Mastering Metacarpophalangeal & Proximal Interphalangeal Joint Contracture Release

Key Takeaway
This masterclass provides an exhaustive, real-time guide to releasing metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joint contractures. Fellows will learn intricate surgical anatomy, meticulous dissection techniques, and critical decision-making for restoring motion. We cover preoperative planning, precise intraoperative execution, managing complications, and essential postoperative rehabilitation protocols, ensuring a comprehensive understanding of this challenging hand surgery.
Comprehensive Introduction and Patho-Epidemiology
The Genesis of Digital Stiffness
Welcome, colleagues, to a definitive exploration of one of the most challenging yet profoundly rewarding domains in hand surgery: the operative release of post-traumatic metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joint contractures. The stiff digit represents a formidable reconstructive challenge, as it fundamentally disrupts the intricate kinematic chain required for prehension, grasp, and fine motor dexterity. This pathology is rarely a simple matter of isolated tissue shortening; rather, it is the culmination of a complex interplay between altered anatomy, disrupted biomechanics, and a relentless fibrotic cascade. Our objective as reconstructive surgeons is not merely the mechanical division of scar tissue, but the meticulous restoration of gliding planes and joint kinematics, thereby returning functional autonomy to our patients.
Post-traumatic contractures typically emerge from two primary pathways: direct articular or periarticular trauma, and indirect consequences of the injury, such as prolonged immobilization, unchecked edema, or sub-optimal splinting paradigms. Intra-articular fractures, severe crush injuries, and extensive soft tissue avulsions directly incite a profound inflammatory response within the joint capsule. Conversely, remote trauma to the hand or upper extremity frequently results in ubiquitous dependent edema. This fluid invariably gravitates toward the MCP and PIP joints due to the relatively compliant nature of their capsular structures, setting the stage for insidious stiffening if not aggressively managed in the acute phase.
The hydraulic pressure generated by joint effusions and hemarthrosis plays a pivotal role in the predictable posturing of the traumatized hand. The MCP joint capsule, when distended by fluid, exerts a hydraulic force that invariably drives the joint into a position of near-maximal extension. This extended posture maximizes capsular volume, thereby minimizing intra-articular pressure and providing the patient with transient pain relief. However, if this position is maintained through prolonged immobilization or patient guarding, the collateral ligaments are permitted to shorten in a lax state, initiating the irreversible structural changes that define an established contracture.
Pathophysiology of Fibroplasia and Contracture
Over time, the initial fluid accumulation and acute inflammatory response transition into a chronic fibrotic state. This fibroplasia is characterized by the proliferation of myofibroblasts and the disorganized deposition of type I and type III collagen. The dorsal capsule of the MCP joint thickens significantly, losing its essential compliance and effectively tethering the joint in extension. Concurrently, the underlying proper collateral ligaments undergo structural shortening and scar densely to the lateral aspects of the metacarpal head, obliterating the normal gliding recesses.
This fibrotic onslaught extends beyond the immediate capsuloligamentous structures. The overlying extensor mechanism, encompassing the extensor digitorum communis (EDC) tendon and its stabilizing sagittal bands, frequently becomes densely adherent to the fibrotic dorsal capsule. This creates a functional tenodesis, further restricting flexion. In the volar aspect of the joint, the volar recess—normally a capacious potential space—can become completely obliterated by unyielding adhesions forming between the volar plate and the metacarpal condyles. Similar pathologic cascades occur at the PIP joint, though the anatomical nuances of the PIP joint typically predispose it to profound flexion contractures rather than extension contractures.
Furthermore, the intrinsic musculature, particularly the interossei and lumbricals, frequently succumb to contracture or ischemic fibrosis following trauma or compartment syndrome. This contributes significantly to the classic "intrinsic-plus" or "intrinsic-minus" deformities, which further complicate the clinical picture. Finally, we must never underestimate the restricting role of scarred skin and subcutaneous tissue, particularly in the wake of thermal burns or severe degloving injuries. The skin envelope must possess sufficient elasticity to accommodate the full excursion of the underlying joints; without it, even the most perfect capsular release will fail to restore motion.
Epidemiological Considerations in Hand Trauma
The epidemiology of joint contractures in the hand is inextricably linked to the incidence of industrial accidents, motor vehicle collisions, and sports-related trauma. Crush injuries, which impart massive energy to both the skeletal architecture and the soft tissue envelope, carry an exceptionally high risk of subsequent stiffness. The incidence of contracture is also directly correlated with the duration of immobilization. The historical paradigm of prolonged casting for hand fractures has largely been supplanted by principles of stable internal fixation and early active mobilization, precisely to mitigate this devastating complication.
Despite advances in hand therapy and surgical techniques, certain patient populations remain at elevated risk. Individuals with a propensity for hypertrophic scarring, those with underlying systemic inflammatory conditions (such as rheumatoid arthritis, though the pathology differs from post-traumatic stiffness), and patients who are non-compliant with rigorous postoperative rehabilitation protocols frequently experience suboptimal outcomes. The psychological burden of a stiff, non-functional hand is immense, often leading to prolonged occupational disability and significantly diminished quality of life, underscoring the critical importance of mastering these reconstructive techniques.
Detailed Surgical Anatomy and Biomechanics
Metacarpophalangeal Joint Osteology and Kinematics
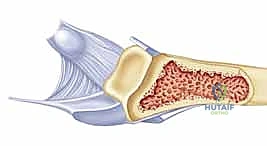
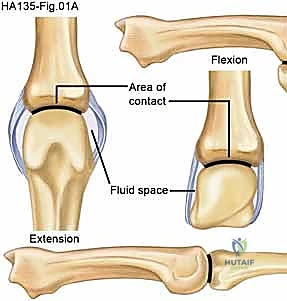
To successfully release a contracted joint, the surgeon must possess an encyclopedic understanding of its underlying anatomy and biomechanical behavior. The MCP joint is a diarthrodial condyloid joint, engineered to permit a biaxial arc of motion that includes flexion, extension, abduction, adduction, and circumduction. The cornerstone of this joint's unique biomechanics is the asymmetrical, cam-shaped morphology of the metacarpal head. While it presents a relatively flat mediolateral convex arc to facilitate abduction and adduction, its anteroposterior profile is profoundly convex, extending significantly further volarly than dorsally.
This volar protrusion of the metacarpal head is the anatomical basis for the "cam effect." As the proximal phalanx flexes around the metacarpal head, the distance between the origin of the collateral ligaments (on the dorsal metacarpal tubercle) and their insertion (on the volar base of the proximal phalanx) increases. Consequently, the proper collateral ligaments become maximally taut in full flexion, providing crucial lateral stability during grasp. Conversely, in full extension, these ligaments are lax, allowing for maximal capsular volume and lateral mobility. This biomechanical reality dictates the fundamental rule of hand splinting: the MCP joints must be immobilized in 70 to 90 degrees of flexion to maintain collateral ligament length and prevent extension contractures.
The base of the proximal phalanx presents a shallow, concave articular surface that articulates with the metacarpal head. The inherent lack of deep bony constraint in the MCP joint means that its stability is almost entirely dependent on the integrity of its surrounding soft tissue envelope. This reliance on soft tissues makes the joint highly susceptible to contracture when these structures become fibrotic, but it also renders the joint amenable to surgical release, provided the surgeon can accurately identify and systematically divide the offending tethers without destabilizing the joint.
Proximal Interphalangeal Joint Architecture
In stark contrast to the multiaxial MCP joint, the PIP joint is a highly constrained, true bicondylar hinge joint. Its osteology permits motion almost exclusively in the flexion-extension plane. The head of the proximal phalanx features two distinct condyles separated by an intercondylar groove, which articulate precisely with the corresponding concave facets and median ridge of the middle phalanx base. This interlocking bony architecture provides substantial inherent stability but leaves little room for error; any subtle articular incongruity following trauma rapidly leads to altered kinematics, cartilage wear, and debilitating stiffness.

The ligamentous stabilization of the PIP joint is frequently described as a robust, box-like configuration. The proper collateral ligaments originate from the condylar recesses of the proximal phalanx and insert onto the volar-lateral aspect of the middle phalanx base. Unlike the MCP joint, the collateral ligaments of the PIP joint remain relatively isometric throughout the arc of motion, though specific fiber bundles experience varying degrees of tension. The accessory collateral ligaments fan out volarly to insert into the margins of the volar plate, effectively suspending it beneath the joint.

The volar plate of the PIP joint is a remarkably thick, rigid, fibrocartilaginous structure designed to resist hyperextension forces. It is loosely attached proximally to the neck of the proximal phalanx by two distinct fibrous bands known as the check-rein ligaments. Watson and colleagues definitively identified these check-rein ligaments as the primary culprits in the pathogenesis of PIP joint flexion contractures. Following trauma and prolonged flexion, these ligaments undergo dense fibroplasia, effectively tethering the volar plate proximally and preventing the middle phalanx from gliding into extension.
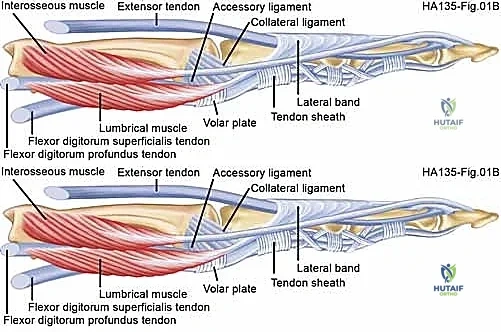
The Extensor and Flexor Mechanisms
The capsuloligamentous structures do not exist in isolation; they are intimately enveloped by the dynamic extensor and flexor mechanisms, which frequently become ensnared in the fibrotic process. Dorsally at the MCP level, the EDC tendon is stabilized by the sagittal bands, which originate from the volar plate and intermetacarpal ligaments, wrapping dorsally to centralize the tendon over the metacarpal head. In an extension contracture, these sagittal bands often become densely adherent to the underlying capsule and collateral ligaments, requiring meticulous elevation or fractional lengthening during release.

Further distally, the extensor mechanism transitions into a complex aponeurotic expansion over the proximal phalanx. The central slip inserts onto the dorsal base of the middle phalanx, responsible for PIP extension, while the lateral bands bypass the PIP joint to converge and insert on the distal phalanx. Adhesions of the central slip or lateral bands to the underlying proximal phalanx or PIP joint capsule will severely restrict digital flexion, necessitating concurrent tenolysis during capsulotomy.

Volarly, the flexor tendons (flexor digitorum superficialis and profundus) glide within a highly specialized fibro-osseous sheath. The sheath is intimately associated with the volar plates of both the MCP and PIP joints. In cases of severe crush injuries or volar lacerations, the flexor tendons can scar densely to the sheath or the volar plate itself. A PIP flexion contracture cannot be successfully resolved if the flexor tendons remain tethered proximally; therefore, the surgeon must always be prepared to perform a flexor tenolysis in conjunction with a volar capsulotomy.
Neurovascular Topography
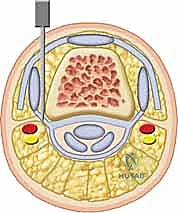
Surgical approaches to the MCP and PIP joints must be executed with a profound respect for the regional neurovascular anatomy. Dorsally, the skin overlying the MCP joints is innervated by terminal sensory branches of the radial nerve (for the radial digits) and the dorsal sensory branch of the ulnar nerve (for the ulnar digits). These delicate nerves course longitudinally in the subcutaneous tissue and are highly vulnerable to transection or traction injury during dorsal longitudinal incisions or flap elevation. Injury to these structures can result in persistent numbness or, more devastatingly, the formation of exquisitely painful neuromas that can eclipse the benefits of the joint release.

Volarly and laterally, the proper digital nerves and arteries course along the midaxial lines of the digits, slightly volar to the axis of rotation of the interphalangeal joints. When utilizing midaxial or volar Bruner incisions to access the PIP joint for volar plate release or flexor tenolysis, these neurovascular bundles must be meticulously identified, mobilized, and protected with vessel loops. In digits with longstanding, severe flexion contractures, the neurovascular bundles may have shortened. Aggressive, acute intraoperative extension of the joint following release can precipitate arterial spasm or intimal traction injury, leading to digital ischemia—a catastrophic complication that must be avoided at all costs.
Exhaustive Indications and Contraindications
Clinical Evaluation and Decision Making
The decision to proceed with the operative release of a contracted digital joint is never taken lightly. It requires a comprehensive clinical evaluation to ascertain the precise anatomical structures restricting motion and to evaluate the patient's overall suitability for a demanding surgical and rehabilitative process. The history must detail the mechanism of the original injury, the duration of the contracture, and the specific conservative modalities (dynamic splinting, static progressive splinting, targeted hand therapy) that have been exhausted. A contracture that has been present for less than six months may still respond to aggressive, specialized therapy, whereas a rigid, unyielding contracture present for over a year is highly unlikely to improve without surgical intervention.

Physical examination is paramount. The surgeon must differentiate between joint-based stiffness (capsular or ligamentous contracture) and extra-articular stiffness (tendon adhesions, intrinsic muscle contracture, or skin shortage). This is accomplished through careful passive range of motion testing while manipulating adjacent joints. For example, if PIP joint flexion improves significantly when the MCP joint is held in extension, the primary pathology likely involves intrinsic muscle tightness (a positive intrinsic tightness test) rather than an isolated PIP capsular contracture. The quality of the soft tissue envelope must be critically assessed; heavily scarred, avascular, or tightly adherent skin will compromise the surgical approach and limit postoperative excursion.

Furthermore, the surgeon must evaluate the specific digital deformities present. A Boutonnière deformity, characterized by PIP flexion and distal interphalangeal (DIP) hyperextension, indicates disruption or attenuation of the central slip with volar subluxation of the lateral bands. A Swan-neck deformity, featuring PIP hyperextension and DIP flexion, suggests volar plate laxity at the PIP joint and terminal tendon disruption or imbalance. These complex multi-joint imbalances require highly specific reconstructive strategies that go far beyond a simple capsular release.
Defining Surgical Candidacy
The success of a joint release is heavily dependent on patient selection. The ideal candidate possesses a stable, congruent joint surface, a supple soft tissue envelope, intact and functional flexor and extensor musculotendinous units, and, most importantly, the psychological resilience and dedication required to endure months of rigorous postoperative therapy.
| Category | Indications | Contraindications (Absolute & Relative) |
|---|---|---|
| Clinical Status | Rigid contracture failing >3-6 months of dedicated, specialized hand therapy. | Absolute: Active, untreated local or systemic infection. |
| Functional Deficit | Severe limitation of grasp, prehension, or occupational function due to fixed joint position. | Absolute: Severe, uncorrected articular incongruity or advanced post-traumatic osteoarthritis (salvage procedures indicated instead). |
| Anatomical Prerequisites | Intact or reconstructable extensor and flexor mechanisms. Sensate digit. | Relative: Poor soft tissue envelope (dense scarring, prior radiation, severe burn eschar) requiring preliminary flap coverage. |
| Patient Factors | Highly motivated patient, fully compliant, with a clear understanding of the prolonged rehabilitative commitment. | Relative: Lack of patient motivation, inability to participate in hand therapy, severe psychiatric non-compliance. |
| Specific Deformities | Isolated MCP extension contracture; PIP flexion contracture secondary to check-rein fibrosis. | Relative: Ischemic digit or severe neurovascular compromise where acute extension may precipitate necrosis. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Assessment and Imaging Modalities
Meticulous preoperative planning begins with high-quality imaging. Standard posteroanterior, true lateral, and oblique radiographs of the affected digit are mandatory. These images are scrutinized for articular congruity, joint space narrowing, osteophyte formation, and the presence of retained hardware or heterotopic ossification. If the articular surface is severely destroyed or arthritic, a soft tissue release will fail to restore painless, functional motion; in such cases, the surgeon must pivot the preoperative plan toward an arthrodesis or a joint arthroplasty.
Advanced imaging, while not routinely required for simple contractures, can be invaluable in complex post-traumatic scenarios. High-resolution ultrasound or Magnetic Resonance Imaging (MRI) without contrast can precisely delineate the extent of tendon adhesions, the integrity of the collateral ligaments, and the presence of occult intra-articular pathology such as loose bodies or chondral defects. This information allows the surgeon to anticipate the necessity for concurrent procedures, such as an extensive tenolysis or the excision of heterotopic bone, and to counsel the patient accordingly regarding expected operative time and outcomes.
Anesthesia, Tourniquet, and Positioning
The procedure is typically performed under regional anesthesia—specifically, an axillary or supraclavicular brachial plexus block. This provides excellent intraoperative anesthesia and profound muscle relaxation, which is critical for assessing the true passive range of motion intraoperatively once the fibrotic tethers have been released. Furthermore, regional anesthesia offers superior postoperative pain control, facilitating immediate mobilization in the recovery room. General anesthesia is reserved for patients with specific contraindications to regional blocks or those requiring extensive, multi-digit, prolonged reconstructions.

The patient is positioned supine with the operative extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Exsanguination with an Esmarch bandage and inflation of the tourniquet (typically to 250 mm Hg) is essential to provide a bloodless surgical field. The intricate dissection required to separate densely adherent capsular structures from delicate neurovascular bundles and thin extensor aponeuroses is impossible without pristine hemostasis. However, the surgeon must be mindful of tourniquet time, generally deflating it after two hours to allow for tissue reperfusion and to assess the vascularity of the digit, particularly after correcting severe flexion contractures.
Anticipating the Pathologic Cascade
The cornerstone of successful surgical mobilization is anticipating all potential pathologic causes of the contracture before making the initial incision. The surgeon must mentally rehearse the systematic, stepwise release of structures. For an MCP extension contracture, the anticipated sequence involves elevating the extensor mechanism, excising the dorsal capsule, releasing the proper collateral ligaments, and potentially addressing the volar plate.

For a PIP flexion contracture, the surgeon must be prepared to execute the classic stepwise approach popularized by Curtis. This begins with an assessment of the extensor mechanism, followed by the sequential release of the collateral ligaments, the volar plate (specifically the check-rein ligaments), and potentially a flexor tenolysis. The surgical plan must be fluid; the surgeon must continuously reassess the joint's passive motion after each sequential release, proceeding to the next anatomical tether only if adequate motion has not yet been achieved. This tailored approach prevents unnecessary destabilization of the joint.
Step-by-Step Surgical Approach and Fixation Technique
Metacarpophalangeal Joint Release Technique
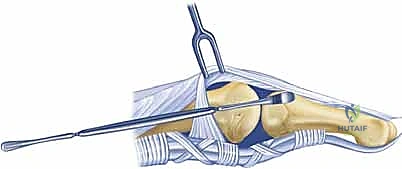
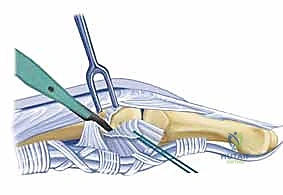
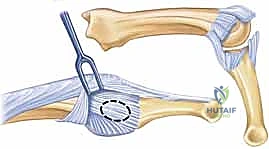
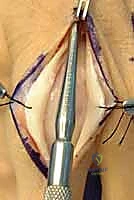
The surgical release of an MCP extension contracture is typically approached dorsally. A longitudinal incision is made directly over the metacarpal shaft, extending distally over the proximal phalanx. Alternatively, a dorsal curvilinear or lazy-S incision can be utilized to prevent a linear scar contracture. Meticulous subcutaneous dissection is performed to identify and retract the delicate dorsal sensory branches of the radial or ulnar nerves. The extensor mechanism is exposed.

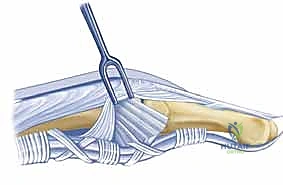
The EDC tendon is frequently adherent to the underlying capsule. The sagittal bands are identified on both the radial and ulnar aspects of the EDC. The extensor mechanism is longitudinally split, or the sagittal bands are carefully elevated from the underlying capsule to allow retraction of the EDC tendon laterally. This exposes the thickened, fibrotic dorsal capsule. A transverse or elliptical excision of the dorsal capsule is performed. Often, this initial step yields minimal improvement in flexion, indicating that the primary pathology lies within the collateral ligaments.

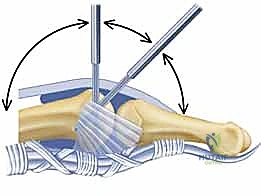
The proper collateral ligaments are identified originating from the metacarpal head tubercles. In a severe extension contracture, these ligaments are shortened, thickened, and densely scarred to the lateral condyles. Using a #15 blade, the proper collateral ligaments are sharply released from their proximal attachments on the metacarpal head or excised entirely. The accessory collateral ligaments, which fan out to the volar plate, are ideally preserved to maintain some degree of lateral stability, though they too must be released if they remain a tether to flexion. Following collateral ligament release, gentle, sustained passive flexion is applied. If resistance persists, a freer elevator is passed volarly to lyse adhesions between the volar plate and the metacarpal head. If the joint remains incongruous or tends to subluxate dorsally upon flexion, temporary transarticular Kirschner wire (K-wire) fixation in 70 degrees of flexion for 7-10 days may be necessary, though immediate mobilization is vastly preferred.
Proximal Interphalangeal Joint Release Technique
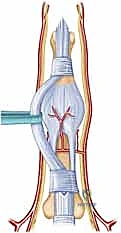
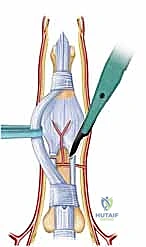
The release of a PIP flexion contracture is arguably more demanding. A midaxial incision (either radial or ulnar, depending on concurrent pathology) or a volar Bruner zig-zag incision is employed. The midaxial approach provides excellent exposure of the collateral ligaments and lateral aspect of the volar plate while remaining dorsal to the neurovascular bundle. The neurovascular bundle is identified, mobilized, and protected throughout the procedure.

Following the principles of Curtis, the release is performed sequentially. First, the lateral bands of the extensor mechanism are mobilized, and any adhesions to the proximal phalanx are lysed. Second, the transverse retinacular ligament is divided. Third, the proper collateral ligaments are assessed. If they are contracted and preventing extension, they are completely excised from their origin on the proximal phalanx to their insertion on the middle phalanx. Excision is preferred over simple transection to prevent the immediate reformation of scar tissue bridging the gap.
The critical step is the management of the volar plate. The accessory collateral ligaments are divided to allow access to the proximal aspect of the volar plate. The check-rein ligaments—the dense, fibrotic bands tethering the volar plate to the periosteum of the proximal phalanx—are identified and radically excised. The proximal margin of the volar plate must be completely freed, allowing it to glide distally as the joint is extended. If full extension is still not achieved, a flexor tenolysis within the A2 or A3 pulley region may be required. Once full, passive extension is obtained, the tourniquet is deflated to ensure the digital artery has not been placed under undue tension, which could precipitate vasospasm and digital ischemia.
Addressing Concomitant Soft Tissue Deficits
In cases involving severe crush injuries or burns, the overlying skin and subcutaneous tissues may be contracted, lacking the necessary elasticity to accommodate the newly restored joint motion. If the skin blanches or tears upon passive flexion (in MCP release) or extension (in PIP release), the surgeon must immediately address the soft tissue envelope. Forcing the joint into position under a tight skin closure will inevitably lead to wound breakdown, infection, and recurrent, more severe stiffness.

Local tissue rearrangements, such as Z-plasties or V-Y advancements, can provide minor gains in longitudinal length. However, significant skin deficits require the importation of healthy, vascularized tissue. Full-thickness skin grafts may be utilized if a healthy, vascularized paratenon or muscle bed is present. In the presence of exposed tendon or bone devoid of periosteum, a local or regional flap, such as a cross-finger flap, a reverse flow homodigital island flap, or even a free tissue transfer, becomes mandatory. The reconstructive ladder must be respected to ensure a durable, supple envelope that facilitates, rather than hinders, postoperative rehabilitation.
Complications, Incidence Rates, and Salvage Management
Intraoperative and Early Postoperative Risks
The surgical release of stiff digital joints is fraught with potential complications, demanding meticulous technique and vigilant postoperative care. Intraoperatively, the most devastating complication is iatrogenic injury to the neurovascular bundles, particularly during the deep dissection required for PIP volar plate release. Transection of a digital artery can compromise digital perfusion, especially if the contralateral vessel is previously injured or diseased. Injury to the digital nerve results in debilitating anesthesia or painful neuroma formation. Careful, magnified dissection and the routine use of vessel loops are imperative to mitigate this risk.
Another significant intraoperative risk is the creation of joint instability. Aggressive, non-selective excision of the capsuloligamentous structures, particularly the complete resection of both proper and accessory collateral ligaments without regard for the intrinsic stabilizers, can result in a flail, subluxating joint. This underscores the importance of the sequential, stepwise release technique. In the early postoperative period, hematoma formation is a primary concern. A hematoma serves as a potent nidus for infection and subsequent severe fibroplasia, effectively restarting the contracture cascade. Meticulous hemostasis prior to closure and the judicious use of small drains are recommended.
Wound dehiscence and marginal skin necrosis can occur if the skin is closed under excessive tension over a newly mobilized joint. If the skin cannot easily accommodate the new range of motion, the surgeon must leave the wound partially open to heal by secondary intention or immediately perform a skin graft or flap coverage. Infection, while relatively rare in elective hand surgery, is catastrophic in the setting of a joint release, as it invariably destroys the articular cartilage and leads to absolute, irreversible stiffness.
Long-Term Sequelae and Salvage Strategies
The most frequent and frustrating long-term complication is the recurrence of the contracture. Despite perfect surgical execution, the biology of scar formation can overwhelm the mechanical release, particularly in patients with a diathesis for hypertrophic scarring or those who fail to comply with the grueling postoperative therapy regimen. Recurrence rates for severe PIP flexion contractures can approach 30-40% in some series, highlighting the recal
Clinical & Radiographic Imaging Archive