Mastering Silicone Arthroplasty for MCP and PIP Joints: An Intraoperative Guide

Key Takeaway
This masterclass provides a comprehensive, immersive guide to metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joint silicone implant arthroplasty. Fellows will learn intricate surgical anatomy, meticulous operative techniques from incision to closure, critical pearls for success, and strategies to manage potential pitfalls and postoperative complications. We cover patient selection, detailed bone preparation, implant sizing, and precise soft tissue balancing for optimal outcomes.
Comprehensive Introduction and Patho-Epidemiology
Silicone implant arthroplasty of the metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints represents a foundational pillar in the surgical management of end-stage inflammatory and degenerative arthritides of the hand. Originally pioneered by Alfred Swanson in the late 1960s, the conceptual genius of the silicone elastomer implant lies not in its ability to replicate a true anatomic articulation, but rather in its function as a dynamic spacer. This spacer maintains joint alignment and distracts the resected bony surfaces while the body mounts a localized fibrotic response. It is this very response—the formation of a thick, fibrous encapsulation around the silicone hinge—that ultimately confers long-term stability and guides the functional arc of motion.
The patho-epidemiology surrounding the indications for this procedure has undergone a paradigm shift over the last two decades. Historically, the relentless progression of rheumatoid arthritis (RA) provided a steady stream of patients presenting with profound ulnar drift, volar subluxation, and debilitating pain. The advent and widespread efficacy of disease-modifying antirheumatic drugs (DMARDs) and biologic therapies have drastically altered the natural history of RA, significantly reducing the incidence of end-stage hand deformities requiring surgical intervention. However, a distinct subset of patients either fail medical management, present late in the disease course, or suffer from aggressive phenotypes that escape pharmacologic control. For these individuals, silicone arthroplasty remains an invaluable, life-altering intervention.
Beyond the rheumatoid population, silicone arthroplasty is increasingly utilized in the management of advanced osteoarthritis (OA) and post-traumatic arthritis. In the osteoarthritic hand, the PIP joint is frequently the epicenter of pain and functional limitation, often presenting with profound osteophyte formation, joint space obliteration, and angular deformities. Post-traumatic arthritis, stemming from intra-articular fractures or chronic ligamentous instability, presents a unique challenge due to the frequently compromised soft tissue envelope and the presence of dense scar tissue. In these non-inflammatory cohorts, the primary goal of the procedure shifts slightly; while deformity correction remains important, the paramount objective is the reliable eradication of pain while preserving a functional, albeit sometimes limited, arc of motion.
Understanding the subtle differences in how these distinct pathologies affect the periarticular soft tissues is critical for intraoperative success. In RA, the surgeon must contend with attenuated collateral ligaments, stretched volar plates, and subluxated extensor mechanisms, necessitating meticulous soft tissue rebalancing alongside the arthroplasty. Conversely, in OA and post-traumatic scenarios, the soft tissues are often contracted and fibrotic, requiring aggressive, systematic releases to restore passive motion before the implant can even be trialed. Mastering silicone arthroplasty requires not just technical precision with the bone cuts, but a profound, almost intuitive understanding of this dynamic soft tissue envelope.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel is ever brought to the skin, a comprehensive, three-dimensional understanding of the intricate anatomy and biomechanics of the hand is absolutely paramount. Every structure, from the dense cortical bone of the phalangeal shafts to the delicate digital nerves, plays a critical role in the ultimate functional outcome and must be meticulously respected during dissection.
Metacarpophalangeal Joint Anatomy and Biomechanics
The MCP joint functions as a diarthrodial condyloid joint, permitting motion in three distinct planes: flexion-extension, abduction-adduction, and a limited degree of pronation-supination. This inherent multiplanar mobility makes the MCP joint somewhat more tolerant of early arthritic changes compared to the tightly constrained PIP joint, but it also renders it highly susceptible to complex, multi-planar deformities in the setting of advanced disease. The osteology of the metacarpal head is uniquely asymmetrical; it is wider on its volar aspect, which serves to tighten the collateral ligaments during flexion, providing maximal stability when gripping. Crucially, the radial condyle is typically larger and projects further distally than the ulnar condyle. This anatomical asymmetry acts as a skeletal fulcrum, inherently predisposing the proximal phalanx to ulnar deviation—a biomechanical reality that is brutally unmasked when the stabilizing radial soft tissues attenuate in rheumatoid disease.
The ligamentous architecture of the MCP joint is defined by the collateral ligaments and the volar plate. The proper collateral ligaments originate from the dorsal aspect of the metacarpal head, dorsal to the axis of rotation. This eccentric origin creates the critical "cam effect": the ligaments are lax in full extension, allowing for maximal abduction and adduction to accommodate objects of varying shapes, but they become progressively taut as the joint flexes to 90 degrees, rigidly locking the digit in place for power pinch and grip. During surgical resection of the metacarpal head, the surgeon must be acutely aware of this origin; over-resection will detach the collateral ligaments, leading to catastrophic, uncorrectable instability. The volar plate, a robust fibrocartilaginous structure, reinforces the joint volarly, resisting hyperextension and serving as the insertion site for the deep transverse metacarpal ligament, which tethers the adjacent metacarpals together.
Dorsally, the extensor mechanism provides dynamic stability and extension. The extensor digitorum communis (EDC) tendons are centralized over the metacarpal heads by the sagittal bands, which form a sling around the base of the proximal phalanx. In the rheumatoid hand, chronic synovitis leads to distension of the joint capsule and subsequent attenuation or frank rupture of the radial sagittal bands. Unopposed pull from the ulnar intrinsic muscles and the ulnar sagittal bands pulls the EDC tendon into the ulnar valley between the metacarpal heads. Once subluxated, the extensor tendon falls volar to the joint's axis of rotation, paradoxically becoming a flexor and a profound deforming force that exacerbates both volar subluxation and ulnar drift.
Proximal Interphalangeal Joint Anatomy and Biomechanics
In stark contrast to the MCP joint, the PIP joint is a highly constrained, bicondylar hinge joint. Its primary arc of motion is strictly limited to flexion and extension, typically ranging from 0 to 110 degrees. The stability of the PIP joint is heavily reliant on the congruity of its articular surfaces. The head of the proximal phalanx features two distinct condyles separated by an intercondylar notch, which perfectly articulate with the reciprocally contoured base of the middle phalanx. The base of the middle phalanx is notably wider on its volar aspect, a critical architectural feature that acts as a bony buttress against dorsal dislocation. Because of this tight bony congruity, the PIP joint is inherently more stable than the MCP joint, but it is also far less forgiving of minor articular incongruities or surgical malalignment.
The ligamentous support of the PIP joint lacks the pronounced cam effect seen at the MCP level. The proper collateral ligaments originate near the true axis of rotation on the proximal phalanx and insert onto the volar-lateral base of the middle phalanx. Consequently, these ligaments maintain a relatively constant state of tension throughout the entire functional arc of flexion and extension. The accessory collateral ligaments fan out volarly to insert onto the margins of the volar plate. The volar plate itself is a thick, rigid structure distally where it inserts into the middle phalanx, but it is thin and membranous proximally (the check-rein ligaments) to allow for joint flexion. Contracture of these check-rein ligaments is a primary driver of PIP joint flexion contractures in both OA and post-traumatic settings.
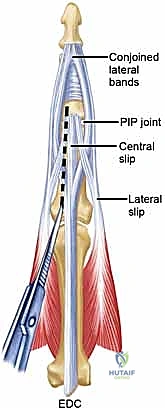
The extensor mechanism at the PIP joint is highly complex and delicate. The central slip of the extensor tendon inserts directly into the dorsal base of the middle phalanx, providing the primary force for PIP joint extension. The lateral bands diverge around the PIP joint to converge distally and insert on the distal phalanx. The integrity of the central slip is absolutely paramount; even minor attenuation or iatrogenic injury during surgical exposure will rapidly lead to a boutonnière deformity, characterized by PIP joint flexion and compensatory distal interphalangeal (DIP) joint hyperextension. Navigating this dorsal apparatus during a PIP joint arthroplasty requires meticulous, tissue-respecting surgical technique.
Exhaustive Indications and Contraindications
Patient selection is the absolute cornerstone of success in silicone arthroplasty. The surgeon must align the mechanical capabilities of the implant with the functional demands and physiological realities of the patient. The primary, overriding indication for this procedure is the relief of intractable pain that has proven refractory to comprehensive nonoperative management, including systemic pharmacotherapy, targeted corticosteroid injections, and custom orthotic splinting. Secondary goals include the correction of severe, debilitating deformities and the improvement of the functional arc of motion, though patients must be explicitly counseled that a return to "normal" physiological motion is rarely achieved.
Indications for Silicone Arthroplasty
The ideal candidate for a silicone MCP or PIP arthroplasty is a low-demand patient, typically older, who suffers from severe pain and progressive deformity that limits their ability to perform basic activities of daily living (ADLs). In the rheumatoid population, indications include fixed volar subluxation, severe ulnar drift that compromises grip mechanics, and joint destruction with bone loss. In these patients, the procedure reliably restores a centralized digital sweep, vastly improving the mechanics of grasp and release. For osteoarthritis, particularly at the PIP joint, the procedure is indicated for patients with painful, stiff joints who require preservation of motion for their specific daily tasks, making them poor candidates for an arthrodesis. It is critical to note that while arthroplasty can improve a restricted arc of motion, it will not restore motion to a joint that has been entirely stiff for years due to profound soft tissue contracture.
Absolute and Relative Contraindications
Contraindications must be rigorously respected to prevent catastrophic implant failure or profound morbidity. Absolute contraindications include the presence of active, ongoing local or systemic infection. Silicone is a foreign body, and placing it into a contaminated bed guarantees biofilm formation and subsequent failure. Inadequate bone stock is another absolute contraindication; the implant stems require a robust intramedullary canal to provide stable fixation and prevent early subsidence or periprosthetic fracture. If the medullary canals are destroyed by cystic rheumatoid changes or prior trauma, alternative salvage procedures must be considered.
Relative contraindications require nuanced clinical judgment. A completely non-functioning extensor mechanism is a strong relative contraindication. The silicone implant acts merely as a spacer; it possesses no inherent dynamic capabilities. If the patient cannot actively extend the digit preoperatively due to irrecoverable tendon rupture or profound neurologic deficit, the arthroplasty will simply fail into a flexed posture. Similarly, an uncorrected proximal deformity, particularly a severe radial deviation or volar subluxation of the wrist, will transmit massive, asymmetrical deforming forces distally across the newly reconstructed MCP joints, leading to rapid recurrent ulnar drift and premature implant failure. The wrist must be stabilized first.
| Category | Specific Conditions | Rationale / Clinical Impact |
|---|---|---|
| Primary Indications | Refractory pain in RA, OA, or post-traumatic arthritis | Improves quality of life and ADLs when conservative measures fail. |
| Primary Indications | Severe ulnar drift / volar subluxation (MCP) | Restores functional alignment and grip mechanics. |
| Absolute Contraindications | Active local or systemic infection | High risk of deep periprosthetic infection and biofilm formation. |
| Absolute Contraindications | Inadequate bone stock / destroyed medullary canals | Inability to seat or stabilize the implant stems, leading to subsidence. |
| Absolute Contraindications | Lack of adequate soft tissue coverage | Risk of implant exposure, extrusion, and subsequent infection. |
| Relative Contraindications | Irreparable extensor mechanism loss | Implant cannot actively extend; joint will rest in severe flexion. |
| Relative Contraindications | Uncorrected severe wrist deformity | Proximal deforming forces will rapidly destroy distal arthroplasty alignment. |
| Relative Contraindications | High-demand / heavy manual laborer | Accelerated wear, silicone particulate synovitis, and early implant fracture. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the crucible in which surgical success is forged. The surgeon must anticipate anatomic challenges, select appropriate implant sizes, and formulate a comprehensive strategy for soft tissue management long before the patient enters the operating theater.
Clinical Evaluation and Radiographic Assessment
The clinical examination must be exhaustive. Pain should be localized precisely to the joint line to differentiate articular pathology from tendinopathy or peripheral nerve entrapment. The active and passive range of motion (ROM) of every joint in the affected ray must be documented using a goniometer. Discrepancies between active and passive ROM suggest tendinous adhesions, ruptures, or profound intrinsic muscle contractures. The Bunnell test is mandatory to assess for intrinsic tightness; if the PIP joint cannot be passively flexed when the MCP joint is held in extension, intrinsic release will be a mandatory step during the arthroplasty. For PIP joint planning, the Elsen test is critical to evaluate the integrity of the central slip.
Radiographic evaluation begins with high-quality, orthogonal plain films (Anteroposterior, Lateral, and true Oblique views). These images are scrutinized for joint space narrowing, periarticular erosions, osteophyte formation, and the degree of subluxation.

FIG 1 • A. Rheumatoid arthritis affecting hand, with most notable disease affecting metacarpophalangeal (MCP) joints. The wrist is also affected.

FIG 1 • B. Isolated osteoarthritis of the MCP joint of the long finger.
Digital templating is a critical step. Using standardized radiographic markers, the surgeon templates the medullary canals of the metacarpals and phalanges to estimate the required implant sizes. The goal is to select an implant stem that fills the canal without causing excessive cortical tension, which could lead to intraoperative fracture. The hinge of the implant must sit flush against the resected bone surfaces without being compressed. It is imperative to ensure that a full array of implant sizes, including half-sizes, is available in the operating room, as radiographic templating is an estimate that must be confirmed with intraoperative broaching and trialing.
Anesthesia, Patient Positioning, and Tourniquet Application
The procedure is typically performed under regional anesthesia, most commonly an axillary or supraclavicular brachial plexus block, which provides excellent intraoperative anesthesia and prolonged postoperative analgesia. General anesthesia is reserved for patients with contraindications to regional blocks or those undergoing extensive, multi-limb procedures.
The patient is positioned supine on the operating table. The affected upper extremity is extended onto a dedicated, radiolucent hand table. Proper positioning is critical; the surgeon must have unimpeded 360-degree access to the hand, and the table must allow for full, unrestricted flexion and extension of the wrist and all digits to assess the dynamic balance of the arthroplasty during trial reduction. A well-padded pneumatic tourniquet is applied to the proximal arm. Exsanguination with an Esmarch bandage and inflation of the tourniquet (typically to 250 mm Hg or 100 mm Hg above systolic pressure) is absolutely essential. A perfectly bloodless field is non-negotiable for the meticulous identification of delicate neurovascular structures and the precise execution of soft tissue releases.
Step-by-Step Surgical Approach and Fixation Technique
The execution of a silicone arthroplasty demands a synthesis of aggressive bone resection and delicate, tissue-preserving soft tissue management. The operative flow must be systematic and reproducible.
Metacarpophalangeal Joint Arthroplasty Technique
For a single joint, a longitudinal dorsal incision is preferred to preserve venous drainage. However, in the rheumatoid patient requiring arthroplasty of all four fingers (index through small), a transverse dorsal incision centered over the metacarpal necks is the gold standard.

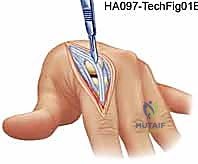
TECH FIG 1 • A. Transverse dorsal incision for metacarpophalangeal arthroplasty of all four fingers. The incision may be straight or undulating.
The skin flaps are elevated with extreme care, utilizing blunt dissection and fine electrocautery to preserve the longitudinal superficial veins and the delicate dorsal sensory branches of the radial and ulnar nerves. Ischemia to the dorsal skin flaps is a devastating complication. Once the extensor mechanism is exposed, the surgeon assesses the degree of ulnar subluxation.
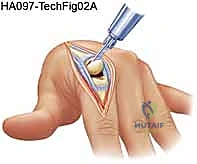
TECH FIG 2 • Extensor mechanism exposure. The ulnar sagittal band is often contracted and must be released to allow centralization of the extensor tendon.
The joint is typically entered by incising the attenuated radial sagittal band or by splitting the extensor tendon longitudinally. The collateral ligaments are identified and carefully preserved if possible, though in severe RA, they may need to be released to correct fixed deformities. The metacarpal head is then resected using an oscillating saw. The cut is made perpendicular to the long axis of the metacarpal shaft, typically removing the entire articular surface and a portion of the metaphyseal flare.

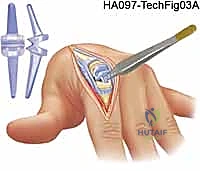
TECH FIG 3 • Resection of the metacarpal head. Care is taken to protect the volar neurovascular bundles.
Following resection, the medullary canals of the metacarpal and proximal phalanx are sequentially prepared using specialized broaches and reamers. The preparation must be meticulous; the canal should be widened enough to accept the implant stem without excessive force, but not so wide that the stem toggles.
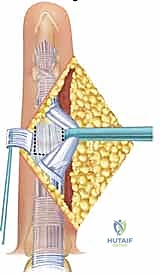
TECH FIG 4 • Broaching the medullary canal of the proximal phalanx.
Once the canals are prepared, sizing trials are inserted. The ideal implant allows for full extension to 0 degrees and flexion to at least 70-80 degrees without the stems pistoning out of the canals or the hinge buckling under tension. The joint must feel stable, and the digit should rest in neutral alignment without a tendency to drift ulnarly.
TECH FIG 5 • Trial reduction. The joint is taken through a full range of motion to assess stability and implant sizing.
After copious irrigation to remove all bone debris, the definitive silicone implant is inserted using a "no-touch" technique to minimize the risk of contamination and lipid absorption, which can weaken the elastomer. The implant stems are gently guided into the medullary canals using blunt forceps.

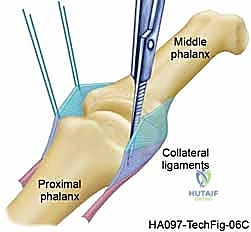
TECH FIG 6 • Insertion of the definitive silicone implant.
The final, and arguably most critical, step is the soft tissue reconstruction. The extensor tendon must be centralized over the newly reconstructed joint. This often requires imbrication or reefing of the radial sagittal band and a formal release of the ulnar intrinsic tendon if tightness persists.
TECH FIG 7 • Capsular closure and centralization of the extensor mechanism.
Proximal Interphalangeal Joint Arthroplasty Technique
The PIP joint presents a more formidable surgical challenge due to the delicate nature of the extensor mechanism. A dorsal longitudinal or curvilinear incision is utilized. The extensor mechanism is exposed, and the surgeon must choose between a central slip-splitting approach or a Chamay approach (elevating a distally based flap of the central slip).

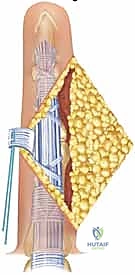
TECH FIG 8 • Exposure of the PIP joint. The central slip is carefully managed to preserve extensor function.
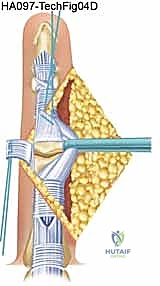
The collateral ligaments are released from their proximal attachments to allow the joint to be "shotgunned" open, providing excellent visualization of the articular surfaces. The head of the proximal phalanx is resected just proximal to the condylar flare. The base of the middle phalanx is typically preserved, with only marginal osteophytes removed, to maintain its broad, stabilizing volar lip.

TECH FIG 9 • Bone preparation at the PIP joint.
Broaching and trialing follow the same principles as the MCP joint. The implant must sit flush and allow for a smooth arc of motion from 0 to 90 degrees.
TECH FIG 10 • Insertion of the PIP silicone implant.
Closure at the PIP joint is exacting. The central slip must be meticulously repaired with non-absorbable sutures. Any lengthening or attenuation of the central slip during repair will inevitably result in an extensor lag and a subsequent boutonnière deformity, severely compromising the functional outcome.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, silicone arthroplasty carries a distinct profile of intraoperative and postoperative complications. The surgeon must be prepared to identify and manage these adverse events promptly to salvage the functional result.
Intraoperative and Early Postoperative Complications
Intraoperative complications are primarily mechanical. Iatrogenic fracture of the metacarpal or phalangeal shaft can occur during aggressive broaching or forceful implant insertion, particularly in osteopenic rheumatoid bone. If a non-displaced longitudinal split occurs, it can often be managed with cerclage wiring or by simply relying on the splinting effect of the implant stem. Displaced or transverse fractures may necessitate abandoning the arthroplasty in favor of formal internal fixation or immediate arthrodesis. Nerve injury is rare but can occur due to excessive traction or errant dissection, highlighting the need for a bloodless field and loupe magnification.
Early postoperative complications include wound dehiscence and superficial infection. The dorsal skin of the hand, especially in patients on chronic systemic corticosteroids, is thin and fragile. Ischemic necrosis of the skin margins requires aggressive wound care and, occasionally, local flap coverage. Deep periprosthetic infection is a catastrophic complication, occurring in approximately 1-2% of cases. It presents with escalating pain, erythema, and purulent drainage. Management mandates immediate surgical debridement, removal of the silicone implant, placement of an antibiotic spacer, and a prolonged course of culture-directed intravenous antibiotics.
Late Complications and Implant Failure
Late complications are largely related to the mechanical limitations of the silicone elastomer and the biological response
Clinical & Radiographic Imaging Archive