Mastering Thumb MCP Joint Collateral Ligament Repair: An Intraoperative Guide

Key Takeaway
Join us in the OR for an immersive masterclass on acute thumb MCP joint UCL and RCL primary repair. We'll meticulously cover surgical anatomy, preoperative planning, and granular, step-by-step intraoperative execution for both arthroscopic and open techniques. Learn to identify Stener lesions, manage avulsion fractures, and apply advanced repair strategies, alongside critical pearls, pitfalls, and comprehensive postoperative protocols for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues, to the operating theater. Today, we are undertaking a definitive exploration of a critical injury that, if mismanaged or underestimated, invariably leads to significant long-term disability, chronic pain, and a devastating loss of hand function: acute disruptions of the thumb metacarpophalangeal (MCP) joint collateral ligaments. These injuries are remarkably common in both athletic and general populations, yet they are frequently dismissed by primary care providers and emergency departments as "just a sprain." However, as orthopedic surgeons, we understand that the impact of a compromised thumb MCP joint on key pinch strength, tip-to-tip pinch, and overall hand dexterity is profound. The thumb contributes approximately forty percent of total hand function, and its stability is the cornerstone upon which this utility is built.
Historically, the chronic manifestation of the ulnar collateral ligament (UCL) injury was famously coined "gamekeeper's thumb" by Campbell in 1955, describing the attritional attenuation seen in Scottish gamekeepers who repeatedly applied a valgus force to the thumb while breaking the necks of rabbits. In modern practice, however, we more frequently encounter the acute variant, often termed "skier's thumb." This acute injury typically results from a sudden, forceful radial deviation and hyperextension moment applied to the thumb, classically occurring when a skier falls while gripping a ski pole. Conversely, radial collateral ligament (RCL) injuries, though historically considered less frequent, are increasingly recognized as a significant source of morbidity, often resulting from forced adduction and torsion.
Our primary surgical objective in addressing these injuries is not merely to achieve a rudimentary anatomical reattachment of the torn ligamentous ends. Rather, our goal is to meticulously restore the intricate, multi-planar biomechanics of the thumb MCP joint. This requires a profound understanding of the native footprint of the ligament, the tensioning required to restore stability without sacrificing physiological motion, and the nuanced interplay between the static capsuloligamentous restraints and the dynamic musculotendinous units. Failure to respect these principles inevitably leads to a stiff, painful, or recurrently unstable joint.
The paradigm of managing these injuries has shifted significantly over the past few decades. While partial tears and non-displaced avulsion fractures can often be managed with rigid immobilization, the identification of a complete ligamentous disruption—particularly one complicated by interposition of the regional aponeurosis—mandates prompt surgical intervention. The advent of advanced arthroscopic techniques and low-profile suture anchor technology has further refined our approach, allowing for minimally invasive reduction of intra-articular fractures and anatomically precise soft-tissue reconstructions. This chapter will serve as your exhaustive intraoperative guide to mastering both the arthroscopic and open management of these complex injuries.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel touches the skin, a master surgeon must possess a three-dimensional, encyclopedic understanding of the regional anatomy. The thumb MCP joint is a biomechanical marvel. While classically categorized as a diarthrodial condyloid joint, its functional kinematics more closely resemble a ginglymus (hinge) joint. Its primary arc of motion occurs in the flexion-extension plane, but it possesses a limited, yet absolutely crucial, capacity for abduction, adduction, and pronation. Unlike the interphalangeal joints, the inherent bony architecture of the thumb MCP joint is remarkably shallow. The metacarpal head is asymmetric, being broader on its volar aspect, which creates a cam effect that tightens the collateral ligaments during flexion. Because the bony congruence offers minimal constraint, the joint's stability is overwhelmingly dependent on its robust ligamentous and capsular envelope.
The Collateral Ligament Complex
The primary static stabilizers of the thumb MCP joint are the ulnar collateral ligament (UCL) and the radial collateral ligament (RCL). Both structures are anatomically analogous, each comprising two distinct, functionally specialized components: the proper collateral ligament and the accessory collateral ligament.

The Proper Collateral Ligaments (PCL) are the primary restraints to varus and valgus stress. They originate from a distinct fossa located on the dorsal third of the metacarpal neck, slightly proximal to the articular margin and dorsal to the joint's axis of rotation. From this dorsal origin, the fibers fan out obliquely and distally to insert onto the volar third of the base of the proximal phalanx. This specific dorsal-to-volar orientation is biomechanically critical; it ensures that the proper collateral ligaments become maximally taut when the joint is in flexion, thereby providing peak medial-lateral and dorsovolar stability during power pinch maneuvers.
The Accessory Collateral Ligaments (ACL) function as supplementary, yet vital, supports. They originate from the palmar aspect of the metacarpal neck fossa, located just volar to the origin of the proper collateral ligaments. Instead of inserting onto the proximal phalanx, the accessory fibers fan out volarly to insert directly into the lateral margins of the volar plate and the respective sesamoid bones embedded within it. Biomechanically, the accessory collateral ligaments are taut in full extension and become lax in flexion. Their primary role is to suspend and stabilize the volar plate, preventing hyperextension and volar subluxation of the joint.

Key Anatomical Distinctions: Ulnar vs. Radial Side
While the intrinsic ligamentous architecture is similar on both sides, the extrinsic soft-tissue envelope presents crucial differences that dictate both pathology and surgical approach. On the ulnar side, the adductor pollicis muscle inserts via a robust, relatively narrow fibrous expansion known as the adductor aponeurosis. This aponeurosis spans the ulnar aspect of the MCP joint, lying directly superficial to the UCL. When the UCL sustains a complete distal avulsion, the violent recoil of the ligament can cause its proximal stump to displace superficially, coming to rest on top of the adductor aponeurosis. The aponeurosis then acts as a mechanical barrier, preventing the ligament from healing back to its anatomic footprint. This pathognomonic phenomenon, described by Stener in 1962, is known as a Stener lesion. Its presence is an absolute indication for surgical repair, as non-operative management will uniformly result in chronic instability.
Conversely, the radial side of the joint is covered by the abductor aponeurosis, an expansion of the abductor pollicis brevis. Unlike the narrow adductor aponeurosis, the abductor expansion is broad and expansive, enveloping nearly the entire radial and dorsal-radial aspect of the MCP joint. Because of this broad coverage, a true Stener-like lesion—where the RCL completely retracts and becomes trapped superficial to the aponeurosis—is exceedingly rare. Consequently, while complete RCL tears still frequently require surgical repair due to high demands on the radial side during pinch, the physiological urgency dictated by an interposed aponeurosis is less of a factor.

Neurovascular Considerations in the Surgical Field
Navigating the surgical approaches to the thumb MCP joint requires meticulous respect for the regional neurovascular structures, as iatrogenic injury can lead to complications far more debilitating than the initial ligament tear. On the radial side, the terminal branches of the superficial radial nerve (SRN) are the primary hazard. These sensory branches arborize extensively as they cross the dorsal-radial aspect of the thumb and wrist. During a radial approach for RCL repair, these branches must be carefully identified, mobilized, and protected with gentle retraction. Injury to the SRN is notorious for producing exquisitely painful neuromas and debilitating dysesthesia that can render the thumb functionally useless.
On the ulnar side, the surgical field is traversed by the dorsal sensory branches of the ulnar nerve. While typically less prominent and less prone to painful neuroma formation than the SRN, they still warrant careful preservation. A more critical consideration on the ulnar side is the motor branch of the ulnar nerve supplying the adductor pollicis muscle. This nerve courses deep to the adductor aponeurosis and the muscle belly itself. While it is generally safe during a standard superficial approach to the UCL, overly aggressive deep dissection, blind placement of retractors, or extensive mobilization of the adductor pollicis origin during chronic reconstructions could potentially place this vital motor branch at risk.
Exhaustive Indications and Contraindications
The decision-making process for managing thumb MCP joint collateral ligament injuries relies heavily on a precise clinical examination, judicious use of imaging, and a clear understanding of the patient's functional demands. The overarching goal is to identify complete ruptures, specifically those with a Stener lesion or significant instability, which will fail conservative management.
The cornerstone of clinical diagnosis is the stress examination. For suspected UCL injuries, a valgus stress test is performed, and for RCL injuries, a varus stress test is utilized. It is absolutely imperative that these tests are performed with the joint in two distinct positions: full extension and 30 degrees of flexion. Testing in full extension primarily assesses the integrity of the accessory collateral ligament and the volar plate. Testing in 30 degrees of flexion isolates the proper collateral ligament, as the cam effect of the metacarpal head relaxes the volar structures. Laxity is always compared to the uninjured contralateral thumb.
An absolute indication for acute surgical repair is the presence of a clinically or radiographically confirmed Stener lesion. Furthermore, joint laxity exceeding 30 degrees in absolute terms, or a side-to-side difference greater than 15 degrees when compared to the contralateral normal thumb, strongly suggests a complete, high-grade tear warranting operative intervention. Additionally, the presence of volar subluxation of the proximal phalanx on lateral radiographs indicates a catastrophic failure of the dorsal capsule and collateral ligament complex, necessitating surgical restoration of joint congruency.
| Indication Category | Specific Clinical/Radiographic Findings | Recommended Management |
|---|---|---|
| Absolute Surgical Indications | Palpable Stener lesion (ulnar side) | Acute Open Repair |
| >30° absolute laxity on stress testing | Acute Open/Arthroscopic Repair | |
| >15° side-to-side difference in laxity | Acute Open/Arthroscopic Repair | |
| Volar subluxation of proximal phalanx | Acute Open Repair | |
| Displaced intra-articular avulsion fracture (>2mm) | Arthroscopic or Open Fixation | |
| Relative Surgical Indications | High-demand athlete with partial tear | Consider early repair vs. rigid cast |
| Chronic symptomatic instability (>6 weeks) | Reconstruction (tendon graft) | |
| Contraindications (Non-Operative) | Grade I/II sprains (stable endpoint, <15° difference) | Thumb spica cast/splint for 4-6 weeks |
| Non-displaced avulsion fracture (<2mm) | Thumb spica cast/splint for 4-6 weeks | |
| Severe pre-existing MCP joint osteoarthritis | Arthrodesis (Fusion) preferred | |
| Active local soft tissue infection | Debridement; delayed reconstruction |
Contraindications to acute primary repair must also be carefully considered. The most significant local contraindication is the presence of advanced, pre-existing osteoarthritis of the thumb MCP joint. In such cases, repairing the ligament will not alleviate the arthritic pain, and the surgical trauma may exacerbate stiffness; a primary MCP joint arthrodesis is the procedure of choice. Additionally, a severely compromised soft tissue envelope, active local infection, or a patient who is medically unfit for surgery represent absolute contraindications to elective ligament repair. In cases of chronic instability presenting months or years after the initial injury, the native ligament is often severely attenuated or scarred beyond functional utility, necessitating a tendon graft reconstruction rather than a primary repair.
Pre-Operative Planning, Templating, and Patient Positioning
Surgical success is frequently dictated before the patient ever enters the operating room. Meticulous preoperative planning begins with a comprehensive review of the patient's history, mechanism of injury, and physical examination findings. The timing of the injury is critical; acute repairs performed within the first 3 to 4 weeks yield significantly better outcomes than delayed repairs, as the ligament ends remain robust and anatomical landmarks are less obscured by fibrotic scar tissue.
Standard radiographic evaluation is mandatory for all suspected collateral ligament injuries. This includes true posteroanterior (PA), lateral, and oblique views of the injured thumb. It is highly recommended to obtain comparative views of the uninjured contralateral thumb to assess baseline joint congruency and identify subtle anatomical variations.

Radiographs are scrutinized for the presence of avulsion fractures at the ligament insertions (the "bony gamekeeper's" thumb), volar subluxation of the proximal phalanx, or pre-existing degenerative changes. While stress radiographs were historically popular, they are often intensely painful for the patient and rarely alter the treatment plan if a thorough clinical exam has been performed; however, they can be utilized under local anesthesia if the clinical exam is equivocal.

Advanced imaging modalities, such as Magnetic Resonance Imaging (MRI) or high-resolution ultrasonography, are excellent tools but are not strictly required for every acute injury. MRI is highly sensitive and specific for identifying complete ligament ruptures and the classic "yo-yo on a string" appearance of a Stener lesion. Ultrasound, when performed by an experienced musculoskeletal radiologist, offers the advantage of dynamic, real-time assessment of ligament integrity during stress maneuvers. These modalities are most useful in complex cases, delayed presentations, or when the clinical examination is limited by severe swelling and guarding.

On the day of surgery, patient positioning and anesthesia optimization are paramount. We typically employ a regional anesthetic technique, such as an axillary or supraclavicular brachial plexus block, combined with light intravenous sedation. This provides profound intraoperative analgesia, excellent muscle relaxation (which aids in joint reduction and stress testing), and prolonged postoperative pain control. The patient is positioned supine on the operating table. The affected upper extremity is abducted and placed on a stable, radiolucent hand table.
A well-padded pneumatic tourniquet is applied to the proximal arm and typically inflated to 250 mmHg after exsanguination with an Esmarch bandage, ensuring a pristine, bloodless surgical field. This is absolutely critical for identifying delicate neurovascular structures and assessing the quality of the ligamentous tissue. Intraoperative fluoroscopy (a mini C-arm) must be positioned perpendicularly to the hand table, allowing the surgeon to easily bring the unit in and out of the field without disrupting the sterile setup or requiring the patient to be repositioned. For arthroscopic procedures, we utilize a simple finger trap applied to the thumb, utilizing approximately 5 to 8 pounds of longitudinal traction. We explicitly avoid bulky traction towers, as they severely impede the maneuverability of the fluoroscope and restrict access to the surgical portals.
Step-by-Step Surgical Approach and Fixation Technique
We will now detail the intraoperative execution, beginning with the arthroscopic management of avulsion fractures—a technique that minimizes soft tissue morbidity—followed by the definitive open approach for soft tissue ruptures and Stener lesions.
Arthroscopic Treatment of UCL Avulsion Fractures
The arthroscopic approach is exceptionally well-suited for addressing displaced intra-articular avulsion fractures of the UCL base, allowing for precise, visually confirmed reduction without the morbidity of a large arthrotomy.
-
Joint Distension and Portal Establishment:
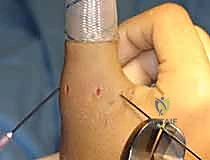
The procedure begins with accurate palpation of the MCP joint line. Using an 18-gauge needle, we inject 1 to 2 mL of local anesthetic (e.g., 1% lidocaine) directly into the intra-articular space. This distends the tight joint capsule, displacing the neurovascular structures superficially and creating a safe corridor for portal placement.

Our primary viewing portal is the dorsoradial (DR) portal. A small, longitudinal stab incision is made through the skin just radial to the extensor pollicis longus (EPL) tendon at the level of the joint line. Blunt dissection with a mosquito hemostat is used to spread the subcutaneous tissues, protecting the superficial radial nerve branches. A blunt trocar is then introduced, followed by a 1.9-mm, 30-degree arthroscope. This radial vantage point provides an expansive, panoramic view of the ulnar-sided pathology.

-
Working Portal and Intra-articular Preparation:
Under direct arthroscopic visualization, a spinal needle is utilized to localize the optimal position for the dorsoulnar (DU) working portal. This portal is typically established just dorsal to the adductor pollicis tendon insertion. A longitudinal stab incision is made, and a 2.0-mm or 2.5-mm full-radius shaver is introduced.
The initial step is a meticulous intra-articular debridement. The shaver is used to evacuate the inevitable hemarthrosis and clear away fibrinous debris. A targeted synovectomy is performed along the ulnar gutter to clearly expose the fracture bed on the proximal phalanx and the corresponding avulsed bony fragment attached to the distal UCL.

-
Fracture Reduction and Percutaneous Fixation:
Once the fracture bed is prepared and cleared of interposed soft tissue, reduction is achieved. This can often be facilitated by applying a varus force to the thumb to relax the UCL, combined with direct manipulation of the fragment using an arthroscopic probe or a small periosteal elevator introduced through the working portal.

While maintaining the reduction under direct arthroscopic visualization, a 0.045-inch Kirschner wire (K-wire) is introduced percutaneously from the ulnar aspect of the thumb, aiming from distal-ulnar to proximal-radial.
The K-wire captures the avulsed fragment and drives it securely into the fracture bed on the proximal phalanx. The anatomical reduction is confirmed both arthroscopically and with orthogonal fluoroscopic views. Depending on the size of the fragment, fixation can be augmented with a second K-wire to prevent rotation, or, if the fragment is sufficiently large, a cannulated headless compression screw can be utilized for definitive, rigid fixation.

Open Surgical Repair of the Collateral Ligament
When dealing with a mid-substance tear, a purely ligamentous avulsion, or a confirmed Stener lesion, an open approach is mandatory to ensure anatomical restoration and appropriate tensioning.
-
Incision and Superficial Dissection:
For a UCL repair, a lazy-S or chevron-shaped incision is centered over the ulnar aspect of the MCP joint. The apex of the incision is typically placed dorsally to avoid placing a straight scar directly over the joint flexion crease, which can lead to restrictive contractures.The skin flaps are elevated, taking great care to identify and protect the dorsal sensory branches of the ulnar nerve. These branches are mobilized and gently retracted dorsally using vessel loops. The underlying deep fascia is incised, exposing the transverse fibers of the adductor aponeurosis.
-
Identifying the Pathology and the Stener Lesion:
At this stage, the surgeon must carefully inspect the anatomy. If a Stener lesion is present, the bulbous, torn proximal stump of the UCL will be clearly visible lying superficial to the adductor aponeurosis.

To access the joint and the native footprint, the adductor aponeurosis must be incised. We typically make a longitudinal incision through the aponeurosis, parallel to the extensor tendon, leaving a sufficient cuff of tissue volarly for later robust repair. The aponeurosis is reflected volarly, exposing the underlying joint capsule and the torn ends of the collateral ligament. -
Footprint Preparation and Anchor Placement:
The joint is inspected, and any intra-articular debris or osteochondral loose bodies are removed. The anatomic footprint of the ligament—most commonly on the volar-ulnar base of the proximal phalanx—is identified. This area is meticulously decorticated using a small curette or a motorized burr to expose bleeding cancellous bone, which is essential for biological healing of the ligament-to-bone interface.A micro-suture anchor (typically 1.3 mm to 1.5 mm in diameter, loaded with high-strength non-absorbable suture) is inserted into the prepared footprint. The anchor must be placed at an angle of approximately 45 degrees to the articular surface to ensure adequate bone purchase and avoid iatrogenic penetration into the joint space.

-
Ligament Repair and Tensioning:
The sutures from the anchor are passed through the distal stump of the UCL using a locking configuration, such as a modified Krakow or Mason-Allen stitch, to ensure a secure, tear-resistant grasp of the tissue.

Crucially, the joint is held in approximately 15 to 20 degrees of flexion and slight ulnar deviation during knot tying. This position appropriately tensions the proper collateral ligament while ensuring the volar plate is not over-constrained. If the accessory collateral ligament or volar plate is also torn, these structures are incorporated into the repair or sutured separately to restore full multi-planar stability.

-
Closure and Immobilization:
Once the ligament is securely repaired, the joint is taken through a gentle range of motion to confirm stability and ensure there is no impingement. The adductor aponeurosis is then meticulously repaired over the reconstructed ligament using absorbable sutures. This layer adds an essential secondary dynamic restraint.

The skin is closed with interrupted non-absorbable sutures. A sterile dressing is applied, and the thumb is immobilized in a custom-molded, short-arm thumb spica splint, positioning the MCP joint in slight flexion and the interphalangeal joint free to encourage early tendon glide.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following thumb MCP joint collateral ligament repair can and do occur. A thorough understanding of these potential pitfalls is essential for prompt recognition and appropriate salvage management. The surgeon must counsel the patient extensively preoperatively regarding these risks.
The most frequent complication following both operative and non-operative management is persistent joint stiffness. The thumb MCP joint is notoriously prone to arthrofibrosis following trauma and immobilization. While a slight loss of terminal flexion is common and rarely impairs overall hand function, severe stiffness can be debilitating. This is mitigated by precise surgical tension
