motion of circumduction and the critical function of opposition. However, this remarkable evolutionary adaptation comes at a significant biomechanical cost: the joint possesses minimal inherent bony constraint. Consequently, the stability of the TM joint is almost entirely reliant upon a complex, dynamic capsuloligamentous envelope.

Historically, the primary stabilizer of the TM joint was considered to be the deep anterior oblique ligament (dAOL), frequently referred to in classical literature as the "beak ligament." The dAOL originates from the palmar tubercle of the trapezium and inserts into the palmar base of the first metacarpal. While the dAOL's role in preventing dorsal subluxation during pinch is undeniable, modern biomechanical studies emphasize that TM joint stability relies on a highly synchronized network of 16 distinct ligaments. Seven of these are direct stabilizers: the superficial anterior oblique ligament (sAOL), the dAOL, the dorsoradial ligament (DRL), the posterior oblique ligament, the ulnar collateral ligament, the intermetacarpal ligament, and the dorsal intermetacarpal ligament. Recent anatomical investigations have elevated the status of the DRL, suggesting it may be the thickest and most critical restraint to dorsal metacarpal translation, challenging the traditional supremacy of the dAOL. The remaining nine ligaments serve as indirect stabilizers by anchoring the trapezium to the surrounding carpus (scaphoid, trapezoid, and capitate).
Pathophysiologically, the genesis of osteoarthritis at the basal joint is inextricably linked to the attenuation or traumatic rupture of these primary ligamentous restraints. When the capsuloligamentous complex becomes incompetent—whether through repetitive microtrauma, age-related degeneration, or acute injury—pathologic laxity ensues. This laxity permits abnormal dorsal and radial translation of the metacarpal base upon the trapezium. The resultant eccentric loading generates abnormally high shear forces, particularly concentrated on the palmar articular facet during lateral pinch and power grip. Over time, this mechanical mismatch leads to the progressive denudation of articular cartilage, subchondral sclerosis, and osteophyte formation. Clinically, the dorsal subluxation of the metacarpal base manifests as the pathognomonic "shoulder sign"—a visible and palpable prominence at the base of the thumb.
As the disease progresses into advanced stages, the altered kinematics initiate a cascade of secondary deformities. The chronic dorsal subluxation of the TM joint leads to an adduction contracture of the first web space. To compensate for this loss of extension and abduction at the basal joint, the patient unconsciously hyperextends the metacarpophalangeal (MCP) joint to open the hand for grasping large objects. This compensatory mechanism eventually attenuates the volar plate of the MCP joint, resulting in a fixed zigzag deformity characterized by TM joint flexion/adduction and MCP joint hyperextension. Failure to recognize and surgically address this secondary MCP hyperextension during TM joint arthroplasty will subject the new implant to catastrophic shear forces, leading to premature failure, dislocation, or accelerated subsidence.
Neurovascular Considerations
The surgical approach to the TM joint is fraught with neurovascular hazards that demand meticulous dissection. The superficial radial nerve (SRN) is the primary neurological structure at risk. The SRN bifurcates into multiple sensory branches that traverse the dorsoradial aspect of the wrist and thumb. Inadvertent transection, traction injury, or entrapment of these branches within scar tissue can result in debilitating neuromas or persistent dysesthesias that often overshadow the benefits of the arthroplasty. The SRN branches must be identified early, mobilized gently using vessel loops, and retracted with minimal tension.
Equally critical is the radial artery, which courses through the anatomic snuffbox, crossing the floor formed by the scaphoid and trapezium before diving between the two heads of the first dorsal interosseous muscle. The artery lies in intimate proximity to the volar-radial aspect of the TM joint capsule. During capsulotomy and subsequent trapezial resection or preparation, the artery is highly vulnerable to iatrogenic injury from scalpels, oscillating saws, or high-speed burrs. Preoperative assessment of collateral hand perfusion via an Allen test is mandatory. Intraoperatively, the artery must be definitively identified, meticulously mobilized from its surrounding venae comitantes and fascial attachments, and protected with a blunt retractor throughout the osseous preparation phases.
Exhaustive Indications and Contraindications
The selection of the appropriate surgical intervention for basal joint arthritis requires a synthesis of radiographic staging, clinical symptomatology, patient age, occupational demands, and the presence of concomitant pathologies. The Eaton and Littler staging system remains the gold standard for radiographic classification and heavily influences preoperative decision-making.
- Stage 1: Characterized by slight joint space widening (often indicative of effusion or synovitis) with normal articular contours. Patients typically present with pain but no significant subluxation.
- Stage 2: Demonstrates mild joint space narrowing, subchondral sclerosis, and the presence of small osteophytes (<2 mm), usually at the ulnar or palmar margins. Mild dorsal subluxation may be present.
- Stage 3: Marked by severe joint space narrowing, cystic changes, and prominent osteophytes (>2 mm). The joint may be significantly subluxed, but the scaphotrapezial (ST) joint remains radiographically normal.
- Stage 4: Characterized by pantrapezial arthritis, with severe degenerative changes involving both the TM joint and the ST joint.
- "Fifth Stage" (Senior Author's description): Extensive pantrapezial disease that encompasses the TM, ST, and the scaphotrapezoidal joints. This highlights the absolute necessity of intraoperative visual assessment of the scaphotrapezoidal articulation, as preoperative radiographs are notoriously insensitive (approximately 44%) for detecting arthritis in this specific joint.
Resurfacing arthroplasties (Artelon, Pyrocarbon) and Total Joint Replacements are generally indicated for patients with Eaton Stage 2 or 3 disease who have failed exhaustive conservative management (including NSAIDs, custom orthoses, intra-articular corticosteroid injections, and targeted thenar isometric strengthening). These joint-sparing procedures are particularly favored in younger, higher-demand patients where preservation of grip strength and trapezial bone stock is paramount.
Conversely, Stage 4 and "Stage 5" disease represent absolute contraindications for isolated TM joint resurfacing or standard unconstrained TJA, as placing an implant against a severely arthritic ST joint will result in persistent, debilitating pain. In these advanced stages, trapeziectomy (with or without LRTI) remains the procedure of choice.
Table 1: Indications and Contraindications for TM Joint Arthroplasty Modalities
| Surgical Modality | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Biologic Resurfacing (e.g., Artelon) | Eaton Stage 2-3; Younger, active patients; Desire to preserve bone stock. | Eaton Stage 4 (ST joint arthritis); Active infection; Severe inflammatory arthritis. | Severe MCP hyperextension (>30°) not addressed concurrently; Heavy manual labor. |
| Pyrocarbon Resurfacing | Eaton Stage 2-3; Patients requiring kinematic restoration; Adequate bone stock. | Inadequate trapezial bone stock; Eaton Stage 4; Uncorrectable instability. | Osteoporosis; History of crystalline arthropathy. |
| Total Joint Replacement (TJR) | Eaton Stage 2-3; Older, lower-demand patients seeking rapid recovery and motion. | Eaton Stage 4; Inadequate bone stock for cup/stem fixation; Active infection. | High-demand manual laborers; Severe, uncorrectable capsular laxity. |
| Trapeziectomy + LRTI | Eaton Stage 3-4; Pantrapezial disease; Failed previous arthroplasty. | None (Universal salvage procedure). | Younger patients where preservation of maximum grip strength is desired. |
Crucially, the surgeon must evaluate the entire upper extremity for coexisting conditions. Carpal tunnel syndrome (CTS) co-occurs in up to 44% of patients with TM joint arthritis. Postoperative edema from basal joint surgery can acutely exacerbate latent CTS, precipitating severe median nerve neuropathy. Therefore, concurrent carpal tunnel release should be strongly considered if preoperative EMG/NCS or clinical signs indicate median nerve compression. Furthermore, De Quervain's tenosynovitis, trigger thumb, and thumb sesamoid arthritis must be meticulously ruled out or addressed simultaneously to ensure a successful overall outcome.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful arthroplasty. Standard imaging must include a true anteroposterior (AP) view of the thumb (Robert's view or pronated AP), a true lateral view, and a posteroanterior 30-degree oblique stress view. The stress view is particularly valuable for unmasking dynamic instability and quantifying the degree of dorsal metacarpal subluxation. Digital templating should be utilized to estimate implant sizing, particularly for Total Joint Replacements, ensuring that the trapezial vault is of sufficient depth and width to accommodate the prosthetic cup without cortical breach.
As previously emphasized, clinical assessment of the thumb MCP joint is non-negotiable. If the MCP joint demonstrates hyperextension exceeding 20 to 30 degrees during a lateral pinch maneuver, it must be surgically addressed. Failure to do so will result in a persistent zigzag deformity, transferring immense cantilever forces to the newly implanted TM joint, leading to rapid implant loosening or dislocation. Depending on the severity of the hyperextension and the presence of intrinsic MCP arthritis, concurrent procedures such as volar plate capsulodesis, extensor pollicis brevis (EPB) transfer, or formal MCP joint arthrodesis must be integrated into the surgical plan.
Patient Positioning and Setup
The patient is positioned supine on the operating table. The affected upper extremity is extended onto a radiolucent hand table, providing broad, unimpeded access for both the surgeon and the fluoroscopy unit (C-arm). A well-padded pneumatic tourniquet is applied to the proximal brachium. Exsanguination with an Esmarch bandage and subsequent tourniquet inflation (typically to 250 mmHg) is critical to maintain a bloodless operative field, allowing for the precise identification of microvascular and neural structures.
The hand is generally maintained in neutral pronation-supination. A skilled surgical assistant is indispensable during these procedures. The assistant's role involves providing dynamic, counter-traction, gently retracting delicate soft tissues, and stabilizing the thumb ray—often by holding the distal phalanx with the nail plate oriented parallel to the floor. This precise positioning optimizes visualization of the saddle joint's complex topography. Prophylactic intravenous antibiotics (typically a first-generation cephalosporin) are administered within one hour prior to the surgical incision.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach for TM joint arthroplasty requires a delicate balance between achieving adequate exposure and preserving the dynamic stabilizers of the thumb.
Exposure and Soft Tissue Dissection
- Incision: A longitudinal or slightly curvilinear incision, measuring approximately 3 to 4 cm, is centered directly over the dorsal aspect of the carpometacarpal joint. This dorsal approach provides excellent visualization while avoiding the more complex volar neurovascular bundles.
- Superficial Dissection: The skin and subcutaneous tissues are incised with a #15 blade. Immediately deep to the dermis, the surgeon must transition to blunt dissection using fine tenotomy scissors to identify the branches of the superficial radial nerve (SRN). These sensory branches are meticulously mobilized, encircled with vessel loops, and retracted gently—usually dorsoulnarly—to prevent traction neuropraxia.
- Tendon Identification: The extensor pollicis longus (EPL) and extensor pollicis brevis (EPB) tendons are identified. The surgical interval is typically developed between the EPL and EPB, or alternatively, between the EPB and the abductor pollicis longus (APL), depending on the specific anatomical variations encountered.
- Radial Artery Mobilization: Deep to the extensor tendons, the radial artery is identified as it courses obliquely across the operative field. Using delicate blunt dissection, the artery and its venae comitantes are freed from the underlying joint capsule. A blunt retractor (such as a Ragnell or Senn retractor) is used to gently mobilize the artery, usually in a proximal and radial direction, ensuring its absolute protection during the osseous work.
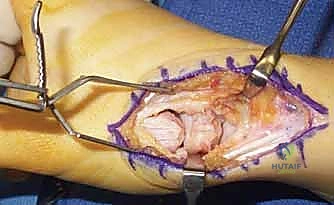
- Capsulotomy: A longitudinal or T-shaped incision is made through the dorsal joint capsule. Full-thickness capsular flaps are developed via subperiosteal elevation and reflected radially and ulnarly. The preservation of robust capsular flaps is vital for subsequent closure and joint stability.
- Joint Assessment: The joint is distracted, and the articular surfaces of the trapezium and metacarpal base are inspected. A crucial step at this juncture is the direct visual and tactile assessment of the scaphotrapezoidal joint to confirm the absence of advanced arthritis, which would necessitate a change in surgical strategy.
Technique 1: Artelon Resurfacing Arthroplasty (Biologic Approach)
For younger, high-demand patients, Artelon resurfacing utilizes a bioabsorbable polyurethane urea scaffold designed to act as an interpositional spacer. Over a period of several years, the implant degrades and is replaced by organized fibrous scar tissue, creating a biologic neo-articulation.
- Trapezial Preparation: The surgeon must choose between resection and decortication.
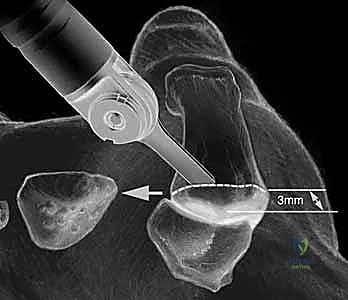
- Resection: Utilizing a high-speed oscillating sagittal saw, the distal 2-3 mm of the trapezial articular surface is resected perpendicular to the long axis of the trapezium. Surgical Warning: The flexor carpi radialis (FCR) tendon lies immediately volar to the trapezium in its fibro-osseous tunnel. The saw blade must be strictly controlled to prevent volar plunging and catastrophic FCR rupture.
- Decortication: Alternatively, a high-speed diamond or cutting burr is used to carefully decorticate the sclerotic subchondral bone of the trapezium, preserving its native biconcave contour. This exposes bleeding cancellous bone, optimizing the biological integration of the implant.
- Metacarpal Preparation: The base of the first metacarpal is similarly prepared using a high-speed burr to remove osteophytes and decorticate the articular surface, creating a congruent bed for the implant.
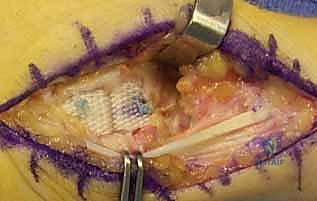
- Implant Sizing and Insertion: The T-shaped Artelon implant is sized. The central interpositional limb is seated deep within the joint space, while the two dorsal "wings" are draped over the prepared dorsal surfaces of the trapezium and metacarpal.
- Fixation: Fixation is achieved using bioabsorbable suture anchors (e.g., loaded with 2-0 high-tensile strength suture). Anchors are placed into the dorsal non-articular surfaces of the trapezium and metacarpal. The sutures are passed through the wings of the Artelon mesh and tied securely. Surgical Warning: Early iterations of this technique utilized cortical screws, which frequently resulted in mesh tear-out and implant failure. Suture anchors provide superior, distributed fixation and are the modern standard.




Technique 2: Pyrocarbon Resurfacing Arthroplasty
Pyrocarbon implants (such as the Ascension Saddle) are designed to perfectly mimic the complex native anatomy of the metacarpal base. Pyrocarbon possesses a modulus of elasticity remarkably similar to cortical bone, theoretically reducing the risk of stress shielding and subsequent subsidence.
- Metacarpal Dislocation and Resection: Following capsulotomy, a subperiosteal release of the metacarpal base is performed. The thumb is hyperflexed and adducted to dislocate the metacarpal base dorsally out of the surgical wound. Using an oscillating saw, a precise, perpendicular resection of the metacarpal base is performed just distal to the articular margin, removing minimal bone stock.
- Canal Preparation: The medullary canal of the first metacarpal is sequentially broached using specialized rasps. It is imperative to maintain the correct rotational alignment during broaching to ensure the saddle implant will articulate congruently with the trapezium.


- Trialing and Insertion: A trial implant is inserted, and the joint is reduced. Fluoroscopy and direct visualization are used to assess stability throughout a full range of motion. The implant must not impinge dorsally or volarly. Once the correct size is confirmed, the definitive pyrocarbon implant is press-fit into the metacarpal canal. The joint is reduced, and stability is meticulously re-verified.

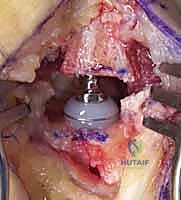
Technique 3: Total Joint Replacement (TJR)
Total joint arthroplasty of the TM joint involves replacing both the trapezial and metacarpal articular surfaces, typically utilizing a metal-on-polyethylene or dual-mobility bearing system.
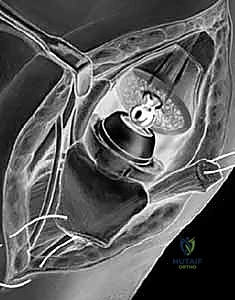
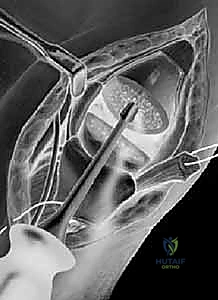
- Trapezial Cup Preparation: After resecting the metacarpal base, attention is turned to the trapezium. The center of the trapezial articular surface is identified. A guide pin is inserted centrally, and sequential reaming is performed to create a hemispherical bed. Extreme caution is required to avoid breaching the thin medial or volar cortices of the trapezium.
- Cup Insertion: The trapezial cup (often hydroxyapatite-coated titanium for cementless fixation, or an all-polyethylene cemented cup) is impacted or cemented into the prepared vault.
- Metacarpal Stem Insertion: The metacarpal canal is broached similarly to the pyrocarbon technique. The definitive metal stem is inserted (cemented or press-fit).
- Reduction and Closure: The modular prosthetic head is impacted onto the metacarpal stem, and the joint is reduced. The capsular flaps must be robustly repaired using non-absorbable or heavy absorbable sutures (e.g., 2-0 Ethibond or Vicryl) to prevent postoperative dislocation. If the capsule is deficient, a local capsuloperiosteal flap or a slip of the APL may be utilized to augment the closure.
Complications, Incidence Rates, and Salvage Management
While TM joint arthroplasty can yield exceptional functional results, the complication profile is non-trivial and demands respect. The most devastating intraoperative complication is injury to the radial artery or the superficial radial nerve. SRN neuromas occur in approximately 2% to 5% of cases and are notoriously difficult to manage, often requiring subsequent surgical excision and burying of the nerve stump into local muscle.
Implant-specific complications are a primary concern. For biological resurfacing (Artelon), foreign body inflammatory reactions (sterile synovitis) have been reported in up to 10-15% of patients in early studies, occasionally necessitating implant removal. For unconstrained implants like Pyrocarbon and TJR, dislocation and subluxation are the most frequent mechanical failures, occurring in 5% to 10% of cases. This is almost exclusively due to inadequate soft-tissue balancing, failure to recognize preoperative MCP hyperextension, or technical errors in implant positioning (e.g., placing the trapezial cup in excessive version). Aseptic loosening and subsidence of the metacarpal stem or trapezial cup also
Clinical & Radiographic Imaging Archive
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding thumb-carpometacarpal-joint-implant-and-resurfacing-arthroplasty