Dupuytren's Disease Fasciectomy: A Masterclass in Palmar and Digital Reconstruction

Key Takeaway
Welcome, fellows, to an immersive operative masterclass on Dupuytren's disease. We'll meticulously dissect the complex palmar anatomy, execute precise fasciectomy techniques, and navigate critical neurovascular structures. This session emphasizes real-time decision-making, meticulous dissection, and advanced strategies for managing contractures and preventing recurrence, ensuring optimal patient outcomes. Prepare to scrub in and master this challenging condition.
Comprehensive Introduction and Patho-Epidemiology
Welcome, esteemed colleagues and surgical fellows, to the operating theater. Today, we embark on a masterclass dedicated to the surgical management of Dupuytren's disease (DD), a condition that, while seemingly straightforward upon superficial inspection, demands our utmost respect, meticulous technical precision, and a profound, three-dimensional understanding of palmar and digital hand anatomy. This is not merely another inflammatory or neoplastic disorder; it is a unique, relentless fibroproliferative process affecting the palmar fascial complex, leading to progressive, often debilitating digital contracture. While it shares some cellular and biochemical characteristics with normal wound healing—specifically the proliferation of myofibroblasts and the deposition of collagen—the relentless, unchecked proliferation and abnormal, chaotic collagen deposition observed in Dupuytren’s disease are truly astonishing and pathognomonic.
The epidemiology of Dupuytren’s disease reveals a striking predilection for individuals of Northern European descent, earning it the historical moniker of the "Viking disease." However, its global prevalence is significant, affecting millions worldwide. The disorder exhibits a strong male predominance, particularly in earlier decades of life, with men typically presenting in their fifth or sixth decade, while women often present a decade later with a generally less aggressive clinical course. The concept of "Dupuytren's diathesis," originally popularized by Hueston, is critical for preoperative prognostication. Patients exhibiting the diathesis—characterized by early age of onset (under 50 years), bilateral hand involvement, a strong family history, and the presence of ectopic fibroproliferative manifestations such as Ledderhose disease (plantar fibromatosis), Peyronie's disease (penile fibromatosis), and Garrod's pads (dorsal knuckle pads)—are at a substantially higher risk for both aggressive disease progression and postoperative recurrence.
At the cellular level, the primary protagonist in the pathogenesis of DD is the myofibroblast. Unlike normal fibroblasts, these specialized cells express alpha-smooth muscle actin (α-SMA), granting them contractile properties akin to smooth muscle cells. The local cytokine milieu in the diseased palmar fascia is highly abnormal, characterized by elevated levels of transforming growth factor-beta 1 (TGF-β1), basic fibroblast growth factor (bFGF), and platelet-derived growth factor (PDGF). TGF-β1, in particular, is the master regulator, driving the differentiation of fibroblasts into myofibroblasts and stimulating the overproduction of extracellular matrix proteins. Furthermore, the normal architectural ratio of collagen is inverted; while normal fascia is predominantly composed of Type I collagen, Dupuytren's tissue exhibits a massive upregulation of Type III collagen, leading to the dense, disorganized, and mechanically inferior tissue that forms the characteristic cords.
The Pathogenesis of Contracture: From Nodule to Cord
The natural history of Dupuytren's disease is classically divided into three distinct histological phases: the proliferative phase, the involutional phase, and the residual phase. The hallmark of the early, proliferative phase is the appearance of the Dupuytren nodule, a highly cellular, highly vascularized mass of proliferating myofibroblasts typically arising in the distal palm. As the disease transitions into the involutional phase, the myofibroblasts begin to align along the lines of tension, actively contracting the surrounding tissue and laying down dense bands of Type III collagen. Finally, in the residual phase, the cellularity decreases dramatically, leaving behind thick, acellular, and unyielding pathological cords. It is the progressive shortening of these cords, which invariably involve the palmar, palmodigital, or digital regions, that leads to the characteristic flexion deformities of the metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints.

Detailed Surgical Anatomy and Biomechanics
Fellows, before we even contemplate making an incision, a thorough, exhaustive understanding of the normal and pathological palmar fascial complex is paramount. This intricate, multi-layered network is the precise anatomical battlefield where Dupuytren's disease wreaks havoc. It is also the treacherous terrain where we will be operating, often dissecting mere millimeters away from vital, easily injured neurovascular structures. The fundamental concept to grasp is that Dupuytren's cords do not arise de novo; rather, they represent the pathological hypertrophy, contracture, and transformation of pre-existing, normal fascial bands.
The Palmar Fascial Complex Components
The normal palmar fascial complex is a highly specialized architectural structure designed to stabilize the palmar skin during grasping while protecting underlying neurovascular and tendinous structures. It comprises the radial, ulnar, and central aponeuroses, as well as the palmodigital and digital fascia.
The Radial Aponeurosis encompasses the thenar fascia, which is an extension of the central aponeurosis over the thenar musculature. It contains the thumb pretendinous band, which, while often small or entirely absent in normal anatomy, can pathologically hypertrophy to form a cord causing severe thumb MCP flexion deformity. Furthermore, the distal and proximal commissural ligaments located here give rise to the respective commissural cords, which are the primary culprits in first web space contracture. The Ulnar Aponeurosis includes the hypothenar muscle fascia and the consistently substantial pretendinous band to the small finger, a highly common site for aggressive cord formation. It also features the abductor digiti minimi (ADM) confluence, the origin point for the isolated ADM cord.
The Central Aponeurosis is the absolute core epicenter of Dupuytren's disease activity. It is anatomically triangular, with a proximal apex continuous with the palmaris longus tendon (when present) and the flexor retinaculum.


Its longitudinal fibers fan out distally as distinct pretendinous bands to the central three digits. Crucially, as each band approaches the MCP joint, it bifurcates distally into three distinct layers: a superficial layer that inserts directly into the overlying dermis (responsible for the characteristic skin pitting seen early in the disease), a middle layer that continues distally as the spiral band into the digit, and a deep layer that passes vertically and dorsally to insert onto the flexor tendon sheath and deep transverse metacarpal ligament.
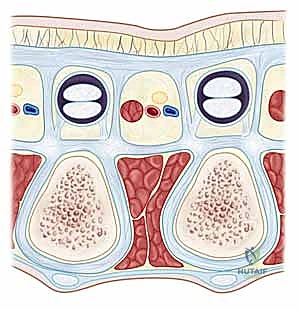
The transverse and vertical fibers of the central aponeurosis are equally critical. The transverse fibers form the natatory ligament (NL) in the distal palm, which creates the web spaces, and the transverse ligament of the palmar aponeurosis (TLPA) proximally. The vertical fibers include the strong vertical bands of Grapow and the septa of Legueu and Juvara. These eight septa form seven distinct fibro-osseous compartments: four flexor septal canals for the flexor tendons and three web space canals containing the common digital neurovascular bundles and lumbrical muscles.



The Pathological Cords
Understanding the specific cords is the key to safe fasciectomy.
* Pretendinous Cord: The most common cord, arising from the pretendinous band. It primarily causes MCP joint flexion deformity. Occasionally, it bifurcates, forming a "commissural Y cord" extending into adjacent digits.
* Central Cord: A direct distal extension of the pretendinous cord into the digit, attaching to the middle phalanx or flexor sheath.



- Spiral Cord: This is the most critical and dangerous cord for the surgeon. Most often seen in the small and ring fingers, it is a composite structure formed by the pathological amalgamation of four normal structures: the pretendinous band, the spiral band, the lateral digital sheet, and Grayson's ligament. Its biomechanical relationship with the neurovascular bundle (NVB) is paramount: as the spiral cord contracts, it displaces the NVB centrally, superficially, and proximally. The nerve spirals around the cord, placing it directly in the path of a standard surgical incision.
- Lateral Cord: Originates from the lateral digital sheet and attaches to Grayson's ligament, primarily causing PIP joint contracture.
- Natatory Cord: Converts the normal U-shaped web space into a restrictive V-shape.
- Abductor Digiti Minimi (ADM) Cord: Originates from the ADM tendon/fascia, coursing superficial to the ulnar NVB of the small finger, potentially displacing it medially, and causing severe PIP or DIP contracture.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention in Dupuytren's disease requires a nuanced assessment of functional impairment, disease progression, and patient expectations. The classic, universally taught threshold for surgical intervention is Hueston’s "tabletop test." If a patient is unable to place their hand completely flat on a hard surface, surgical evaluation is warranted. More specifically, quantitative indications include a metacarpophalangeal (MCP) joint flexion contracture exceeding 30 degrees, or any degree of proximal interphalangeal (PIP) joint flexion contracture. The lower threshold for PIP joint involvement is due to the notoriously recalcitrant nature of PIP contractures; the complex capsuloligamentous anatomy of the PIP joint rapidly undergoes secondary shortening, making complete surgical correction exceedingly difficult if intervention is delayed.
Furthermore, the velocity of disease progression is a critical factor. A rapidly evolving contracture, particularly in a younger patient exhibiting signs of Dupuytren's diathesis, necessitates earlier and potentially more aggressive intervention to prevent irreversible joint stiffness and severe functional decline. Pain is rarely a primary indication for fasciectomy, as DD is typically painless unless a rapidly growing nodule causes localized pressure or nerve compression. However, profound interference with activities of daily living—such as the inability to grasp large objects, put on gloves, or wash one's face without the contracted digit poking the eye—serves as a strong functional indication.
Contraindications must be carefully weighed. Absolute contraindications include active, uncontrolled local infection, severe medical comorbidities precluding safe anesthesia, and a lack of patient willingness or cognitive ability to participate in the rigorous, mandatory postoperative rehabilitation protocol. A history of severe Complex Regional Pain Syndrome (CRPS) in the ipsilateral extremity is a strong relative contraindication, as the surgical trauma of fasciectomy is a known potent trigger for CRPS flare-ups. In such cases, less invasive modalities, such as percutaneous needle aponeurotomy (PNA) or collagenase clostridium histolyticum (CCH) injections, might be considered, though open limited fasciectomy remains the gold standard for durable, long-term correction of severe, multi-digit disease.
| Category | Specific Criteria | Clinical Rationale |
|---|---|---|
| Primary Indications | MCP joint contracture > 30° | Restores functional grasp; MCP joints are highly amenable to surgical release. |
| Any degree of PIP joint contracture | PIP joints rapidly develop secondary capsular contractures; early release prevents permanent stiffness. | |
| Positive Hueston's Tabletop Test | Simple, reliable clinical indicator of functional impairment. | |
| Rapid disease progression | Prevents irreversible anatomical distortion, especially in patients with diathesis. | |
| Relative Contraindications | History of severe CRPS | High risk of triggering a debilitating postoperative pain syndrome. |
| Mild, non-progressive nodules | Surgery on isolated nodules without contracture carries risks without functional benefit. | |
| Absolute Contraindications | Inability to participate in rehab | Postoperative splinting and therapy are mandatory; failure guarantees recurrence/stiffness. |
| Active palmar infection | Risk of deep space hand infection and catastrophic tissue loss. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the absolute foundation of a successful Dupuytren's fasciectomy. The clinical examination must go beyond merely measuring joint angles with a goniometer. The surgeon must systematically palpate the entire palmar and digital surface to map the exact trajectory of the pathological cords. Skin involvement must be critically assessed; deep skin pitting, severe tethering, or blanching upon passive extension indicates that the dermis is intimately involved with the underlying cord. In these specific areas, standard flap elevation may result in full-thickness skin necrosis, necessitating the pre-operative consideration of a dermofasciectomy and subsequent full-thickness skin grafting (FTSG). A rigorous neurovascular examination, including static two-point discrimination and a modified Allen test, is mandatory to document any pre-existing deficits, which are not uncommon in chronic, severe contractures.

Incision planning is an art form in palmar reconstruction. The fundamental rule is to never cross a flexion crease perpendicularly, as this guarantees a secondary, iatrogenic scar contracture. The most widely utilized approaches are the Bruner zigzag incisions and longitudinal incisions incorporating multiple Z-plasties. The Bruner incision utilizes apices that meet at the flexion creases, allowing for excellent exposure of the flexor sheath and NVBs. Longitudinal incisions with planned Z-plasties are particularly useful when the skin is severely contracted, as the transposition of the Z-plasty flaps recruits transverse skin laxity to provide longitudinal lengthening, effectively addressing both the fascial and the cutaneous deficiency.


Patient positioning and operating room setup must be optimized for microsurgical precision. The patient is positioned supine with the operative extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. While some surgeons prefer exsanguination with an Esmarch bandage, others advocate for simple elevation prior to tourniquet inflation, allowing the veins to remain slightly engorged, which can aid in their identification and preservation during flap elevation. The surgeon must operate seated, utilizing high-quality surgical loupes (minimum 2.5x to 3.5x magnification) and a dedicated headlight. Essential instrumentation includes a lead hand or dynamic retractor system, fine-tipped tenotomy or Stevens scissors, delicate skin hooks (to minimize crush injury to the skin edges), and bipolar electrocautery for pinpoint hemostasis.


Step-by-Step Surgical Approach and Fasciectomy Technique
The execution of a limited fasciectomy requires a delicate balance between aggressive resection of pathological tissue and absolute preservation of the microvascular dermal plexus and digital neurovascular structures. The initial step involves the elevation of the planned skin flaps. These must be raised as full-thickness flaps, meticulously preserving the subdermal fat layer where the delicate microvascular plexus resides. Dissection should proceed with a scalpel or fine scissors, staying strictly superficial to the glistening, pathological Dupuytren's fascia. The use of skin hooks, rather than toothed forceps, is critical to prevent ischemic crush injury to the flap apices, which are highly susceptible to marginal necrosis.


Once the flaps are elevated and retracted, the most critical phase of the operation begins: the identification and protection of the Neurovascular Bundles (NVBs). The cardinal rule of Dupuytren's surgery is the "proximal-to-distal" approach. The surgeon must first identify the normal, un-involved common digital nerve and artery in the proximal palm, well proximal to the disease epicenter. Once identified, these structures are tagged with vessel loops and painstakingly traced distally into the pathological tissue. When a spiral cord is present, the surgeon must anticipate the nerve's abnormal anatomical displacement—superficial, central, and proximal. The cord must be carefully divided longitudinally or piecemeal to unroof and liberate the entrapped nerve before any en bloc resection is attempted.


Excision of the pathological tissue is then performed. In a standard limited fasciectomy, only the macroscopically diseased fascia is resected. The pretendinous cords are traced distally, releasing their insertions. If the PIP joint remains contracted after complete fascial excision, a stepwise joint release is indicated. This begins with an assessment of the flexor tendon sheath; occasionally, release of the A
Clinical & Radiographic Imaging Archive



