Mastering Tendon Transfers for Ulnar Nerve Palsy: An Intraoperative Guide

Key Takeaway
This masterclass guides fellows through tendon transfers for ulnar nerve palsy, focusing on restoring thumb adduction and correcting claw deformity. We meticulously cover surgical anatomy, patient positioning, and step-by-step intraoperative execution, including brachioradialis-to-APB transfer and FPL-EPL tenodesis. Critical pearls, potential pitfalls, and comprehensive postoperative care are emphasized, ensuring a thorough understanding of this intricate hand procedure.
Comprehensive Introduction and Patho-Epidemiology
The restoration of function following ulnar nerve palsy remains one of the most intellectually demanding and technically unforgiving challenges in upper extremity reconstructive surgery. The ulnar nerve is often designated the "musician's nerve" or the "nerve of fine movements," and its loss systematically dismantles the intricate biomechanical balance of the human hand. When managing these complex cases, the orthopedic surgeon is not merely redirecting tendons; we are fundamentally re-engineering the hand’s force vectors to restore the critical abilities to pinch, grasp, and interact with the physical world. A profound, three-dimensional understanding of hand anatomy, dynamic biomechanics, and meticulous surgical execution is paramount to achieving a durable, functional outcome.
Ulnar nerve palsy, whether originating from a high lesion (proximal to the elbow) or a low lesion (at or distal to the wrist), presents a unique reconstructive paradigm due to the simultaneous loss of critical sensory feedback and intrinsic motor function. The epidemiological profile of ulnar neuropathy spans a wide spectrum, encompassing acute traumatic lacerations, chronic compressive neuropathies (such as cubital tunnel or Guyon's canal syndromes), traction injuries, and systemic neuropathic conditions. Regardless of the etiology, the resulting motor deficit produces a predictably devastating pattern: profound weakness in key pinch, marked reduction in grip strength, and the development of debilitating secondary deformities, most notably the classic claw hand.
The primary goals of reconstructive tendon transfers in this setting are to compensate for the paralyzed intrinsic musculature. Specifically, we aim to restore thumb adduction for powerful lateral pinch, provide active metacarpophalangeal (MCP) joint flexion to correct the claw deformity of the ring and small fingers, and integrate these isolated movements into a synchronized, functional grasp. This masterclass chapter is designed to guide the advanced surgical trainee and practicing hand surgeon through the exhaustive preoperative assessment, the nuanced surgical anatomy, and the precise intraoperative execution required to master these reconstructive procedures.
Achieving a successful outcome requires more than technical proficiency; it demands rigorous preoperative planning and an unyielding adherence to the biomechanical principles of tendon transfer. We must carefully select donor muscles that possess adequate strength and excursion, ensure a straight line of pull, and establish synergistic firing patterns whenever possible. Furthermore, the absolute prerequisite of supple, contracture-free joints cannot be overstated. As we delve into the specific techniques, remember that our ultimate objective is not anatomical perfection, but the maximal restoration of independent, purposeful hand function.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel is ever utilized, the reconstructive surgeon must possess an encyclopedic knowledge of the ulnar nerve's anatomical course, its motor and sensory distributions, and the profound biomechanical consequences of its absence. This foundational knowledge dictates donor selection, routing pathways, and the anticipation of compensatory anomalies.
The Ulnar Nerve Motor and Sensory Distribution
The ulnar nerve is the terminal continuation of the medial cord of the brachial plexus, deriving its fibers primarily from the C8 and T1 nerve roots. It is a mixed peripheral nerve carrying essential motor and sensory fascicles. In the arm, the ulnar nerve descends without providing any motor branches, piercing the medial intermuscular septum to enter the posterior compartment before traveling behind the medial epicondyle. As it enters the forearm through the cubital tunnel, passing between the two heads of the flexor carpi ulnaris (FCU), it begins its motor innervation sequence.
Immediately distal to the elbow, the nerve supplies the FCU and subsequently the ulnar half of the flexor digitorum profundus (FDP), which drives the distal interphalangeal (DIP) joint flexion of the ring and small fingers. A lesion proximal to these branches constitutes a high ulnar nerve palsy. As the nerve progresses distally, it enters the hand through Guyon's canal, where it bifurcates into superficial sensory and deep motor branches. This deep motor branch is the lifeblood of the hand's intrinsic musculature. It innervates the hypothenar muscles (abductor digiti minimi, flexor digiti minimi, opponens digiti minimi), the ulnar two lumbricals, all dorsal and palmar interossei, the adductor pollicis, and the deep head of the flexor pollicis brevis (FPB).
The sensory distribution is equally critical for hand function. The ulnar nerve provides sensation to the entire small finger and the ulnar half of the ring finger. Crucially, the dorsal sensory branch of the ulnar nerve arises approximately 5 to 8 centimeters proximal to the wrist crease, coursing dorsally to supply the ulnar dorsum of the hand. A clinical pearl of immense localizing value: preservation of dorsal ulnar sensation in the presence of intrinsic motor and volar sensory deficits definitively localizes the lesion to Guyon's canal (a low palsy), as the dorsal sensory branch exits proximal to this anatomic bottleneck.
Anomalous Innervation and Compensatory Mechanisms
The peripheral nervous system is notorious for its anatomical variations, and the ulnar nerve is no exception. Understanding these anomalies is vital, as they can obscure the clinical picture and confound electrodiagnostic studies. The Martin-Gruber anastomosis, occurring in the forearm, involves motor fascicles crossing from the median nerve to the ulnar nerve. Depending on the specific subtype, a complete ulnar nerve transection at the elbow might still present with functioning intrinsic muscles in the hand if they receive crossover innervation from the median nerve.
Conversely, the Riche-Cannieu anastomosis occurs in the palm, representing a connection between the deep motor branch of the ulnar nerve and the recurrent motor branch of the median nerve. This can result in the ulnar nerve innervating typical median nerve territories (such as the thenar musculature) or vice versa. These variations underscore the necessity of a meticulous, muscle-by-muscle physical examination rather than relying solely on generalized patterns of weakness.

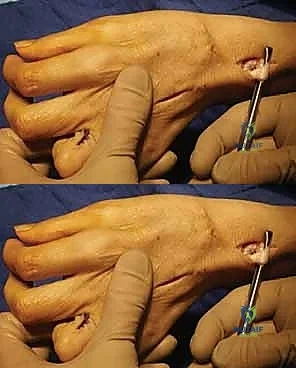
When the ulnar nerve fails, the hand attempts to compensate, leading to pathognomonic clinical signs. The Froment sign (illustrated above) is a classic example. When a patient with ulnar palsy attempts a forceful lateral pinch, the paralyzed adductor pollicis cannot stabilize the thumb MCP joint. To compensate, the patient recruits the median-innervated flexor pollicis longus (FPL), resulting in hyperflexion of the thumb interphalangeal (IP) joint. Concurrently, the Jeanne sign may manifest as reciprocal hyperextension of the thumb MCP joint due to the unopposed action of the extensor pollicis brevis and longus.
Biomechanics of the Claw Hand Deformity
The most visually striking and functionally debilitating consequence of ulnar nerve palsy is the claw hand deformity (Duchenne sign). This posture is characterized by hyperextension of the MCP joints and flexion of the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints of the ring and small fingers. To correct this, one must understand the biomechanics of the "intrinsic minus" state.

Normally, the lumbricals and interossei flex the MCP joints and extend the IP joints. They act as a vital dynamic link between the extrinsic flexors and extensors. When these intrinsics are paralyzed, the extrinsic extensor digitorum communis (EDC) acts unopposed on the proximal phalanx, driving the MCP joint into hyperextension. Because the EDC's excursion is exhausted by hyperextending the MCP joint, it cannot effectively transmit force to the central slip and lateral bands to extend the PIP and DIP joints. Consequently, the resting tone of the FDP and FDS pulls the IP joints into flexion.
Interestingly, the claw deformity is paradoxically more pronounced in a low ulnar nerve palsy compared to a high palsy. This is known as the ulnar paradox. In a low palsy, the FDP to the ring and small fingers remains innervated, exerting a strong, unopposed flexing force on the IP joints. In a high palsy, the ulnar-innervated FDP is also paralyzed, reducing the flexion force on the IP joints and resulting in a less severe resting claw posture. Over time, regardless of the level, the volar plate of the MCP joint attenuates, and the PIP joint can develop rigid flexion contractures, drastically complicating surgical reconstruction.
Exhaustive Indications and Contraindications
The decision to proceed with reconstructive tendon transfers must be predicated on a rigorous evaluation of the patient's neurological status, functional deficits, and anatomical suitability. Tendon transfers are salvage procedures; they are permanent biomechanical alterations designed to mask an underlying neurological deficit. Therefore, timing and patient selection are the ultimate determinants of success.
| Variable | Favorable Indications for Transfer | Absolute/Relative Contraindications |
|---|---|---|
| Neurological Status | Irreparable nerve injury; No clinical/EMG recovery > 12 months post-repair. | Progressive neurological disease (e.g., ALS); Early phase of recovery (< 6 months). |
| Joint Mobility | Supple, full passive range of motion in all affected digits. | Fixed flexion contractures (especially PIP joints > 45 degrees); Severe joint arthrosis. |
| Donor Muscle | Synergistic, expendable, Medical Research Council (MRC) Grade 4 or 5 strength. | Spasticity; Co-contracting muscles; MRC Grade < 4; Previous injury to donor muscle. |
| Soft Tissue Envelope | Healthy, pliable skin; adequate subcutaneous fat for tendon gliding. | Severe scarring; active infection; compromised vascularity; inadequate soft tissue coverage. |
| Patient Factors | Compliant, highly motivated, cognitively intact to participate in complex rehab. | Poor compliance; severe cognitive impairment; unrealistic expectations. |
Timing of Intervention and Patient Selection
The timing of tendon transfer surgery is a delicate balance. If a nerve repair or grafting has been performed, or if a compressive neuropathy has been decompressed, the surgeon must allow adequate time for axonal regeneration. Nerve regeneration occurs at approximately 1 millimeter per day. Therefore, depending on the distance from the lesion to the motor endplates, a period of 6 to 12 months or longer may be required before declaring the nerve irreparably damaged. Serial clinical examinations and electromyography (EMG) are critical during this waiting period to detect subclinical reinnervation.
However, early or "internal splinting" tendon transfers may be indicated in specific scenarios. If the nerve injury is deemed completely irreparable at the time of trauma (e.g., massive avulsion injuries), early tendon transfers can prevent the development of secondary joint contractures and immediately improve hand function. Furthermore, in patients who present late with severe, established clawing, an early transfer to block MCP hyperextension can prevent irreversible stretching of the volar plate and central slip, even while awaiting potential nerve recovery.
Clinical Examination and Diagnostic Modalities
A meticulous physical examination is the cornerstone of preoperative planning. The surgeon must systematically evaluate the strength of every potential donor muscle. The Boyes criteria dictate that a donor muscle must have at least Grade 4 (out of 5) strength, as a muscle typically loses one grade of strength following transfer. Furthermore, the excursion of the donor muscle must match the functional requirements of the recipient site.

The Bouvier maneuver is an indispensable clinical test used to assess the integrity of the extensor mechanism and guide the surgical plan for claw correction. The surgeon passively blocks the MCP joints of the affected fingers in slight flexion, preventing the hyperextension deformity. The patient is then asked to actively extend their PIP joints. If the patient can fully extend the PIP joints (a positive Bouvier test), the central slip and lateral bands are intact. In this scenario, the surgical reconstruction only needs to provide a volar force to block MCP hyperextension (e.g., a Zancolli lasso procedure).

Conversely, if the patient cannot actively extend the PIP joints even when the MCP joint is stabilized (a negative Bouvier test), this indicates that the central slip has become attenuated or stretched due to chronic flexion. In this more complex scenario, simply blocking the MCP joint will not restore finger extension. The surgeon must select a tendon transfer that routes the donor tendon directly into the lateral bands (e.g., a modified Stiles-Bunnell or Brand transfer) to actively provide PIP joint extension.
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning for ulnar nerve palsy reconstruction is akin to architectural drafting; every vector, tension line, and fixation point must be conceptualized before entering the operating theater. The failure of a tendon transfer is rarely due to intraoperative technical errors, but rather due to flawed preoperative strategy, poor donor selection, or unrecognized joint contractures.
Donor Selection Principles
Selecting the appropriate donor muscle requires adherence to established biomechanical principles. First and foremost is the principle of "one tendon, one function." A single transferred tendon cannot be expected to simultaneously perform two distinct, opposing actions. If multiple functions are required (e.g., thumb adduction and claw correction), multiple donor tendons must be utilized.
The concept of synergism is also critical for postoperative motor re-education. Synergistic muscles normally fire together during a specific functional movement. For example, wrist extensors naturally fire during finger flexion to stabilize the wrist and optimize the length-tension relationship of the flexors. Therefore, utilizing a wrist extensor (like the ECRB or ECRL) as a donor to restore finger flexion or thumb adduction capitalizes on these pre-existing neural pathways, making postoperative rehabilitation significantly easier for the patient.
Excursion—the linear distance a tendon travels during maximal muscle contraction—must also be matched. A wrist extensor typically has an excursion of 3-4 cm, while finger flexors require 5-7 cm. If a low-excursion donor is used for a high-excursion requirement, the patient will experience a limited range of motion. Finally, the donor tendon must be routed in a straight line of pull. Sharp angles or pulleys increase friction, decrease the effective force of the transfer, and increase the risk of tendon rupture or adhesion.
Anesthesia, Positioning, and Tourniquet Control
Tendon transfer surgery is typically performed under regional anesthesia (supraclavicular or axillary brachial plexus block) combined with intravenous sedation, or under general anesthesia. Regional anesthesia is highly preferred as it provides excellent intraoperative muscle relaxation and profound postoperative analgesia, which is crucial for early mobilization protocols.
The patient is positioned supine with the operative extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Prior to exsanguination, the surgeon must carefully assess the resting tension and cascade of the hand. Once the arm is prepped and draped in a standard sterile fashion, the limb is exsanguinated with an Esmarch bandage, and the tourniquet is inflated to 250 mm Hg (or 100 mm Hg above systolic pressure).
Meticulous hemostasis is absolutely critical in tendon transfer surgery. Hematoma formation in the tendon bed leads to severe fibroblastic proliferation, resulting in dense adhesions that will tether the transfer and doom the functional outcome. Therefore, many surgeons prefer to release the tourniquet prior to final skin closure to ensure absolute hemostasis, particularly after extensive soft tissue dissection and tendon routing.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of ulnar nerve palsy reconstruction is modular, typically addressing three primary functional deficits: loss of powerful key pinch (thumb adduction), the claw deformity of the fingers (loss of intrinsic MCP flexion/IP extension), and the abducted posture of the small finger (Wartenberg sign).
Restoration of Key Pinch and Thumb Adduction
The loss of the adductor pollicis profoundly weakens lateral pinch, making tasks like turning a key or holding a pen incredibly difficult. Several transfers exist to restore this function, but the extensor carpi radialis brevis (ECRB) or the flexor digitorum superficialis (FDS) of the ring or middle finger are the most commonly utilized donors.

The Smith-Hastings Transfer (ECRB to Adductor Pollicis):
This is a highly favored, synergistic transfer. An incision is made over the dorsal wrist to harvest the ECRB tendon at its insertion on the base of the third metacarpal. A second incision is made in the mid-forearm to retrieve the ECRB tendon. To provide sufficient length to reach the thumb, a tendon graft (typically the palmaris longus or a strip of fascia lata) is woven into the ECRB.

The routing of this transfer is critical. The tendon graft is routed from the dorsal forearm, through the interosseous space (typically between the second and third metacarpals), and directed volarly across the palm. It must pass deep to the flexor tendons and the median nerve to replicate the transverse vector of the native adductor pollicis.

The insertion point is the adductor tubercle on the ulnar base of the thumb proximal phalanx. Fixation can be achieved using a bone anchor, an interference screw, or by weaving the graft into the tendon of the adductor pollicis. Tensioning is performed with the wrist in neutral, the thumb in full adduction, and the IP joint in extension.

The FDS Transfer (Boyes Transfer):
Alternatively, the FDS of the ring or middle finger can be used. The FDS is harvested just proximal to the A1 pulley. It is then routed transversely across the palm, deep to the flexor tendons, and inserted into the adductor tubercle. This transfer is excellent because it requires no tendon graft and provides a strong, robust motor. However, harvesting the FDS can slightly weaken grip strength and may contribute to a PIP joint extension deficit in the donor finger.
Correction of the Claw Deformity (Intrinsic Replacement)
The surgical strategy for claw correction is dictated entirely by the preoperative Bouvier maneuver. The goal is to provide a volar flexion force at the MCP joint, which subsequently allows the extrinsic extensors to effectively extend the IP joints.

The Zancolli Lasso Procedure (For Positive Bouvier):
If the central slip is intact, the Zancolli lasso is the procedure of choice. It is elegant, reliable, and technically straightforward. The FDS tendon of the affected finger (usually ring and small) is harvested at the level of the proximal phalanx.

The tendon is then pulled proximally into the palm. The critical step involves routing the distal end of the FDS tendon volarly through the A1 pulley of its respective digit, folding it back onto itself, and suturing it under tension.

By securing the FDS to the A1 pulley, the surgeon creates a dynamic tenodesis. When the flexor muscle belly contracts, it pulls on the A1 pulley, forcing the MCP joint into flexion. This prevents the hyperextension deformity and allows the native EDC to extend the PIP and DIP joints. Tensioning is set to hold the MCP joint in approximately 30 to 40 degrees of flexion with the wrist in neutral.

The Brand Transfer (For Negative Bouvier):
If the central slip is stretched (negative Bouvier), a transfer must be routed to the lateral bands to actively extend the PIP joint. The Brand transfer utilizes the extensor carpi radialis longus (ECRL) or ECRB. Because the wrist extensors are too short to reach the fingers, a free tendon graft (plantaris or split palmaris longus) is required. The graft is attached to the ECRL/ECRB in the forearm.

The graft is split into multiple slips (one for each paralyzed finger). These slips are routed dorsally, passing volar to the deep transverse metacarpal ligament (crucial to provide the flexion moment at the MCP joint), and then directed dorsally to insert into the radial lateral band of the proximal phalanx.
This routing perfectly mimics the path of the native lumbrical muscle. Tensioning is extremely delicate; it must be tight enough to correct the claw but not so tight as to create a swan neck deformity (PIP hyperextension and DIP flexion).
Addressing the Wartenberg Sign and Finger Abduction
The Wartenberg sign—the persistent abduction of the small finger—is caused by the unopposed pull of the extensor digiti minimi (EDM) in the absence of the third palmar interosseous muscle. This can be a significant nuisance, causing the small finger to catch on pockets or objects.

Correction is typically achieved by redirecting the deforming force. The EDM tendon is identified over the dorsal wrist and divided proximally. It is then routed volarly, passing deep to the deep transverse metacarpal ligament between the ring and small fingers. It is then inserted into the radial collateral ligament of the small finger MCP joint or the radial base of the proximal phalanx. By routing the tendon volarly, it is converted from an abductor/extensor into an adductor/flexor, effectively centralizing the small finger and contributing to claw correction.
Complications, Incidence Rates, and Salvage Management
Despite meticulous planning and flawless execution, tendon transfers for ulnar nerve palsy carry a distinct risk profile. The surgeon must be prepared to manage complications ranging from minor tensioning errors to catastrophic tendon ruptures.
| Complication | Estimated Incidence | Etiology / Pathophysiology | Salvage Management Strategy |
|---|---|---|---|
| Tendon Adhesions | 10 - 15% | Poor hemostasis; rough tissue handling; delayed mobilization; inadequate soft tissue bed. | Intensive hand therapy; tenolysis if no improvement after 6 months of dedicated therapy. |
| Recurrent Clawing (Under-tensioning) | 5 - 10% | Tendon stretching at the repair site; initial tension set too loose; failure to recognize negative Bouvier. | Revision surgery; retensioning of the transfer; conversion to a lateral band insertion if central slip is incompetent. |
| Swan Neck Deformity (Over-tensioning) | 3 - 8% | Transfer to lateral band tensioned too tightly, overpowering the volar plate; intrinsic plus posture. | Volar plate capsulodesis; central slip tenotomy; lengthening of the transferred tendon. |
| Tendon Rupture | < 2% | Aggressive early mobilization; weak suture technique (failure to use Pulvertaft weave); infection. | Immediate surgical re-exploration and repair; potential need for new tendon graft if ends are retracted/frayed. |
| Joint Stiffness | 5 - 12% | Prolonged immobilization; pre-existing unrecognized contractures; complex regional pain syndrome (CRPS). | Aggressive therapy; serial casting; eventual surgical joint release (capsulectomy) if refractory. |
Intraoperative and Early Postoperative Complications
The most critical intraoperative error is incorrect tensioning. The resting posture of the hand on the operating table under the tourniquet is the best indicator of appropriate tension. If a claw correction transfer is tensioned too loosely, the transfer will stretch out during the healing phase, resulting in recurrent clawing and a failure to restore grip strength. Conversely, if a lateral band transfer (like the Brand procedure) is tensioned too tightly, it will overpower the PIP joint, driving it into hyperextension and causing a secondary swan neck deformity, which is often more functionally debilitating than the original claw.
Early postoperative complications include hematoma formation and infection. Hematomas act as a biological glue, inciting a massive inflammatory response that leads to dense, restrictive adhesions. Meticulous hemostasis prior to closure and the judicious use of drains are preventative mandates. If an infection occurs, it threatens the integrity of the tendon weave and can lead to rupture. Prompt surgical debridement and targeted intravenous antibiotics are required.
Long-Term Failures and Salvage Procedures
Long-term failure is typically defined by a loss of functional excursion due to adhesions or progressive attenuation of the transfer. If a patient presents months later with restricted motion despite aggressive hand therapy,
