

Comprehensive Introduction and Patho-Epidemiology
Syndactyly represents the most ubiquitous congenital anomaly of the upper extremity, manifesting with an incidence of approximately 1 in 2,000 to 2,500 live births. While it may appear superficially as a mere cutaneous fusion, it represents a profound interruption in the highly orchestrated embryological cascade of upper limb development. The anomaly exhibits a slight male predilection and occurs bilaterally in approximately 50% of documented cases. The most frequently involved commissure is the third web space (between the long and ring fingers), followed by the fourth, second, and first web spaces.
To master the surgical reconstruction of the syndactylized web space, the orthopedic surgeon must first possess a granular understanding of the embryological blueprint. The upper extremity buds emerge from the lateral body wall mesoderm around the fourth week of gestation. By the fifth and sixth weeks, the terminal portion of the bud flattens to form the rudimentary hand plate. The critical phase of digital separation occurs between the sixth and eighth weeks. This separation is not a process of active outward growth of the digits, but rather a highly regulated, genetically programmed cell death—apoptosis—within the interdigital necrotic zones.
This apoptotic cascade is governed by a complex interplay of signaling molecules. The Apical Ectodermal Ridge (AER) acts as the primary signaling center for proximo-distal outgrowth, heavily reliant on Fibroblast Growth Factors (FGFs). Concurrently, the Zone of Polarizing Activity (ZPA), located at the posterior margin of the limb bud, secretes Sonic Hedgehog (SHH) protein, which dictates radio-ulnar (anterior-posterior) patterning. The actual interdigital apoptosis is primarily mediated by Bone Morphogenetic Proteins (specifically BMP-2, BMP-4, and BMP-7), which are modulated by the cessation of FGF signaling from the AER in the interdigital regions. Any genetic mutation, teratogenic exposure, or localized ischemia that disrupts this intricate molecular crosstalk results in a failure of separation, yielding syndactyly.

Classification of syndactyly is paramount for surgical planning and prognostic counseling. The nomenclature is defined by both the extent of the fusion and the nature of the conjoined tissues:
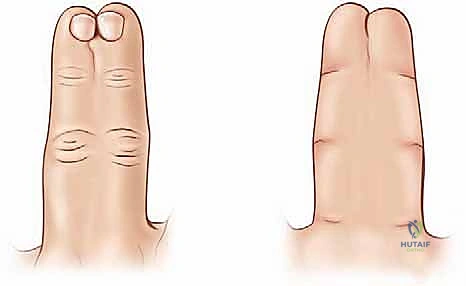
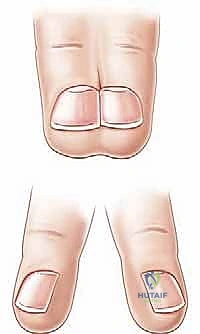
* Complete Syndactyly: The soft tissue union extends to the absolute distal tips of the involved digits, often involving the nail folds (synonychia).
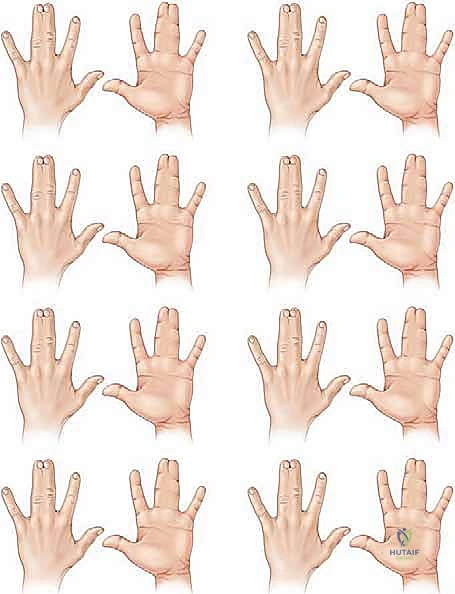
* Incomplete Syndactyly: The fusion terminates proximal to the distal interphalangeal joint or fingertips.
* Simple Syndactyly: The digits are tethered exclusively by skin, subcutaneous tissue, and occasionally fibrous fascial bands. No osseous fusion is present.
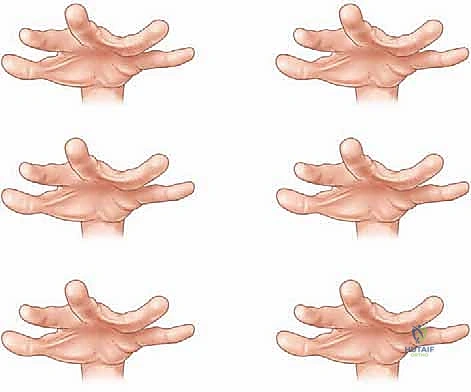
* Complex Syndactyly: Characterized by side-to-side osseous or cartilaginous fusion between adjacent phalanges.
* Complicated Syndactyly: Denotes a chaotic anatomical arrangement, frequently involving interposed accessory digits, hidden phalanges, delta bones, or severely intertwined neurovascular networks (often seen in Apert or Poland syndromes).
Detailed Surgical Anatomy and Biomechanics
The reconstructive goal in syndactyly release is not merely the separation of digits, but the architectural recreation of a functional, aesthetically normal web space. The normal human digital commissure is a biomechanical masterpiece, designed to permit independent digital flexion and wide abduction while maintaining palmar stability during power grip.
The Geometry of the Web Space
A normal web space is not a sharp cleft but a complex, sloping quadrilateral surface. The index-long and ring-small finger commissures are generally U-shaped, whereas the long-ring web is more V-shaped. The critical geometric feature is the dorsal-to-volar slope. The non-glabrous dorsal skin extends further distally than the glabrous palmar skin, creating a commissure that slopes at approximately a 45-degree angle from proximal-dorsal to distal-volar. This slope typically terminates near the mid-shaft of the proximal phalanx. Surgical reconstruction must meticulously replicate this 45-degree slope using robust dorsal skin flaps; failure to do so results in a web space that is too palmar, restricting abduction and predisposing the patient to web creep.
Neurovascular Topography and Anomalies
The vascular supply to the digits arises from the common digital arteries, which travel volar to the superficial transverse metacarpal ligament. In a normal hand, the common digital artery bifurcates into the proper digital arteries proximal to the web space. However, in syndactyly, the bifurcation of both the common digital arteries and the common digital nerves is frequently anomalous and located significantly distal to the intended new commissure.
During dissection, the surgeon must anticipate this distal bifurcation. If the neural bifurcation is distal, the common digital nerve can usually be safely split proximally through an epifascicular epineurotomy, teasing the fascicles apart under loupe or microscopic magnification without causing neuropraxia. Conversely, a distal arterial bifurcation presents a more formidable challenge. The artery cannot be split. If the bifurcation prevents the dorsal flap from seating deeply into the new web space, the surgeon must carefully assess the collateral circulation. While ligation of one proper digital artery is occasionally necessary to achieve a tension-free web, it is absolutely contraindicated if the opposite side of that digit has been, or will be, operated upon, as it risks catastrophic digital ischemia.
Fascial and Ligamentous Tethers
The natatory ligaments (superficial transverse metacarpal ligaments) are dense fascial bands that run transversely across the web spaces, supporting the palmar skin and contributing to the distal limit of the web. In syndactyly, these ligaments are often hypertrophied and form a rigid tether between the digits. Complete excision of the natatory ligament within the involved web space is a mandatory step to allow the reconstructed commissure to migrate proximally and sit without tension. Additionally, thickened bands of Cleland’s and Grayson’s ligaments may contribute to the syndactyly and require meticulous release.
The Biomechanics of Skin Deficits
A fundamental geometric principle dictates the necessity of skin grafting in simple complete syndactyly. The circumference of two separate cylinders (the separated digits) is approximately 22% greater than the circumference of a single cylinder encompassing both (the syndactylized digits). Therefore, separating the digits inevitably creates a substantial soft tissue deficit. While local flaps (dorsal and palmar) are utilized to reconstruct the deep commissure, attempting to close the lateral digital defects primarily will result in excessive tension, vascular compromise, and severe longitudinal scar contracture. Full-thickness skin grafts (FTSG) are the gold standard for resurfacing these inevitable lateral "bare areas."
Exhaustive Indications and Contraindications
The decision to operate, and specifically when to operate, requires a nuanced understanding of the natural history of the anomaly and the functional demands of the growing hand. Simple syndactyly does not spontaneously resolve. If left untreated, the tethering of adjacent digits—particularly those of disparate lengths—will inevitably lead to progressive flexion contractures, angular deformities (clinodactyly), and rotational malalignment.
Indications for Surgical Release
The primary indication for surgical release is the prevention of secondary growth deformities and the establishment of independent digital function.
* Differential Digital Length: Syndactylies involving the first web space (thumb-index) or the fourth web space (ring-small) must be released early (typically around 6 months of age). The significant difference in growth rates and ultimate lengths of these digits means that the longer digit will rapidly develop a severe, often irreversible, angular and flexion deformity if tethered to its shorter neighbor.
* Functional Independence: Complete syndactyly of any web space impairs fine motor dexterity, spanning grasp, and keyboard-oriented tasks. Release is indicated to maximize functional potential.
* Aesthetic and Psychosocial Considerations: The psychosocial impact of a visible congenital hand difference on a developing child is non-trivial. Reconstructing a natural-appearing hand before the child reaches school age minimizes negative peer interactions and fosters normal psychological development.
Contraindications to Surgical Release
While most simple syndactylies are amenable to surgical correction, certain complex scenarios warrant restraint.
* Mild Simple Incomplete Syndactyly: A very distal, subtle web that causes no functional impairment and minimal aesthetic concern may be managed non-operatively, provided the family is adequately counseled.
* The "Superdigit": In complex polysyndactyly, two digits may share a single tendinous or neurovascular apparatus. Attempting to separate these may result in two flail, insensate, or ischemic digits. In such cases, maintaining the syndactyly or performing a targeted ray resection is often functionally superior.
* Severe Medical Comorbidities: As this is an elective procedure, any severe cardiopulmonary or systemic anomaly that renders general anesthesia prohibitively dangerous is an absolute contraindication until the patient's medical status is optimized.
| Category | Clinical Scenario | Recommendation / Action |
|---|---|---|
| Absolute Indication | Border digit involvement (Thumb-Index, Ring-Small) | Early release (approx. 6 months) to prevent angular deformity. |
| Absolute Indication | Simple Complete Syndactyly (Long-Ring) | Release between 12-18 months for functional independence. |
| Relative Indication | Simple Incomplete Syndactyly (proximal to PIP) | Observation vs. elective release based on functional/aesthetic deficit. |
| Relative Contraindication | Complex Polysyndactyly ("Superdigit") | Avoid separation if it yields flail/insensate digits; consider ray amputation. |
| Absolute Contraindication | Severe unoptimized cardiopulmonary disease | Delay surgery until medically cleared for general anesthesia. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the bedrock of a successful syndactyly release. The surgical strategy must be formulated long before the initial incision is made.
Timing of the Intervention
The optimal timing for syndactyly release is a subject of ongoing academic discourse, balancing the anesthetic risks in infancy against the risk of progressive deformity.
* Early Release (6 months): Reserved for border digits (first and fourth web spaces) and complex syndactylies where tethering threatens immediate growth disturbances.
* Standard Release (12 to 18 months): The widely accepted window for simple complete syndactyly of the central digits (second and third web spaces). Operating at this age allows the anatomical structures to grow to a more manageable size for dissection, while still completing the reconstruction before the child develops complex prehensile patterns and body image awareness. Delaying past 18-24 months has been historically suggested to reduce the risk of "web creep," but modern flap designs have largely mitigated this concern, making earlier functional release preferable.
Imaging and Diagnostic Modalities
Standard posteroanterior (PA) and lateral plain radiographs of the affected hand are absolutely mandatory for every patient, regardless of how "simple" the syndactyly appears clinically. Radiographs are essential to definitively rule out complex syndactyly (hidden phalangeal fusions) or complicated syndactyly (interposed delta phalanges, bracket epiphyses).

Advanced imaging modalities, such as Magnetic Resonance Imaging (MRI) or MR Angiography, are rarely indicated for simple syndactyly. The neurovascular anomalies, while common, are managed intraoperatively through meticulous dissection rather than preoperative mapping. Such imaging requires sedation in pediatric patients and offers a low yield for altering the surgical plan in simple cases.
Patient Positioning and Preparation
The patient is positioned supine with the affected upper extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied high on the brachium. It is critical to place the tourniquet proximally enough to allow unhindered access to the antecubital fossa, should a full-thickness skin graft be required from that location.
If the inguinal fold is selected as the donor site for the full-thickness skin graft (which is highly preferred due to the abundance of tissue and concealable scar), the ipsilateral groin must be prepped and draped simultaneously.
* Surgical Pearl: Prior to draping, the surgeon should flex the patient's hip to accentuate the natural inguinal crease. The elliptical graft harvest site is marked precisely within this crease. Crucially, the harvest site must be positioned lateral to the femoral artery pulse. Harvesting medial to the artery risks transferring hormonally responsive, hair-bearing skin from the pubic region to the hand, a complication that is both cosmetically distressing and functionally problematic.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a simple syndactyly release is an exercise in geometric precision and atraumatic tissue handling. We will detail the release of a simple complete syndactyly utilizing the classic dorsal rectangular flap and lateral interdigitating zigzag incisions.
Flap Design and Incision Marking
Before tourniquet inflation, the incisions are marked with a fine surgical pen. The limb is exsanguinated with an Esmarch bandage, and the tourniquet is inflated to age- and weight-appropriate pressures (typically 150-200 mmHg in infants).
- The Dorsal Commissural Flap: This is the keystone of the reconstruction. A proximally based, rectangular or hourglass-shaped flap is drawn on the dorsum of the syndactylized web. The base of the flap corresponds to the metacarpal heads. The length of the flap is critical: it must extend distally to approximately two-thirds the length of the proximal phalanx. This length ensures that when the flap is inset volarly, it recreates the normal 45-degree dorsal-to-volar slope of the web space.
- The Volar Triangular Flaps: On the palmar aspect, one or two proximally based triangular flaps are designed. The apices of these triangles meet the distal margin of the planned dorsal flap. The base of the volar flap defines the new palmodigital crease.
- Lateral Interdigitating Flaps: From the distal margins of the dorsal and volar flaps, zigzag incisions are drawn along the lateral aspects of the conjoined digits. These incisions must cross the midline of the syndactyly at acute angles (typically 60 to 90 degrees). Straight longitudinal incisions are strictly forbidden, as they will inevitably lead to severe flexion contractures as the scar matures. The apices of the zigzag flaps on one digit must perfectly correspond to the recesses on the adjacent digit.
Dissection and Neurovascular Protection
Incisions are made sharply through the dermis using a #15 or #67 Beaver blade. Dissection proceeds under loupe magnification (3.5x to 4.5x). The dorsal and volar flaps are elevated. It is imperative to elevate these flaps with a thin layer of subcutaneous fat to preserve the subdermal vascular plexus, ensuring flap viability.

As the lateral flaps are elevated, the dissection deepens into the interdigital space. The thickened fascial bands of the interdigital septum and the natatory ligaments are identified and sharply excised. This release is what allows the digits to physically separate.
The critical phase of dissection is the identification of the neurovascular bundles. The common digital artery and nerve are located volar to the natatory ligament. Using blunt dissection with tenotomy scissors or fine hemostats, the bundles are traced distally.

If the bifurcation of the common digital nerve is distal to the planned commissure, an epifascicular epineurotomy is performed. Using micro-scissors, the epineurium is longitudinally incised, and the fascicles destined for the adjacent digits are gently separated proximally, allowing the nerve to drop deep into the hand. If the common digital artery bifurcates distally and tethers the web, the surgeon must evaluate the tension. If the dorsal flap cannot be seated without kinking the artery, one proper digital artery may need to be ligated, but only after confirming robust flow through the contralateral proper digital artery of that digit.

Flap Inset and Commissure Reconstruction
Once the digits are fully separated and the neurovascular bundles protected, the tourniquet is temporarily deflated to ensure hemostasis and confirm the viability of the digits and flaps. Meticulous bipolar electrocautery is used for hemostasis; tying off small vessels is avoided to minimize foreign body reaction.
The dorsal rectangular flap is then transposed through the newly created web space and sutured to the palmar triangular flaps. The flap must sit without tension. If the flap is too thick, it may be cautiously defatted, taking care not to violate the subdermal plexus. The flap is secured using fine absorbable sutures (e.g., 5-0 or 6-0 chromic gut). This maneuver establishes the critical dorsal-to-volar slope of the new commissure.


Full-Thickness Skin Grafting
Following the inset of the commissural and lateral zigzag flaps, substantial "bare areas" will remain on the lateral aspects of the digits, exposing the neurovascular bundles and flexor tendon sheaths. These defects must be resurfaced with full-thickness skin grafts (FTSG). Split-thickness grafts are contraindicated due to their high propensity for secondary contracture.
The previously marked elliptical graft is harvested from the inguinal crease. The donor site is closed primarily in layers, resulting in a highly aesthetic, concealed linear scar.
The harvested FTSG must be meticulously defatted. Using curved tenotomy scissors, all macroscopic subcutaneous fat is sharply excised until the stark white, glistening undersurface of the dermis is exposed. Any residual fat acts as a barrier to plasmatic imbibition and subsequent inosculation, leading to graft necrosis.

The defatted graft is templated to match the bare areas and sutured into place using 5-0 or 6-0 fast-absorbing plain gut or chromic sutures. Basting sutures may be placed centrally to ensure the graft is tightly apposed to the recipient bed, preventing hematoma accumulation.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following syndactyly release can occur. The surgeon must be adept at recognizing and managing these issues to salvage digital function and aesthetics.
Web Creep
Web creep is the most common long-term complication, occurring in up to 10-20% of cases depending on the series and the age at release. It is characterized by the distal migration of the commissure over time, resulting in a recurrent, albeit usually less severe, syndactyly. Web creep is multifactorial, driven by longitudinal scar contracture, inadequate initial dorsal flap length, or a growth mismatch between the scar tissue and the surrounding normal skin.
* Management: Mild web creep may be observed. Symptomatic or functionally limiting web creep requires secondary reconstruction, typically utilizing a combination of Z-plasties, local advancement flaps, or a redo of the dorsal flap with additional skin grafting.
Ischemia and Vascular Compromise
Digital ischemia is a rare but catastrophic complication. It is usually the result of excessive tension on the vascular pedicles, aggressive dissection, or the inadvertent ligation of a proper digital artery in a digit that lacks adequate collateral flow (e.g., if the other side of the digit was previously operated on).
* Management: Immediate recognition is critical. If a digit appears dusky or pale upon tourniquet deflation, the surgeon must first ensure the patient is normotensive and warm. Topical vasodilators (e.g., papaverine) can be applied to the vessels. If tension is the cause, sutures must be removed, and the flaps allowed to separate. In severe cases, vein grafting or microvascular repair may be necessary, though this is exceedingly difficult in infants.
Graft Failure and Infection
Partial or complete failure of the FTSG occurs in 2-5% of cases. It is most commonly caused by inadequate defatting of the graft, hematoma formation beneath the graft, or shear forces disrupting early inosculation. Superficial infections can also lead to graft loss.
* Management: Small areas of graft loss will heal by secondary intention, though they may leave a hypertrophic scar. Larger areas of necrosis require surgical debridement and application of a new skin graft once a healthy granulating bed is established.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Web Creep | 10% - 20% | Inadequate flap length, longitudinal scar contracture, early surgery. | Secondary Z-plasty, local advancement flaps, repeat FTSG. |
| Graft Failure | 2% - 5% | Inadequate defatting, hematoma, shear forces, infection. | Local wound care for small areas; debridement and re-grafting for large defects. |
| Scar Contracture | 5% - 10% | Straight longitudinal incisions, split-thickness grafts, poor compliance with OT. | Aggressive OT, silicone sheeting, surgical release with Z-plasty. |
| Digital Ischemia | < 1% | Vascular injury, excessive tension, bilateral simultaneous release. | Suture release, topical vasodilators, microvascular exploration. |
Phased Post-Operative Rehabilitation Protocols
The success of a syndactyly release is heavily dependent on the postoperative immobilization and subsequent rehabilitation. The delicate skin grafts and local flaps require absolute protection from shear forces during the initial healing phase.
Phase I: Immediate Post-Operative Immobilization (Weeks 0-3)
At the conclusion of the procedure, a highly specialized, non-adherent dressing is applied. Xeroform or a similar non-stick interface is placed directly over the grafts and incision lines. Moistened cotton balls or fluffs are meticulously packed into the interdigital spaces to act as a stent, applying gentle, even pressure to the FTSG to prevent hematoma and shear. A tie-over bolster dressing is often utilized to secure the graft in the concavity of the lateral digits.
The hand and forearm are then wrapped in a bulky, soft dressing. Finally, a well-molded, long-arm cast is applied. The elbow is immobilized at 90 degrees of flexion, and the cast extends proximal to the elbow. This long-arm configuration is absolutely essential in pediatric patients; a short-arm cast will inevitably slide off due to the child's tapered forearm anatomy, destroying the grafts in the process.
Phase II: Graft Assessment and Mobilization (Weeks 3-6)
The initial cast and dressings are removed in the clinic at approximately 3 to 4 weeks postoperatively. This is a critical juncture where the viability of the flaps and grafts is assessed. The grafts should appear
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding release-of-simple-syndactyly