Digital & Thumb Joint Arthrodesis: An Intraoperative Masterclass

Key Takeaway
Join us in the OR for a masterclass on hand joint arthrodesis. We'll meticulously cover indications, comprehensive anatomy, precise preoperative planning, and detailed step-by-step intraoperative execution for DIP, PIP, and MCP fusions. Learn critical techniques, fixation options, and how to navigate potential pitfalls, ensuring optimal outcomes and stability for your patients.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater and to this definitive masterclass on small joint arthrodesis in the hand. As orthopedic surgeons, we are frequently tasked with the complex challenge of managing end-stage joint pathology where the delicate balance of mobility and stability has been irrevocably lost. Today, we are delving into the nuanced, technically demanding world of digital and thumb joint arthrodesis. This is a fundamental, cornerstone procedure that, when executed with meticulous precision and a profound understanding of biomechanics, offers profound pain relief, durable stability, and functional restoration for our patients. This intervention transcends the mere mechanical fusion of bones; it represents a critical, irreversible decision to purposefully eliminate motion for the greater functional good of the entire digit and, by extension, the hand.
The patho-epidemiology of small joint destruction in the hand encompasses a broad spectrum of challenging, often debilitating conditions. Osteoarthritis (OA) remains the most ubiquitous culprit, predominantly afflicting the distal interphalangeal (DIP) joints, though frequently involving the proximal interphalangeal (PIP) and thumb carpometacarpal (CMC) or metacarpophalangeal (MCP) joints. Patients typically present with a constellation of symptoms including insidious, progressive pain, palpable osteophytes, mucoid cysts, classic Heberden’s or Bouchard’s nodes, and progressive angular or rotational deformities that severely compromise pinch and grasp mechanics. Conversely, inflammatory arthropathies—such as rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), and psoriatic arthritis—present a different pathoanatomic challenge. In RA, relentless synovial proliferation and pannus formation lead to aggressive cartilage degradation and the insidious attenuation of critical supporting structures, including the collateral ligaments and the extensor apparatus, culminating in profound deformities like ulnar drift or fixed boutonnière postures.

The biomechanical trade-off inherent in arthrodesis requires a sophisticated understanding of hand kinematics. The hand operates on a foundational principle of a stable central post (the index and middle fingers) opposing a highly mobile ulnar border (the ring and small fingers) to facilitate both precision pinch and powerful grasp. When we elect to fuse a joint, we are actively prioritizing stability and pain relief over mobility. While modern arthroplasty techniques utilizing silicone, pyrocarbon, or surface replacements have advanced significantly, arthrodesis remains the unequivocal gold standard for specific joints—most notably the DIP joints, the thumb MCP joint, and the index finger PIP joint—where the functional demands for absolute stability far outweigh the benefits of preserved, albeit potentially weak or painful, motion.

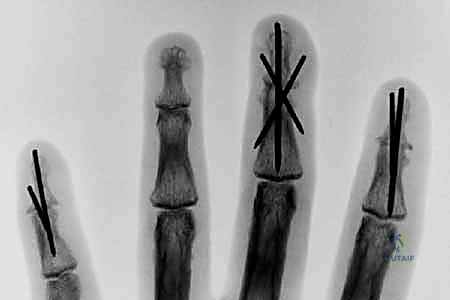
Looking toward the future of small joint arthrodesis, the evolution of fixation techniques continues to refine our intraoperative capabilities and postoperative outcomes. We have transitioned from the historical reliance on simple crossed Kirschner wires (K-wires), which often necessitated prolonged external immobilization and carried risks of pin tract infections, to highly sophisticated internal constructs. The advent of intraosseous wiring, dorsal tension band constructs, and, most prominently, headless compression screws (HCS) has revolutionized the procedure. These modern implants provide superior biomechanical rigidity, interfragmentary compression, and rotational control, allowing for earlier rehabilitation, decreased nonunion rates, and enhanced patient satisfaction. Mastery of these diverse fixation modalities is essential for the contemporary hand surgeon.
Detailed Surgical Anatomy and Biomechanics
Distal Interphalangeal Joint Architecture
Let us begin our anatomical dissection distally. The DIP joints are classic, highly constrained hinge (ginglymus) joints, biomechanically designed to permit primary motion in the sagittal plane—specifically flexion and extension—while rigidly resisting coronal and transverse plane forces. The bony architecture is fundamental to this stability; the condylar head of the middle phalanx is distinctly biconvex, articulating with the reciprocal biconcave base of the distal phalanx, which features a prominent central ridge. This interlocking configuration inherently limits lateral translation and axial rotation, providing static osseous stability even before the ligamentous constraints are considered.

The ligamentous and capsular structures of the DIP joint are robust and precisely engineered. The volar plate is a thick, fibrocartilaginous structure extending from its proximal membranous origin on the neck of the middle phalanx to a firm osseous insertion on the volar base of the distal phalanx. It acts as the primary checkrein against pathological hyperextension. Laterally, the joint is stabilized by the collateral ligament complex. The true collateral ligaments originate from the dorsal-lateral aspects of the middle phalanx condyles and insert onto the volar-lateral tubercles of the distal phalanx, remaining effectively isometric throughout the functional arc of motion. The accessory collateral ligaments fan out more volarly to insert onto the margins of the volar plate, specifically resisting lateral deviation when the joint is in full extension.

Dorsally, the extensor mechanism crosses the DIP joint as the terminal tendon, which is formed by the confluence of the lateral bands. This tendon inserts broadly onto the dorsal base of the distal phalanx, slightly distal to the articular margin. A critical clinical pearl for all operating surgeons: the germinal matrix of the nailbed is located in perilous proximity to this insertion site, averaging a mere 1.2 to 1.5 millimeters distal to the extensor insertion. Any aggressive dorsal surgical dissection, overzealous retraction, or errant drill bit placement during arthrodesis preparation can easily violate the nail matrix, resulting in a permanent, iatrogenic nail dystrophy.

Volarly, the flexor digitorum profundus (FDP) tendon traverses the joint to insert broadly onto the volar aspect of the distal phalanx, extending from the metaphyseal base to the midshaft. This powerful musculotendinous unit provides the primary flexion moment for the DIP joint. Furthermore, the neurovascular bundles, comprising the proper digital nerves and arteries, run along the lateral aspects of the digit, positioned volar to the collateral ligaments. While they are relatively protected during a standard dorsal surgical approach, meticulous lateral subperiosteal elevation and careful retractor placement are absolutely essential to avoid devastating iatrogenic neurovascular injury during joint preparation and hardware insertion.
Proximal Interphalangeal Joint Mechanics
Moving proximally along the digital ray, the PIP joints function as highly constrained hinge joints, structurally analogous to the DIP joints but subjected to significantly greater biomechanical loads and functional demands during power grasp and precision pinch. The osseous anatomy mirrors the distal joint, with the biconvex condylar head of the proximal phalanx articulating with the biconcave, centrally ridged base of the middle phalanx. This congruent articular geometry dictates a pure flexion-extension arc while severely restricting varus, valgus, and rotational laxity.
The soft tissue envelope of the PIP joint is arguably the most complex in the human digit. The volar plate is a massive, load-bearing structure that not only prevents hyperextension but also serves as the floor of the flexor tendon sheath. Its proximal attachments, the checkrein ligaments, anchor it firmly to the periosteum of the proximal phalanx. The collateral ligament complex consists of the robust true collateral ligaments, which are maximally taut in 15 to 20 degrees of flexion, and the accessory collateral ligaments, which stabilize the volar plate. Disruption of these structures, often seen in dorsal fracture-dislocations, leads to profound instability and rapid onset of post-traumatic arthritis, frequently necessitating arthrodesis.

The dorsal apparatus over the PIP joint is an intricate web of dynamic stabilizers. The extensor mechanism trifurcates over the proximal phalanx; the central slip, receiving contributions from the extrinsic extensor tendon and intrinsic lumbrical/interosseous muscles, inserts onto the dorsal tubercle of the middle phalanx to provide primary PIP extension. The lateral bands diverge to bypass the PIP joint laterally, stabilized by the transverse retinacular ligaments, before converging distally. Attenuation of the central slip, common in rheumatoid arthritis or following closed trauma, results in the classic boutonnière deformity—a frequent indication for PIP arthrodesis when the deformity becomes fixed and the joint articular surface is destroyed.

Volarly, the flexor mechanism is characterized by the complex interaction of the flexor digitorum superficialis (FDS) and the FDP. The FDS tendon bifurcates at the level of the proximal phalanx, wrapping around the FDP tendon at Camper's chiasm, to insert along the volar-lateral margins of the middle phalanx diaphysis. The neurovascular bundles run strictly laterally, volar to the axis of rotation. When performing a PIP arthrodesis, particularly via a lateral or volar approach, the surgeon must maintain a healthy respect for these structures, ensuring that all dissection remains strictly subperiosteal and that retractors do not inadvertently compress or stretch the proper digital nerves.
Metacarpophalangeal Joint Dynamics
The digital MCP joints (digits 2-5) represent a biomechanical departure from the interphalangeal joints; they are diarthrodial, multiaxial condyloid joints that permit motion in multiple planes, including flexion/extension, abduction/adduction, and a limited degree of circumduction and axial rotation. This multiaxial capability is essential for the hand's ability to conform to objects of varying shapes during grasp. The metacarpal head exhibits a complex, asymmetric, pear-shaped configuration; it is significantly wider on its volar aspect than its dorsal aspect, and its radius of curvature increases progressively from dorsal to volar (the "cam effect").

This unique osseous geometry fundamentally dictates the behavior of the collateral ligaments. Crucially, the metacarpal origin of the true collateral ligaments is located dorsal to the central axis of rotation. Consequently, as the MCP joint flexes, the ligaments are stretched over the wider volar flare of the metacarpal head, becoming maximally taut at approximately 70 to 90 degrees of flexion. Conversely, in extension, the ligaments are relatively lax, permitting maximal abduction and adduction. This dynamic tensioning is why digits must be immobilized in MCP flexion to prevent collateral ligament contracture, and it must be deeply understood when considering the rare indication for MCP joint arthrodesis.

The extensor mechanism at the MCP level lacks a direct tendinous insertion onto the proximal phalanx. Instead, MCP joint extension is achieved via a complex "sling effect." The sagittal bands of the extensor hood encircle the metacarpal neck and proximal phalanx, lifting the proximal phalanx into extension as the extensor digitorum communis contracts. Flexion is driven by the intrinsic muscles (lumbricals and interossei), which flex the MCP joint while simultaneously extending the IP joints via their contributions to the lateral bands.

Neurovascular anatomy at the MCP level requires precise navigation. The common digital nerves and vessels bifurcate into the proper digital nerves and vessels just proximal to the deep transverse metacarpal ligament. They course distally along the lateral aspects of the metacarpal neck and the base of the proximal phalanx. During dorsal capsulotomies or synovectomies preceding an MCP arthrodesis, the radial sagittal band of the index finger and the ulnar sagittal band of the small finger are particularly vulnerable zones where the neurovascular bundles can be inadvertently injured if dissection strays volar to the mid-axial line.
Thumb Metacarpophalangeal and Interphalangeal Joints
The articulations of the thumb, while sharing fundamental structural similarities with the digital joints, possess unique anatomical and biomechanical characteristics tailored to the thumb's specialized role in opposition and powerful pinch. The thumb MCP joint is a condyloid joint, but it exhibits remarkable inter-individual variability in its osseous contour. Some metacarpal heads are distinctly rounded, permitting a wider arc of motion, while others are flatter and more "square," inherently limiting lateral translation and total flexion-extension excursion. This variability dictates the baseline stability of the joint prior to any pathological insult.

The extensor apparatus of the thumb MCP is driven primarily by the extensor pollicis brevis (EPB), which inserts onto the dorsal base of the proximal phalanx. However, the size and efficacy of the EPB are highly variable; in a significant subset of patients, the extensor pollicis longus (EPL) tendon, which primarily extends the IP joint, assumes a major secondary role in extending the MCP joint through fascial connections. The collateral ligaments and volar plate function similarly to those of the digital MCPs, but the ulnar collateral ligament (UCL) of the thumb MCP is particularly critical, resisting the massive valgus forces generated during key pinch. Chronic UCL insufficiency (Gamekeeper's or Skier's thumb) that is unamenable to reconstruction is a classic indication for thumb MCP arthrodesis.

The thumb interphalangeal (IP) joint functions as a pure hinge joint, structurally analogous to the digital DIP and PIP joints. It is extended by the EPL tendon, which inserts onto the dorsal base of the distal phalanx, and flexed by the powerful flexor pollicis longus (FPL) tendon, which inserts volarly. The stability of the thumb IP joint is paramount for fine motor tasks and picking up small objects. When destroyed by osteoarthritis or inflammatory disease, arthrodesis provides an exceptionally reliable and functional outcome.

Neurovascular considerations in the thumb are critical, particularly regarding the radial sensory nerve branches. The proper digital nerves and vessels run laterally, volar to the collateral ligaments. However, the dorsal radial sensory nerve branches cross the anatomical snuffbox and course over the dorsoradial aspect of the thumb MCP and IP joints. These branches are exquisitely sensitive and highly prone to painful neuroma formation if injured during the dorsal or dorsoradial surgical approaches typically utilized for thumb joint arthrodesis. Meticulous superficial dissection and gentle retraction are mandatory.
Exhaustive Indications and Contraindications
The decision to proceed with small joint arthrodesis must be predicated on a rigorous, evidence-based evaluation of the patient's pathology, functional demands, and the status of adjacent articulations. Fundamentally, arthrodesis is indicated when a joint is irrevocably destroyed, profoundly unstable, or chronically painful, and where the preservation of motion is either technically impossible, functionally undesirable, or actively detrimental to the overall biomechanics of the hand. Osteoarthritis remains the most prevalent indication, particularly at the DIP joints, where patients present with intractable pain, progressive deviation, and functional impairment due to osteophyte impingement. Post-traumatic arthritis, following intra-articular fractures or chronic fracture-dislocations (especially at the unforgiving PIP joint), frequently culminates in the need for salvage arthrodesis when joint congruity cannot be restored.

The critical decision matrix between arthrodesis and arthroplasty requires a nuanced, joint-specific and digit-specific analysis. For the DIP joint, arthrodesis is universally considered the procedure of choice; the functional deficit from a fused DIP is clinically negligible, while the benefits of absolute stability and pain relief are profound. However, at the PIP joint, the calculus becomes highly complex. The index finger PIP joint demands absolute stability to withstand the sheer forces of lateral key pinch; therefore, an isolated, destroyed index PIP joint is almost exclusively managed with arthrodesis. Conversely, the small and ring finger PIP joints require mobility to facilitate a tight, conforming power grasp; thus, in the ulnar digits, arthroplasty (silicone or surface replacement) is often prioritized, reserving arthrodesis for cases of profound bone loss or uncorrectable soft tissue failure.

Inflammatory arthropathies, particularly Rheumatoid Arthritis (RA), present unique strategic challenges. In the rheumatoid hand, the surgeon is often faced with multi-level joint destruction. A critical axiom in rheumatoid reconstruction is the avoidance of "double-row arthroplasties" (performing arthroplasty at both the MCP and PIP joints of the same digit), as this predictably leads to recurrent deformity and functional failure due to the lack of a stable intercalated segment. The established paradigm for a digit with combined MCP and PIP destruction is to provide a stable, fused central post via PIP arthrodesis, thereby allowing for a successful, mobile MCP arthroplasty. In severe variants like arthritis mutilans (psoriatic arthritis), where massive osteolysis ("pencil-in-cup" deformity) obliterates bone stock, arthrodesis with structural bone grafting is often the only viable method to restore digital length and alignment.

Contraindications to small joint arthrodesis must be carefully respected to avoid catastrophic functional outcomes. Absolute contraindications include active, untreated local or systemic infection (which precludes the use of internal fixation), and a severely compromised soft tissue envelope or vascular insufficiency that would prevent wound healing. A critical relative contraindication, particularly for the thumb MCP joint, is stiffness or advanced arthritis in the adjacent joints. If a patient has a stiff thumb IP joint and a severely arthritic, immobile CMC joint, fusing the intervening MCP joint will render the thumb a rigid, useless post, severely crippling the hand. In such scenarios, alternative salvage procedures or staged reconstructions must be entertained.
| Clinical Condition | Primary Indication for Arthrodesis | Preferred Joint Target | Key Contraindications / Caveats |
|---|---|---|---|
| Primary Osteoarthritis | Intractable pain, instability, deformity | DIP Joints, Thumb MCP/IP | Avoid if adjacent joints are completely stiff. |
| Rheumatoid Arthritis | Boutonnière deformity, multi-level disease | PIP Joints (to support MCP arthroplasty) | Avoid double-row arthroplasty in the same digit. |
| Post-Traumatic | Chronic fracture-dislocation, incongruity | Index PIP, Any DIP | Poor soft tissue envelope requires flap coverage first. |
| Chronic Instability | Unreconstructable UCL tear (Gamekeeper's) | Thumb MCP Joint | Rule out concurrent advanced CMC arthritis. |
| Neurologic Deficit | Intrinsic minus hand, severe imbalance | Thumb MCP, Digital PIPs | Ensure tendon transfers are planned accordingly. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the bedrock of a successful small joint arthrodesis. The clinical evaluation must extend beyond the isolated painful joint. The surgeon must perform a comprehensive assessment of the entire upper extremity, meticulously documenting the active and passive range of motion of all adjacent joints. The patient's specific vocational and avocational demands must be deeply understood; a concert pianist will have vastly different functional requirements and tolerance for joint fusion than a heavy manual laborer. A thorough neurovascular examination is mandatory to ensure adequate digital perfusion and to document any pre-existing sensory deficits.
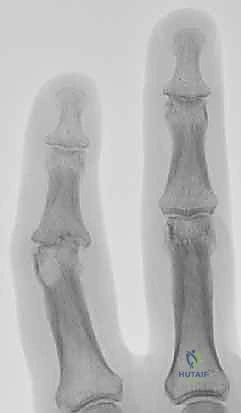
Radiographic evaluation requires high-quality, digitally calibrated, true posteroanterior (PA), true lateral, and oblique views of the affected digit. The surgeon must critically assess the degree of joint space narrowing, the presence of osteophytes, subchondral sclerosis, and most importantly, the geometry of any angular or rotational deformity. Pre-operative templating is essential, particularly when utilizing modern headless compression screws or plate constructs. The surgeon must measure the medullary canal diameter to select the appropriate screw thread diameter and estimate the required screw length, accounting for the anticipated bone resection necessary to achieve flat, bleeding cancellous surfaces.

Determining the optimal angle of fusion is arguably the most critical intraoperative decision, and it must be planned pre-operatively. We adhere to the concept of the "functional cascade" to optimize grasp. For the PIP joints, the index finger is typically fused in 25 to 30 degrees of flexion to optimize pinch, while the angle progressively increases moving ulnarly: 30-35 degrees for the middle finger, 35-40 degrees for the ring finger, and 40-50 degrees for the small finger to facilitate power wrap-around grasp. DIP joints are generally fused in neutral (0 degrees) to a maximum of 10 degrees of flexion. The thumb MCP joint is optimally fused in 10 to 15 degrees of flexion, 10 degrees of pronation, and slight abduction, while the thumb IP joint is fused in 0 to 15 degrees of flexion.
Patient positioning and anesthesia are tailored to the specific procedure and patient comorbidities. These procedures are highly amenable to regional anesthesia, such as a supraclavicular or axillary brachial plexus block, which provides excellent intraoperative conditions and prolonged postoperative analgesia. Alternatively, wide-awake local anesthesia no tourniquet (WALANT) techniques are increasingly utilized, allowing for intraoperative assessment of the digital cascade with active patient participation. If a traditional approach is used, the patient is positioned supine with the arm extended on a radiolucent hand table. A well-padded pneumatic upper arm tourniquet or a sterile forearm tourniquet is applied to ensure a bloodless surgical field, which is critical for meticulous cartilage resection and precise hardware placement. Prophylactic intravenous antibiotics (typically a first-generation cephalosporin) are administered strictly prior to tourniquet inflation.

Step-by-Step Surgical Approach and Fixation Technique
Surgical Exposure and Joint Preparation
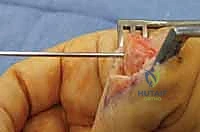
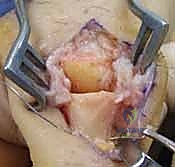
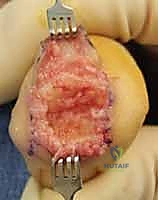
The surgical approach dictates the visualization of the joint and the protection of the surrounding soft tissue envelope. For the DIP and PIP joints, a dorsal approach is standard. Several skin incisions can be utilized, including a straight dorsal longitudinal incision, an H-shaped incision, or a Y-shaped (chamfer) incision. The straight dorsal approach is often preferred for its simplicity and extensibility. The skin and subcutaneous tissues are carefully elevated, taking immense care to identify and protect the delicate dorsal sensory nerve branches. At the DIP joint, the terminal extensor tendon is identified and sharply divided transversely or split longitudinally. The surgeon must remain hyper-vigilant of the germinal matrix, ensuring the dissection remains proximal to the nail fold.

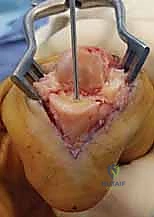
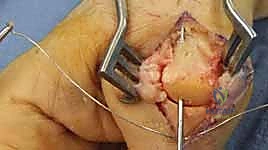
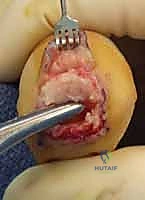
Once the extensor mechanism is breached, the dorsal capsule is excised, and the collateral ligaments are sharply released from their phalangeal insertions. This allows for maximal hyperflexion ("shotgunning") of the joint, providing unparalleled, 360-degree visualization of the articular surfaces. Joint preparation is the most critical step for achieving a successful arthrodesis. The goal is to completely eradicate all articular cartilage and sclerotic subchondral bone, exposing healthy, bleeding cancellous bone capable of robust osteogenesis.

Several techniques exist for bone preparation. The "flat-cut" technique utilizes an oscillating micro-sagittal saw to create perfectly planar surfaces at the predetermined angle of fusion; while technically straightforward, it inherently shortens the digit and offers minimal intrinsic osseous stability. The "cup-and-cone"
Clinical & Radiographic Imaging Archive