Mastering the Lapidus Procedure: A Comprehensive Intraoperative Guide

Key Takeaway
This masterclass guides fellows through the Lapidus procedure for hallux valgus with first TMT hypermobility. We meticulously cover patient selection, detailed surgical anatomy, precise intraoperative steps including joint preparation and stabilization, and critical pearls to ensure successful arthrodesis. Emphasis is placed on neurovascular protection, accurate deformity correction, and comprehensive postoperative management, preparing you for complex forefoot reconstruction.
Welcome, colleagues and fellows, to the operating theater. Today, we are tackling a foundational procedure in advanced forefoot reconstruction: the Lapidus bunionectomy, more accurately defined as a first tarsometatarsal (TMT) arthrodesis. This operation transcends a simple bunion correction; it represents a fundamental, multi-planar realignment of the medial column. By addressing the root cause of many hallux valgus deformities—namely, the hypermobility, sagittal instability, and medial orientation of the first TMT joint—we restore the foundational biomechanics of the foot. Understanding this principle, initially conceptualized by Albrecht in 1911 and later popularized by Paul W. Lapidus in 1934, is paramount to achieving lasting correction, preventing recurrence, and yielding a pain-free, plantigrade foot.
In modern orthopedic surgery, our appreciation of hallux valgus has evolved from a simple two-dimensional transverse plane deformity to a complex triplanar anomaly. The Lapidus procedure remains the gold standard for addressing all three planes simultaneously: correcting the intermetatarsal angle (transverse plane), plantarflexing the first ray (sagittal plane), and derotating the pronated first metatarsal (frontal plane). This chapter provides an exhaustive, step-by-step masterclass on the pathoanatomy, preoperative planning, surgical execution, and postoperative management of the Lapidus procedure.
Comprehensive Introduction and Patho-Epidemiology
The Lapidus procedure is founded on the biomechanical premise that a significant subset of hallux valgus deformities is secondary to an underlying metatarsus primus varus, which intrinsically stems from instability or hypermobility at the first TMT joint. This instability manifests destructively across multiple planes. In the axial plane, it allows the first metatarsal to drift medially, increasing the intermetatarsal angle (IMA) and stripping the sesamoid apparatus of its mechanical advantage. In the sagittal plane, the first metatarsal elevates (dorsiflexes) under weight-bearing loads, transferring critical forces laterally and predisposing the patient to lesser metatarsalgia, stress fractures, and even dorsolateral peritalar subluxation over time.
Epidemiologically, hallux valgus affects nearly a third of the adult population, with a pronounced predilection for females. While distal and diaphyseal osteotomies are sufficient for mild to moderate deformities with a stable medial column, they fail to address the apex of the deformity in patients with TMT hypermobility. The failure to recognize and treat this proximal instability is a leading cause of hallux valgus recurrence. The Lapidus procedure directly neutralizes this hypermobility by fusing the medial cuneiform to the base of the first metatarsal, thereby locking the medial column into a mechanically advantageous, plantigrade position.
Our ultimate surgical goal is to restore a perfectly plantigrade foot, ensuring even weight distribution across the primary weight-bearing surfaces: the paired sesamoids, the lesser metatarsal heads, and the calcaneal tuberosity. The medial column is architecturally designed for rigidity, which is crucial for an efficient lever arm during the push-off phase of the gait cycle. Conversely, the lateral column provides the necessary mobility for accommodation to uneven terrain. By fusing the first TMT joint, we do not sacrifice essential foot mobility; rather, we restore the obligatory rigidity required for normal, pain-free ambulation.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel touches the skin, the operating surgeon must possess a meticulous, three-dimensional understanding of the surgical field. The anatomy of the first ray is unforgiving, and iatrogenic injury to its surrounding neurovascular structures can lead to devastating postoperative complications.
Osteology and Articular Geometry
The first TMT joint connects the base of the first metatarsal to the medial cuneiform. This joint is deceptively deep, often measuring 28 to 32 mm from dorsal to plantar, and its articular surfaces exhibit significant morphological variability. It is typically reniform (kidney-shaped), with a slight concavity on the metatarsal base and a corresponding convexity on the medial cuneiform. In patients requiring a Lapidus procedure, we frequently encounter an atavistic or medially oriented first TMT joint facet, which inherently drives the metatarsus primus varus. Understanding this angulation is critical; the surgeon must often resect an asymmetric wedge (wider laterally and plantarly) to achieve the desired multi-planar correction. Furthermore, the base of the second metatarsal articulates with the intermediate cuneiform and is recessed proximally compared to the first TMT joint. The dorsal aspect of the second metatarsal base serves as a critical anatomical landmark and target for our intermetatarsal stabilizing "home run" screw.
Neurovascular Networks
The dorsal approach to the first TMT joint places several critical neurovascular structures at risk. The deep peroneal nerve, a terminal branch of the common peroneal nerve, courses dorsally within the first intermetatarsal space. It supplies critical sensation to the first web space and provides motor innervation to the extensor digitorum brevis and the intrinsic muscles of the foot. It lies in perilous proximity to our deep dissection. The dorsalis pedis artery, the direct continuation of the anterior tibial artery, runs just lateral to the extensor hallucis longus (EHL) tendon, providing the primary arterial inflow to the dorsum of the forefoot. Its pulsations are routinely palpable preoperatively and should be protected meticulously. Additionally, the medial dorsal cutaneous nerve, a branch of the superficial peroneal nerve, supplies sensation to the dorsomedial aspect of the foot. Its branches are highly variable and are particularly vulnerable during the superficial exposure and when extending incisions distally toward the first metatarsophalangeal (MTP) joint.
Musculotendinous and Ligamentous Structures
Our primary dorsal approach exploits the internervous and intertendinous interval between the Extensor Hallucis Longus (EHL) and the Extensor Hallucis Brevis (EHB). The EHL is a prominent, easily identifiable landmark lying medial to the neurovascular bundle, while the EHB sits laterally. Utilizing this precise interval allows for robust access to the joint capsule while minimizing muscular disruption. Deep to the intermetatarsal ligament lie the fibular sesamoid and the adductor hallucis tendon. During any concomitant modified McBride procedure or lateral soft tissue release, it is imperative to protect the plantar structures. Plantarly, the peroneus longus tendon inserts onto the lateral base of the first metatarsal and medial cuneiform. This tendon acts as a primary plantarflexor of the first ray; preserving its insertion is vital for maintaining the postoperative windlass mechanism and dynamic medial arch stability.
Exhaustive Indications and Contraindications
Patient selection is the absolute cornerstone of a successful Lapidus arthrodesis. The procedure is technically demanding and carries a longer recovery period than distal osteotomies; therefore, it must be reserved for patients exhibiting specific pathoanatomical criteria. The primary indication is a symptomatic hallux valgus deformity accompanied by documented first TMT hypermobility. This hypermobility is assessed clinically by stabilizing the lesser metatarsals and moving the first ray dorsally and plantarly; excessive, unresisted dorsal excursion indicates incompetence of the plantar fascial and ligamentous restraints.
Additionally, the Lapidus procedure is the treatment of choice for patients presenting with first TMT arthrosis in conjunction with hallux valgus. Fusing an already degenerative joint eliminates pain while simultaneously correcting the deformity. It is also highly indicated for patients with severe sagittal plane instability—evidenced by a dorsiflexed first metatarsal and secondary lesser metatarsalgia (transfer lesions)—as well as for revision scenarios where a previous distal hallux valgus surgery failed due to an unaddressed hypermobile medial column. Severe deformities with an intermetatarsal angle exceeding 15 to 20 degrees, particularly in younger, active patients, are also best managed with a proximal fusion to ensure a powerful, durable lever arm.
Conversely, absolute contraindications must be strictly respected. Open physeal growth plates preclude the use of a Lapidus, as arthrodesis of a growth plate-containing joint will lead to severe growth arrest and secondary deformities. Active localized or systemic infection, severe peripheral vascular disease, and non-ambulatory status are universally accepted contraindications. Furthermore, significant bone loss, severe osteopenia, or Charcot neuroarthropathy (without specialized rigid fixation techniques) represent relative to absolute contraindications, as the risk of nonunion or hardware failure becomes unacceptably high.
| Category | Specific Conditions |
|---|---|
| Primary Indications | Symptomatic hallux valgus with first TMT hypermobility; Severe hallux valgus (IMA > 15°); First TMT osteoarthritis with deformity; Revision hallux valgus surgery. |
| Secondary Indications | Sagittal plane instability (elevated first ray) with transfer metatarsalgia; Connective tissue disorders (e.g., Ehlers-Danlos, Marfan syndrome) causing ligamentous laxity. |
| Absolute Contraindications | Open physeal growth plates; Active pedal or systemic infection; Severe peripheral arterial disease (inadequate perfusion for bone healing). |
| Relative Contraindications | Active smoking (high nonunion risk); Severe osteoporosis/osteopenia; Non-ambulatory patients; Uncontrolled diabetes mellitus (HbA1c > 8.0%). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning separates the master surgeon from the technician. The success of the Lapidus procedure is largely dictated before the first incision is made, relying heavily on rigorous radiographic analysis and clinical examination.
Radiographic Assessment and Templating
Our evaluation begins with standardized, weight-bearing radiographs of the foot, including anteroposterior (AP), lateral, and oblique projections. On the AP view, we meticulously quantify the hallux valgus angle (HVA, normal < 15 degrees) and the intermetatarsal angle (IMA, normal < 9 degrees). We critically evaluate the morphology of the first TMT joint, noting any atavistic (medial) angulation that will dictate the geometry of our bony resection. The position of the sesamoids is graded; lateral subluxation indicates the need for a thorough lateral soft tissue release at the MTP joint. On the lateral weight-bearing view, we assess the talar-first metatarsal angle (Meary's angle) to identify sagittal plane collapse and evaluate the first metatarsal for elevation (dorsiflexion). An axial sesamoid view is imperative to assess metatarsosesamoid arthrosis, which, if severe, may necessitate a concurrent first MTP arthrodesis rather than a joint-sparing Lapidus.
Clinical Evaluation
Beyond imaging, a comprehensive physical examination is non-negotiable. The first TMT hypermobility test is performed to confirm proximal instability. We must also perform the Silfverskiöld test to differentiate between gastrocnemius tightness and a combined Achilles contracture. A tight gastrocnemius-soleus complex exerts a massive plantarflexion force on the calcaneus, which secondarily unlocks the midfoot and exacerbates medial column collapse. If a severe equinus contracture is identified, a concurrent gastrocnemius recession or percutaneous Achilles tendon lengthening is mandatory to prevent catastrophic overload of the TMT arthrodesis site. Finally, the plantar aspect of the foot is inspected for intractable plantar keratoses (IPKs) beneath the lesser metatarsal heads, confirming transfer metatarsalgia.
Patient Positioning and Operating Room Setup
The patient is positioned supine on a radiolucent operating table. A padded bump is placed under the ipsilateral hip to internally rotate the leg, neutralizing the natural external rotation of the lower extremity and bringing the foot into a true AP position. This seemingly minor step is critical for accurate intraoperative fluoroscopic assessment. A sterile pneumatic tourniquet is applied to the thigh or calf, depending on surgeon preference and the potential need for proximal bone graft harvesting. Once the limb is prepped and draped, a small towel bump is placed beneath the knee to slightly flex the joint, relaxing the posterior neurovascular structures and allowing the foot to rest perfectly flat on the table. The C-arm fluoroscopy unit is brought in from the contralateral side, positioned to allow seamless, immediate AP, lateral, and oblique views without requiring awkward repositioning of the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
We have completed our definitive time-out, confirmed the patient, the operative site, and the procedure. The surgical field is optimally exposed, and we are ready to commence the reconstruction.
Incision and Superficial Dissection
We begin with the primary dorsal approach to the first TMT joint. Using a surgical marker, we outline an incision approximately 6 to 8 cm in length, centered directly over the first TMT joint. This incision runs parallel to the lateral border of the first metatarsal and the medial cuneiform, precisely targeting the internervous interval between the EHL and the EHB.

TECH FIG 1A: Preoperative planning and marking of the dorsal incision over the first TMT joint, centered between the EHL and EHB tendons.
Using a #15 blade, the skin and superficial fascia are incised.

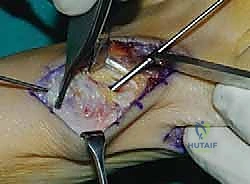
TECH FIG 1B: Superficial dissection utilizing the interval between the extensor hallucis longus (medial) and extensor hallucis brevis (lateral).
Subcutaneous dissection is performed bluntly using a Freer elevator or Metzenbaum scissors. The surgeon must remain acutely vigilant regarding the deep peroneal nerve and the dorsalis pedis artery, which course just lateral to the EHL tendon. These structures are mobilized as a single bundle and gently retracted laterally using Senn or Ragnell retractors. Hemostasis is maintained meticulously with bipolar electrocautery to prevent postoperative hematoma formation, which can compromise wound healing.
Deep Dissection and Tarsometatarsal Joint Exposure
Once the interval is established, the dorsal capsule of the first TMT joint is identified. The joint line is palpated and confirmed by gently manipulating the first metatarsal in the sagittal plane. A longitudinal capsulotomy is performed sharply with a #15 blade. We utilize a "Henry angle" of subperiosteal dissection, elevating the capsule medially and laterally to fully expose the articular surfaces. Often, a prominent dorsal osteophyte is present at the TMT joint; this is excised using a sharp 1/4-inch osteotome. Clinical Pearl: Retain these healthy, cancellous osteophytes on the back table; they serve as excellent autologous bone graft to pack into the arthrodesis site later, negating the need for allograft.
Joint Preparation and Arthrodesis Site Management
Thorough joint preparation is the most critical step in preventing nonunion. The goal is to remove all articular cartilage down to healthy, bleeding subchondral bone while carefully preserving the native architecture and length of the first ray.
If the joint does not exhibit severe medial angulation and the metatarsal length is a concern, joint preparation is performed using hand instruments.
TECH FIG 1C: Joint preparation utilizing a curette to meticulously remove articular cartilage while preserving subchondral bone contour.

TECH FIG 2A: Deep curettage of the first TMT joint. Note the depth of the joint; the plantar flare must be adequately debrided to prevent dorsal malunion.
We utilize curved osteotomes, ring curettes, and a high-speed burr to meticulously denude the cartilage. The first TMT joint is nearly 3 cm deep; failure to adequately prepare the plantar-most aspect is a classic pitfall that leads to a dorsal opening wedge upon compression, resulting in a disastrous dorsiflexion malunion. Once denuded, the subchondral bone is aggressively fenestrated using a 2.0-mm drill bit or a K-wire to stimulate marrow bleeding and osteoprogenitor cell migration.
Conversely, if a significant angular deformity exists (a severely medially angled cuneiform facet), planar resection using an oscillating saw is required.

TECH FIG 2B: Utilizing an oscillating saw for planar resection. This technique allows for the removal of a biplanar wedge (plantar and lateral base) to correct severe deformities.
The saw blade is directed to resect a wedge of bone that is wider laterally (to close the IMA) and wider plantarly (to plantarflex the first ray). Extreme care must be taken to avoid over-shortening the metatarsal, which can induce severe transfer metatarsalgia.
Deformity Reduction and Provisional Fixation
With the joint prepared, we execute the triplanar reduction. The first metatarsal is grasped with a sturdy bone clamp. The reduction maneuver consists of three simultaneous actions: 1) Lateral translation and angulation to close the intermetatarsal angle; 2) Plantarflexion to restore the sagittal arch and load the medial column; and 3) Supination (derotation) of the metatarsal to correct the frontal plane pronation intrinsic to hallux valgus.
Once reduced, the joint is provisionally stabilized with two 2.0-mm Kirschner wires. Fluoroscopy is brought in to confirm the reduction on AP, lateral, and oblique views. The IMA should be reduced to less than 9 degrees, the sesamoids should be anatomically located beneath the metatarsal head, and the lateral view should demonstrate a perfectly colinear Meary's line without dorsal elevation of the first ray.
Definitive Hardware Fixation
Rigid internal fixation is mandatory. While modern plating systems are popular, the classic crossed-screw technique remains a biomechanically robust and cost-effective gold standard.

TECH FIG 3A: Application of a pointed reduction clamp to achieve robust compression across the arthrodesis site prior to screw placement.
A large pointed reduction clamp is applied across the joint to generate maximal compression. The first screw—the "home run" screw—is typically a 4.0-mm or 4.5-mm fully threaded, solid or cannulated cortical screw. It is directed from the dorsal-distal aspect of the first metatarsal base, aiming proximal and plantar into the dense bone of the medial cuneiform.
TECH FIG 3B: Insertion of the primary compression screw across the TMT joint.
A second screw is placed to control rotation. This can be directed from the dorsal-proximal medial cuneiform into the plantar-distal first metatarsal, or, alternatively, as an intercuneiform/intermetatarsal screw from the first metatarsal base into the base of the second metatarsal.

TECH FIG 3C: Final seating of the crossed-screw construct, ensuring screw heads are countersunk to prevent hardware prominence.
If the bone quality is poor or the deformity is massive, a dorsal or medial neutralization plate is applied over the joint to augment the screw construct and provide rigid stabilization against plantar gapping.
Distal Soft Tissue Procedure and Closure
Following rigid fixation of the TMT joint, attention is turned to the first MTP joint. If residual hallux valgus or sesamoid subluxation remains, a distal soft tissue release (modified McBride) is performed through a separate dorsal first web space incision. The adductor hallucis tendon is released from the base of the proximal phalanx and the fibular sesamoid, and the deep transverse metatarsal ligament is transected. A medial capsulorrhaphy is then performed to realign the hallux.

TECH FIG 4: Final intraoperative fluoroscopy confirming anatomic alignment, closure of the IMA, and appropriate hardware placement without intra-articular joint penetration.
The wounds are thoroughly irrigated with sterile saline. The extensor retinaculum and subcutaneous tissues are closed meticulously with 3-0 absorbable sutures, ensuring the superficial nerves are not entrapped. The skin is closed with a running 4-0 non-absorbable subcuticular stitch or nylon sutures. A sterile, bulky, compressive dressing is applied, and the foot is placed in a well-padded short leg splint in neutral dorsiflexion.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, the Lapidus procedure carries a distinct complication profile. The most feared complication is nonunion (pseudoarthrosis) of the first TMT joint. Historically reported at rates up to 10-12%, modern rigid fixation techniques and joint preparation methods have driven the nonunion rate down to approximately 3-5%. Patient factors such as smoking, diabetes, and non-compliance with non-weight-bearing protocols drastically increase this risk. Symptomatic nonunions require revision surgery with aggressive debridement, structural autogenous bone grafting (e.g., iliac crest), and robust plate fixation.
Malunion is another critical complication, with dorsal elevation (dorsiflexion malunion) being the most common and devastating. This occurs due to inadequate plantar joint preparation or premature weight-bearing, leading to plantar gapping. A dorsiflexed first ray strips the medial column of its weight-bearing capacity, resulting in severe, recalcitrant transfer metatarsalgia beneath the second and third metatarsal heads. Salvage requires a corrective plantarflexion opening wedge osteotomy of the medial cuneiform or first metatarsal base.
Hardware prominence is common, particularly with dorsal plates or poorly countersunk screws, leading to shoe wear irritation. This is easily managed with symptomatic hardware removal after radiographic union is confirmed (typically after 6 months). Iatrogenic nerve injury, particularly to the medial dorsal cutaneous nerve or deep peroneal nerve, can result in painful neuromas or localized numbness. Careful soft tissue handling and retraction are the only preventative measures.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Nonunion | 3% - 5% | Smoking, inadequate joint prep, poor fixation, premature weight-bearing. | Revision arthrodesis, iliac crest bone graft, rigid locking plate fixation. |
| Dorsiflexion Malunion | 2% - 4% | Inadequate plantar resection, plantar gapping during screw compression. | Plantarflexing opening wedge osteotomy (proximal metatarsal or cuneiform). |
| Hardware Prominence | 10% - 15% | Thin dorsal soft tissue envelope, prominent screw heads or bulky plates. | Hardware removal after definitive radiographic union (minimum 6 months). |
| Nerve Injury / Neuroma | 1% - 3% | Aggressive retraction, entrapment in closure (deep peroneal or superficial branches). | Gabapentinoids, targeted steroid injections, surgical neuroma excision/burial. |
Phased Post-Operative Rehabilitation Protocols
The rehabilitation following a Lapidus procedure is protracted compared to distal osteotomies, demanding high patient compliance. A phased, biologically respectful approach is mandatory to ensure bony union while preventing stiffness.
Phase I: Immediate Post-Operative (Weeks 0-2)
The primary goals during this phase are wound healing, edema control, and pain management. The patient is placed in a rigid posterior splint and is strictly non-weight-bearing on the operative extremity. Elevation above the level of the heart is emphasized to minimize swelling. At two weeks, the patient returns to the clinic for splint removal, wound inspection, and suture removal. If the incisions are fully healed, the patient is transitioned into a removable controlled ankle motion (CAM) boot.
Phase II: Protected Weight-Bearing (Weeks 2-6)
During weeks two through six, the patient remains in the CAM boot. Depending on the surgeon's preference, bone quality, and the rigidity of the fixation construct, the patient may remain strictly non-weight-bearing or begin progressive heel-touch weight-bearing. Active and passive range of motion exercises of the first MTP joint are initiated immediately to prevent capsular contracture and arthrofibrosis, which are common secondary complications of prolonged immobilization.
Phase III: Progressive Loading and Strengthening (Weeks 6-12)
At the six-week mark, weight-bearing radiographs are obtained. If there is evidence of bridging trabecular bone across the arthrodesis site, the patient is cleared to begin progressive full weight-bearing within the CAM boot. Physical therapy is formally initiated, focusing on intrinsic foot muscle strengthening, restoration of the normal heel-to-toe gait mechanics, and aggressive first MTP joint mobilization. By weeks 8 to 10, patients are typically transitioned into a supportive, stiff-soled athletic shoe with a wide toe box. High-impact activities and sports are generally restricted until 4 to 6 months postoperatively, pending complete radiographic consolidation and functional recovery.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the Lapidus procedure is deeply rooted in robust orthopedic literature. Paul W. Lapidus’s original 1934 manuscript in Surgery, Gynecology & Obstetrics remains the foundational text, establishing the concept that proximal hypermobility dictates distal deformity. In the modern era, Myerson et al. (1992) revolutionized the procedure by demonstrating that rigid crossed-screw fixation significantly reduced the unacceptably high nonunion rates associated with earlier casting techniques.
More recently, the biomechanical studies by Coetzee and colleagues have underscored the critical importance of plantarflexing the first ray to restore the windlass mechanism and prevent transfer metatarsalgia. Furthermore, the paradigm-shifting work by Dayton et al. has brought the triplanar nature of hallux valgus to the forefront. Their research definitively proves that the first metatarsal is not only deviated medially but is also inherently pronated (rotated) in the frontal plane. Consequently, modern clinical guidelines now dictate that a successful Lapidus procedure must incorporate a derotational maneuver prior to fixation to achieve true anatomical restoration of the sesamoid complex. Mastery of this triplanar correction distinguishes the contemporary orthopedic surgeon and ensures the highest level of functional outcomes for our patients.
