Mastering Thumb CMC Resection Arthroplasty with FCR Suspensionplasty

Key Takeaway
This masterclass details thumb carpometacarpal (CMC) joint resection arthroplasty using FCR suspensionplasty. We'll cover comprehensive surgical anatomy, meticulous patient positioning, and a granular, step-by-step intraoperative execution. Learn crucial techniques for trapezium excision, FCR tendon harvest, and suspensionplasty to restore stability and function, while navigating potential pitfalls and ensuring excellent postoperative recovery.
Comprehensive Introduction and Patho-Epidemiology
Symptomatic basilar joint arthrosis of the thumb represents one of the most pervasive and profoundly disabling conditions encountered in hand and upper extremity surgery. When executed with precision, a deep understanding of the underlying biomechanics, and meticulous handling of soft tissues, thumb carpometacarpal (CMC) resection arthroplasty combined with flexor carpi radialis (FCR) suspensionplasty can dramatically restore a patient's quality of life. This chapter serves as an exhaustive masterclass on the pathology, surgical anatomy, and technical execution of this cornerstone procedure.
Osteoarthritis—or more accurately, osteoarthrosis—is a ubiquitous pathology within the human hand. While the distal interphalangeal (DIP) joint remains the most frequently affected articulation anatomically, arthrosis of the trapeziometacarpal (TM) joint is disproportionately debilitating. The thumb CMC joint is the functional epicenter of the hand, dictating opposition, key pinch, and power grip. Patients typically present with significant localized pain, catastrophic loss of pinch strength, and functional weakness, rendering simple activities of daily living—such as turning a doorknob, manipulating keys, or twisting a jar lid—excruciatingly difficult.
The pathogenesis of basilar thumb arthrosis is distinctly multifactorial, representing a complex interplay between biochemical degradation and biomechanical failure. Biochemically, the presence of synovial fluid cytokines, matrix metalloproteinases (MMPs), and inflammatory mediators accelerates articular cartilage degradation. Biomechanically, the joint's capacity to withstand repetitive, high-shear daily loads diminishes over time. Epidemiologically, there is a striking correlation with postmenopausal women, who exhibit an incidence rate 10 to 15 times higher than their male counterparts. This demographic predilection strongly suggests that estrogen withdrawal, or the loss of related protective hormonal compounds, alters ligamentous laxity and cartilage resilience at the cellular level.
Historically, the cornerstone of this disease process has been attributed to the attenuation of the palmar or anterior oblique ligament (AOL), frequently referred to as the "beak ligament." The AOL has long been considered the primary stabilizing ligament of the thumb CMC joint against dorsal translation. When this ligament degenerates, stretches, or becomes functionally incompetent, it initiates a predictable cascade: ligamentous laxity, abnormal dorsal translation of the thumb metacarpal on the trapezium, exponentially increased shear forces across the articular surface, and a characteristic abnormal wear pattern. Initial eburnation of the articular cartilage typically manifests along the palmar-volar aspect of the joint. As the disease progresses inexorably, global joint space narrowing occurs, marginal osteophytes develop, and eburnation extends throughout the entire biconcave articular surface, ultimately leading to fixed subluxation and the classic "shoulder sign" deformity.
Detailed Surgical Anatomy and Biomechanics
Before initiating any surgical intervention, the operating surgeon must possess a three-dimensional mastery of the thumb CMC joint anatomy. The trapeziometacarpal joint is a fascinating, highly mobile biconcave (saddle) joint. Its unique geometry affords motion in three distinct planes: flexion-extension, abduction-adduction, and pronation-supination (which combine to allow opposition). However, this extensive, multi-axial range of motion comes at a severe biomechanical cost: minimal osseous constraints. The joint relies almost entirely on its surrounding capsuloligamentous envelope for stability.
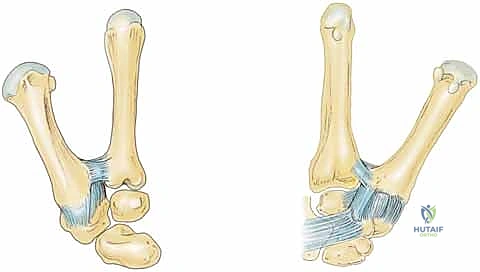
The ligamentous anatomy of the basilar joint is a complex, intricately woven network. Anatomical studies have described up to 16 distinct ligaments surrounding the thumb CMC joint, with 7 identified as the primary stabilizers of the thumb metacarpal. These core stabilizers include the superficial anterior oblique, deep anterior oblique (beak), dorsal radial, posterior oblique, ulnar collateral, intermetacarpal, and dorsal intermetacarpal ligaments. While the AOL was historically viewed as the primary restraint, modern biomechanical literature heavily emphasizes the critical importance of the Dorsal Radial Ligament (DRL) in preventing dorsal subluxation of the metacarpal base. The remaining ligaments serve to stabilize the trapezium itself within the distal carpal row, providing a rigid foundation against which the thumb can pivot.
Beyond primary idiopathic osteoarthritis, secondary arthrosis frequently develops from direct mechanical damage to the articular cartilage, such as intra-articular fractures (e.g., Bennett or Rolando fractures) or trapezial fractures. While meticulous anatomic reduction and internal fixation can minimize post-traumatic sequelae, the risk of late-onset arthrosis remains significant. Paradoxically, an unreduced or malunited Bennett fracture—by virtue of allowing proximal migration of the metacarpal shaft and functionally unloading the volar aspect of the joint—may occasionally protect against the classic patterns of future osteoarthritis, though it creates its own functional deficits.
Neurovascular Structures of Critical Importance
The surgical approach to the basilar joint places several critical neurovascular structures at immediate risk. Mastery of this regional anatomy is non-negotiable.
The Radial Artery: The radial artery courses directly through our primary surgical interval, particularly when utilizing a dorsal or dorsoradial approach. After passing deep to the abductor pollicis longus (APL) and extensor pollicis brevis (EPB), it traverses the anatomic snuffbox over the scaphoid and trapezium before diving between the two heads of the first dorsal interosseous muscle. During capsular exposure, the surgeon will encounter multiple deep perforating branches supplying the dorsal capsule. These must be meticulously identified, coagulated with bipolar electrocautery, and divided to allow the main trunk of the radial artery to be safely mobilized and retracted dorsally and ulnarly. Iatrogenic injury to the main trunk can lead to catastrophic bleeding, pseudoaneurysm formation, or vascular compromise of the digits.
The Radial Sensory Nerve (RSN): The superficial branch of the radial nerve is exquisitely vulnerable during the initial skin incision and superficial dissection. Multiple terminal branches arborize over the first dorsal compartment and the CMC joint. These branches must be identified using blunt longitudinal dissection and meticulously protected. Never skeletonize, encircle with tight vessel loops, or unnecessarily divide these branches. Iatrogenic injury, traction neuropraxia, or neuroma formation within the RSN distribution leads to debilitating postoperative radial sensory neuritis—a notoriously difficult complication to manage, which can precipitate complex regional pain syndrome (CRPS) or reflex sympathetic dystrophy (RSD).
Muscular Intervals and Osteology
The primary surgical window is developed between the extensor pollicis longus (EPL) dorsally and ulnarly, and the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) radially and volarly. Understanding the dynamic tension of these muscle-tendon units is key to efficient, safe, and self-retaining retraction. Furthermore, the flexor carpi radialis (FCR) tendon, the workhorse for our suspensionplasty, courses along the volar forearm, passing through its own fibro-osseous tunnel within the transverse carpal ligament, intimately grooving the volar aspect of the trapezium before inserting onto the base of the second metacarpal.
Osteologically, the surgeon must be intimately familiar with the trapezium, the thumb metacarpal base, and the adjacent scaphotrapezial-trapezoidal (STT) joint. The trapezium articulates with the thumb metacarpal distally, the scaphoid proximally, and the trapezoid ulnarly. During complete trapeziectomy, the surgeon must exercise extreme caution when resecting the ulnar-most aspect of the trapezium to avoid iatrogenic damage to the articular surface of the capitate or the trapezoid.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention must be predicated on a thorough clinical evaluation, radiographic staging, and the exhaustion of non-operative modalities. Patient selection is the primary determinant of surgical success in CMC arthroplasty.
Most patients should undergo a rigorous trial of conservative therapy prior to surgical consideration. This includes custom orthoplast thumb spica splinting (particularly for high-demand activities and nighttime wear), intra-articular corticosteroid injections (often performed under fluoroscopic or ultrasound guidance), non-steroidal anti-inflammatory drugs (NSAIDs), and targeted hand therapy focusing on thenar isometric strengthening and proprioceptive re-education. While these interventions do not alter the natural history of the disease or reverse cartilage loss, they frequently provide substantial symptomatic relief, allowing the patient to delay surgical intervention for years.
When conservative measures fail to provide durable relief, and the patient exhibits unacceptable pain and functional limitation, surgical intervention is indicated. The choice of procedure—hematoma distraction arthroplasty, simple trapeziectomy, trapeziectomy with ligament reconstruction and tendon interposition (LRTI), or suspensionplasty—depends on the patient's age, functional demands, and the presence of concomitant joint pathology. Suspensionplasty utilizing the FCR tendon is specifically designed to resist cantilever bending forces, prevent proximal migration (subsidence) of the thumb metacarpal, and provide superior dynamic stability compared to simple trapeziectomy, making it the gold standard for active, high-demand patients.
| Category | Specific Clinical Scenarios |
|---|---|
| Primary Indications | - Debilitating basilar joint pain refractory to >6 months of conservative management. - Significant loss of key pinch and grip strength impacting ADLs. - Radiographic evidence of Eaton-Littler Stage II, III, or IV disease. - Fixed dorsal subluxation of the thumb metacarpal base. |
| Absolute Contraindications | - Active local or systemic infection. - Medically unstable patient unfit for elective surgery. - Patient inability or unwillingness to comply with strict postoperative rehabilitation. - Charcot arthropathy of the basilar joint. |
| Relative Contraindications | - Isolated Eaton Stage I disease (consider extra-articular ligament reconstruction or arthroscopic debridement first). - Severe, unaddressed cervical radiculopathy mimicking distal symptoms. - Concomitant, uncorrected severe MCP joint hyperextension (>30 degrees). |
Addressing Concomitant MCP Joint Pathology
A critical aspect of preoperative decision-making is the evaluation of the metacarpophalangeal (MCP) joint. In advanced basilar arthrosis, the thumb metacarpal subluxates dorsally and adducts. To clear the thumb for grasp, the patient compensatory hyperextends the MCP joint, gradually attenuating the volar plate and leading to a fixed "zig-zag" deformity.
If dynamic collapse or fixed hyperextension of the MCP joint exceeds 30 degrees during key pinch, it must be addressed concurrently with the CMC arthroplasty. Failure to correct MCP hyperextension will result in persistent abnormal biomechanics, driving the base of the metacarpal proximally into the trapezial void, leading to early failure of the suspensionplasty. Depending on the severity and flexibility of the deformity, concomitant procedures may include EPB tendon transfer, volar plate capsulodesis, or formal MCP joint arthrodesis.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning ensures a seamless intraoperative workflow and minimizes the risk of unforeseen complications. This begins with a meticulous radiographic assessment to accurately stage the disease process and evaluate surrounding articulations.
Radiographic Assessment and Staging
Standard posteroanterior (PA) and lateral views of the hand are insufficient for evaluating the basilar joint due to its 30-degree pronated position relative to the rest of the carpus. We require dedicated thumb views: a pronated AP (Robert view), a true lateral of the thumb, and a 30-degree PA stress view. The stress view, obtained by having the patient forcefully press the tips of their thumbs together, is invaluable for unmasking dynamic dorsal subluxation and assessing the competence of the capsuloligamentous envelope.

We utilize the Eaton and Littler radiographic staging system to guide our surgical approach. However, the operating surgeon must always critically evaluate the scaphotrapezial-trapezoidal (STT) joint. As emphasized by Tomaino et al., failure to recognize and address STT arthritis (Stage V disease) is a primary cause of persistent postoperative pain following isolated CMC procedures.
- Stage I: Normal-appearing articular surfaces or slight widening of the joint space, indicative of synovitis and early ligamentous laxity.
- Stage II: Joint space narrowing with the formation of marginal osteophytes smaller than 2 mm.
- Stage III: Advanced joint space narrowing, subchondral sclerosis, and osteophytes larger than 2 mm.
- Stage IV: Pan-trapezial disease involving advanced arthrosis of both the TM joint and the scaphotrapezial joint.
- Stage V (Tomaino modification): Stage IV appearance with the addition of advanced narrowing, sclerosis, or osteophytes within the scaphotrapezoid articulation.
Patient Positioning and Operating Room Setup
The patient is positioned supine on the operating table. The operative upper extremity is extended onto a radiolucent hand table. Meticulous padding is applied to all bony prominences. A well-padded pneumatic tourniquet is placed on the proximal arm. Regional anesthesia (e.g., supraclavicular or axillary brachial plexus block) is highly recommended, as it provides excellent intraoperative muscle relaxation and profound postoperative analgesia, minimizing the need for systemic opioids.
The arm is prepped and draped in a standard sterile fashion. The surgeon sits in the axilla, facing the hand, while the assistant sits opposite. Intraoperative fluoroscopy (mini C-arm) must be readily available and positioned to allow unimpeded access to the surgical field without compromising sterility. Prior to inflation of the tourniquet, the limb is exsanguinated using an Esmarch bandage, and the tourniquet is inflated to 250 mmHg (or 100 mmHg above systolic pressure).
Step-by-Step Surgical Approach and Fixation Technique
The execution of a resection arthroplasty with FCR suspensionplasty requires a choreographed sequence of precise surgical maneuvers. The goal is complete excision of the offending osteoarthritic surfaces while reconstructing a robust, dynamic ligamentous suspension to prevent metacarpal subsidence.
1. Incision and Superficial Dissection
We begin with a triradiate or Wagner-type incision centered over the anatomic snuffbox and the base of the thumb metacarpal. I prefer the triradiate approach as it provides expansive exposure of the dorsal capsule and facilitates proximal visualization of the STT joint. If a concomitant first dorsal compartment release (De Quervain's release) is anticipated, a slightly more volar longitudinal incision may be preferred.
As the skin is incised, extreme vigilance is required. The superficial branches of the radial sensory nerve (RSN) reside immediately deep to the dermis in the subcutaneous fat. Using fine tenotomy scissors and blunt spreading techniques, these branches are meticulously identified, mobilized gently, and retracted. Small vein retractors or vessel loops (applied loosely) can be used to protect the RSN branches, ensuring they are kept out of the working field without inducing traction neuropraxia.
If the patient presents with a prominent "shoulder sign" (fixed dorsal subluxation of the metacarpal base), the distorted anatomy can obscure the true location of the CMC joint. In such instances, palpation of the scaphoid tuberosity proximally and the rigid shaft of the metacarpal distally will help re-orient the surgeon and ensure the incision is accurately centered over the trapezium.
2. Deep Exposure and Radial Artery Mobilization
Deep exposure is achieved by developing the interval between the extensor pollicis longus (EPL) dorsally and the abductor pollicis longus (APL) / extensor pollicis brevis (EPB) volarly. Senn or Ragnell retractors are placed beneath these tendinous structures to open the interval down to the dorsal joint capsule.

Within this interval, the main trunk of the radial artery is identified coursing obliquely over the capsule. The artery is tethered to the capsule by several small, deep perforating vessels. Using micro-bipolar electrocautery, these perforators are meticulously coagulated and divided. This critical step untethers the radial artery, allowing it to be safely swept dorsally and ulnarly using a blunt retractor. Failure to adequately mobilize the radial artery drastically increases the risk of iatrogenic laceration during capsulotomy or trapezial excision.
3. Capsulotomy and Metacarpal Base Preparation
With the radial artery safely protected, a longitudinal capsulotomy is performed directly over the midline of the CMC joint, extending proximally to expose the scaphotrapezial joint. The capsular flaps are elevated subperiosteally using a sharp Freer elevator or a small surgical blade. Heavy 3-0 Vicryl tag sutures or small sharp retractors are used to retract the capsular flaps, providing a panoramic view of the trapezial articulations.
Before attempting to excise the trapezium, it is highly advantageous to address the base of the thumb metacarpal. Using an oscillating microsagittal saw, a thin, 2-3 millimeter transverse sliver of bone is resected from the proximal articular surface of the metacarpal base.

This maneuver serves three critical purposes: First, it removes the eburnated, osteoarthritic cartilage of the metacarpal. Second, it creates a flat, bleeding cancellous bone surface that will eventually interface with the tendon interposition. Third, and most importantly, it dramatically increases the working space within the joint, facilitating access to the distal pole of the trapezium and allowing for a much safer subsequent trapeziectomy.
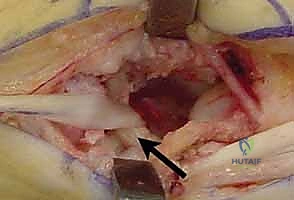
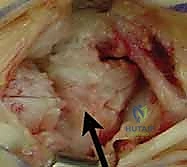
4. Complete Trapeziectomy
Excision of the trapezium is the most technically demanding portion of the procedure. The goal is complete removal of the bone without damaging the underlying FCR tendon, the adjacent capitate, or the scaphoid.

The trapezium can be removed en bloc or piecemeal. I strongly advocate for a piecemeal resection using a combination of a small osteotome, rongeurs, and a high-speed burr. An osteotome is used to split the trapezium longitudinally. The fragments are then carefully grasped with a towel clip or heavy rongeur and avulsed from their deep volar ligamentous attachments.
As the volar and ulnar aspects of the trapezium are approached, the surgeon must exercise extreme caution. The FCR tendon lies immediately deep to the trapezium within its fibro-osseous groove. Aggressive use of osteotomes or rongeurs in this area can easily lacerate the FCR tendon, compromising the suspensionplasty. Furthermore, the ulnar border of the trapezium articulates intimately with the trapezoid and capitate; indiscriminate resection here can cause iatrogenic arthrosis of the midcarpal joint.

Once the trapezium is completely excised, the void is thoroughly irrigated and inspected. Any remaining osteophytes on the scaphoid or trapezoid are debrided. The FCR tendon must be directly visualized in the depth of the wound to confirm its integrity.
5. FCR Tendon Harvest and Preparation
Attention is now turned to harvesting the FCR tendon. Depending on surgeon preference and the patient's anatomy, either the entire thickness or the radial half of the FCR tendon can be harvested. Utilizing the entire tendon provides a more robust construct for suspension and interposition, and rarely results in clinically significant wrist flexion weakness.

A series of short transverse incisions (or one longitudinal incision) is made along the volar aspect of the distal forearm, following the course of the FCR tendon. The tendon is identified, and its sheath is opened. The tendon is transected proximally at the musculotendinous junction (typically 10-12 cm proximal to the wrist crease).

The proximal end of the harvested tendon is tagged with a grasping suture (e.g., 2-0 Ethibond or FiberWire). The tendon is then carefully dissected distally, releasing it from its fascial attachments, until it is delivered directly into the trapezial void at the base of the thumb. The tendon must be completely freed to its insertion on the base of the second metacarpal to allow for a direct, unhindered line of pull during the suspensionplasty.
6. Metacarpal Bone Tunnel Creation
To recreate the stabilizing vector of the anterior oblique ligament and suspend the thumb, a bone tunnel must be created through the base of the thumb metacarpal.

Using a power drill and a 3.2 mm or 4.0 mm drill bit (sized to accommodate the thickness of the harvested FCR tendon), a tunnel is created. The entry point is located on the dorsal-radial aspect of the metacarpal shaft, approximately 1.5 cm distal to the resected base. The drill is directed obliquely and proximally, exiting squarely within the center of the resected cancellous surface of the metacarpal base.
Care must be taken to ensure the cortical bridges surrounding the tunnel are robust enough to withstand the tension of the suspensionplasty without fracturing. The edges of the tunnel are chamfered slightly with a curette to prevent fraying or abrasion of the tendon.
7. Suspensionplasty, Tensioning, and Anchoring
The tagged proximal end of the FCR tendon is now passed through the metacarpal bone tunnel.

A wire loop or a specialized tendon passer is inserted retrograde from the dorsal-radial cortex, down through the tunnel, and out the metacarpal base. The suture attached to the FCR tendon is captured and pulled through the tunnel, delivering the tendon out the dorsal aspect of the metac
Clinical & Radiographic Imaging Archive