Volar Plate Arthroplasty: A Masterclass in PIP Joint Reconstruction
Key Takeaway
This masterclass guides fellows through Volar Plate Arthroplasty (VPA) for Proximal Interphalangeal (PIP) joint fracture-dislocations. We'll cover comprehensive surgical anatomy, meticulous preoperative planning, and granular intraoperative execution, from incision to K-wire fixation. Expect detailed instrument use, real-time decision-making, and extensive pearls to manage complications and optimize patient outcomes, ensuring stable, functional joint reconstruction.
Welcome, colleagues, to this comprehensive masterclass on proximal interphalangeal (PIP) joint reconstruction. Today, we address one of the most challenging yet rewarding pathologies in hand surgery: the chronic dorsal fracture-dislocation of the PIP joint. When conservative management fails or initial injuries are neglected, patients present with profound instability, debilitating pain, and significant functional deficits. Our definitive surgical solution in these complex scenarios is the Volar Plate Arthroplasty (VPA). This elegant, anatomically sound technique provides a critical volar restraint against dorsal subluxation, effectively resurfacing the injured volar articular portion of the middle phalanx using autologous local tissue—the volar plate itself.
It is crucial to understand that even seemingly innocuous PIP joint injuries can precipitate protracted symptoms, including fusiform swelling, recalcitrant stiffness, and chronic pain that invariably exceeds patient expectations. While the principles of VPA can theoretically be extrapolated to the distal interphalangeal (DIP) joint, its primary and most successful application remains at the PIP joint. This preference is dictated by the anatomical complexities introduced by the flexor digitorum profundus (FDP) insertion at the base of the distal phalanx, which significantly complicates DIP exposure and reconstruction. This chapter will serve as your definitive guide to mastering the nuances of PIP joint Volar Plate Arthroplasty.
Comprehensive Introduction and Patho-Epidemiology
The proximal interphalangeal joint is frequently described as the functional workhorse of the human digit, responsible for the majority of the arc of motion required for power grip and fine pinch kinematics. Consequently, any disruption to its congruent articular surfaces or ligamentous stabilizers results in disproportionate functional impairment. Dorsal fracture-dislocations of the PIP joint represent a spectrum of severe trauma, typically resulting from a combination of longitudinal axial loading and hyperextension forces. These mechanisms are ubiquitous in athletic endeavors, particularly ball sports, as well as in high-energy occupational accidents.
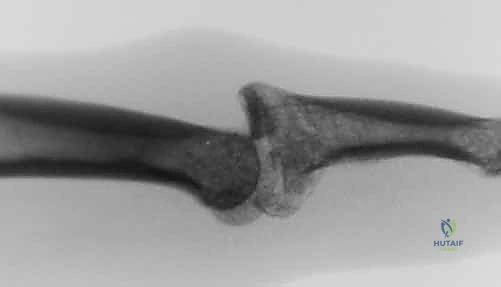
The pathogenesis of this specific injury pattern involves the middle phalanx being driven forcefully in a dorsal and proximal direction against the unyielding condyles of the proximal phalanx. This violent impaction shears off the volar lip of the middle phalanx base, creating an articular defect and simultaneously avulsing the critical distal insertion of the volar plate. When the articular fracture fragment encompasses a significant portion of the volar base, the cupping mechanism of the middle phalanx is lost, rendering the joint inherently unstable and prone to recurrent dorsal subluxation.
Chronic subluxation or dislocation—generally defined in the literature as presenting more than six weeks post-injury—is an unfortunately common clinical scenario. This delay often stems from the initial trauma being erroneously dismissed by primary care providers or the patient as a simple "finger sprain." As the joint remains in a subluxated state, a cascade of pathological changes ensues. The collateral ligaments contract in their shortened, abnormal position, the volar plate scars into the collateral recesses, and the articular cartilage, deprived of normal contact mechanics and synovial fluid nutrition, begins to degenerate. Without definitive surgical intervention, this chronic instability inevitably culminates in severe, painful post-traumatic osteoarthritis.
Detailed Surgical Anatomy and Biomechanics
Before initiating any surgical incision, a profound, three-dimensional understanding of the PIP joint's complex surgical anatomy is mandatory. The PIP joint is a highly constrained bicondylar hinge joint, and its stability relies on a delicate interplay of precise osseous geometry and robust soft-tissue stabilizers. Mastery of these structures is the foundation of a successful volar plate arthroplasty.
Ligamentous Restraints and the Volar Plate
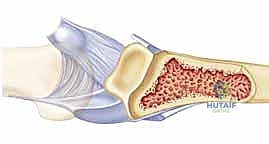
The volar plate (VP) is a dense, fibrocartilaginous structure that serves as the primary static restraint against hyperextension of the PIP joint. It is situated on the palmar aspect of the joint capsule, effectively separating the articular cavity from the overlying flexor tendon sheath. Proximally, the volar plate originates from the proximal phalanx via two robust, lateral fascial bands known as the proximal checkrein ligaments, giving it a characteristic "swallowtail" appearance. These checkrein ligaments are vital for the normal proximal-distal gliding motion of the plate during digital flexion and extension. During our surgical approach, releasing these checkreins is often a mandatory step to achieve sufficient distal advancement of the volar plate into the fracture defect.
Distally, the volar plate transitions into a thick cartilaginous structure that inserts firmly into the volar lip of the middle phalanx base. This central insertion is augmented laterally by a conjoined insertion with the proper and accessory collateral ligaments. The normal kinematic behavior of the volar plate involves it sliding proximally during joint flexion to prevent impingement, and advancing distally during extension to tension the joint capsule and prevent hyperextension.

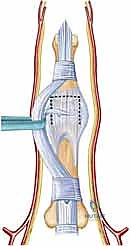
The collateral ligament complex is equally critical. Originating from the dorsal-lateral aspects of the proximal phalanx condyles, the proper collateral ligaments course obliquely to insert on the volar-lateral base of the middle phalanx. They are the primary restraints to lateral deviation. The accessory collateral ligaments fan out more volarly to insert directly into the lateral margins of the volar plate. Together, the volar plate and the bilateral collateral ligament complexes form a highly stable, three-dimensional "box" configuration. In chronic dorsal subluxations, the oblique orientation of these ligaments causes them to contract, effectively tethering the middle phalanx in its dorsally displaced position and necessitating sequential surgical release.
Musculotendinous and Neurovascular Relationships
The musculotendinous units traversing the PIP joint exert significant deforming forces in the setting of instability. The flexor digitorum superficialis (FDS) bifurcates at the level of the proximal phalanx, wrapping around the flexor digitorum profundus (FDP) at Camper's chiasm, before inserting broadly onto the volar-lateral aspects of the middle phalanx shaft, just distal to the joint capsule. In a volar plate-deficient joint, the powerful proximal pull of the FDS vector accentuates the dorsal subluxation of the middle phalanx base. Conversely, the central slip of the extensor mechanism inserts onto the dorsal base of the middle phalanx. We must maintain absolute vigilance regarding the central slip during our reconstruction, particularly when passing sutures dorsally through the middle phalanx, to avoid iatrogenic extensor lag or boutonniere deformity.
The neurovascular anatomy demands meticulous attention. The radial and ulnar digital neurovascular bundles course longitudinally along the lateral aspects of the digit, intimately associated with Cleland's and Grayson's ligaments. They lie immediately adjacent to our surgical field and are highly vulnerable during the volar approach, particularly when the PIP joint is hyperextended to gain articular exposure (the "shotgun" maneuver). Meticulous identification, mobilization, and gentle retraction of these bundles are non-negotiable steps to prevent catastrophic traction neuropraxia or vascular compromise.
Osteology and Articular Geometry
The osseous architecture of the PIP joint dictates its inherent kinematic stability. The head of the proximal phalanx features two asymmetric condyles separated by an intercondylar notch. The radial condyle is typically larger, contributing to the slight ulnar deviation observed during normal digital flexion. A pristine, normal articular contour of these proximal phalangeal condyles is an absolute prerequisite for a successful volar plate arthroplasty; if the condyles are severely damaged, the advanced volar plate will rapidly degenerate against the irregular surface.
The base of the middle phalanx presents two corresponding concave articular facets separated by a median ridge. In dorsal fracture-dislocations, it is the volar aspect of these facets that is sheared away. For a VPA to be biomechanically viable, the surgeon must identify an intact dorsal cortex and a sufficient remnant of the dorsal articular cartilage on the middle phalanx. This dorsal remnant provides the essential buttress against which the proximal phalanx condyles will articulate, while the advanced volar plate reconstructs the deficient volar cup.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of surgical success in PIP joint reconstruction. Volar plate arthroplasty is a technically demanding procedure that requires specific anatomical prerequisites to function effectively. The primary goal is to restore a stable, concentric reduction that permits early active motion, thereby minimizing stiffness while preventing recurrent subluxation.
The classic indication for VPA is an acute dorsal fracture-dislocation of the PIP joint that remains persistently unstable following attempted closed reduction, particularly when the volar articular fragment is severely comminuted and not amenable to primary screw or pin fixation. Furthermore, VPA is the gold standard for chronic, neglected subluxations or dislocations—even those presenting up to two years post-injury—provided the articular cartilage of the proximal phalanx remains viable. If dynamic fluoroscopy demonstrates that more than 30 to 45 degrees of flexion is required to maintain a concentric joint reduction, non-operative management is destined to fail, and surgical reconstruction is mandated.
Patient Selection Criteria
| Parameter | Indications for Volar Plate Arthroplasty | Contraindications for Volar Plate Arthroplasty |
|---|---|---|
| Chronicity | Acute unstable injuries; Chronic neglected dislocations (>6 weeks). | Acute injuries amenable to simple closed reduction and splinting. |
| Articular Defect | Volar base fracture involving 30% to 50% of the articular surface. | Volar base fracture involving >60% of the articular surface (consider Hemi-Hamate). |
| Dorsal Cortex | Intact dorsal cortex and dorsal articular cartilage on the middle phalanx. | Fractures extending into or compromising the dorsal cortex/central slip insertion. |
| Proximal Phalanx | Intact, smooth, and congruent articular condyles. | Severe osteochondral damage or degenerative arthritis of the proximal phalanx head. |
| Soft Tissue | Viable volar plate tissue available for advancement. | Active local infection; severe, uncorrectable soft tissue contractures preventing reduction. |
It is imperative to recognize that fractures involving more than 50% to 60% of the middle phalanx articular surface stretch the biomechanical limits of VPA. In these massive defects, the advanced volar plate may fail to provide sufficient volar support, leading to recurrent dorsal subluxation. In such extreme cases, alternative salvage procedures, such as hemi-hamate autograft arthroplasty or primary PIP joint arthrodesis, must be strongly considered.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative evaluation relies heavily on high-quality radiographic imaging. Every patient presenting with a PIP joint injury requires a dedicated trauma series consisting of true anteroposterior (AP), true lateral, and oblique radiographs of the individual digit. The AP view is scrutinized for collateral avulsions, joint space narrowing, and coronal plane alignment. However, the true lateral radiograph is the single most critical diagnostic tool.
Radiographic Evaluation and Advanced Imaging
On a perfect lateral view, the surgeon must meticulously evaluate the congruency of the articular surfaces. In the setting of dorsal subluxation, a characteristic radiographic finding known as the "dorsal V sign" is frequently observed. This sign, originally described by Light, indicates that the articular surfaces of the proximal and middle phalanges are neither congruent nor parallel, forming a V-shaped radiolucency that diverges dorsally. This subtle finding confirms persistent instability even if the joint appears clinically reduced.

While standard radiographs are usually sufficient for diagnosis, they frequently underestimate the true extent of the articular comminution and bone loss. In chronic or highly complex cases, a dedicated Computed Tomography (CT) scan with 3D reconstructions can be invaluable. CT precisely delineates the percentage of articular surface involvement, the exact location of fracture lines, and the presence of intra-articular loose bodies, allowing the surgeon to definitively plan between a VPA, hemi-hamate graft, or arthrodesis before entering the operating room.
Operating Room Setup and Anesthesia Considerations
The procedure is typically performed under regional anesthesia (supraclavicular or axillary brachial plexus block) combined with intravenous sedation, though a wide-awake local anesthesia no tourniquet (WALANT) approach can be utilized by experienced surgeons to assess active motion intraoperatively. The patient is positioned supine with the affected upper extremity extended onto a radiolucent hand table.
An upper arm pneumatic tourniquet is applied and inflated to ensure a completely bloodless surgical field, which is an absolute necessity for the meticulous micro-dissection required around the digital neurovascular bundles. A mini C-arm fluoroscopy unit is draped sterilely and positioned perpendicular to the hand table. The ability to obtain dynamic, magnified, true lateral fluoroscopic images throughout the procedure is critical for assessing the initial reduction, confirming precise drill hole placement, and evaluating the final stability of the arthroplasty.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a volar plate arthroplasty is an exercise in precision, demanding a deep respect for the delicate soft tissue envelope of the digit. The following steps detail the classical approach, optimized for maximum exposure and secure fixation.
Incision and Superficial Dissection
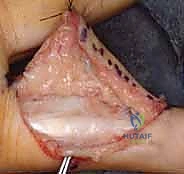
The operation commences with a meticulously planned volar incision. A standard Bruner (zigzag) incision is highly recommended, centered precisely over the PIP joint flexion crease. The apices of the incision should extend to the mid-axial lines radially and ulnarly. Alternatively, a mid-lateral incision can be utilized, but the Bruner approach offers superior, extensile exposure of the entire volar apparatus.
Upon incising the skin, careful blunt dissection through the subcutaneous adipose tissue is performed to elevate full-thickness flaps. The immediate objective is to identify and protect the radial and ulnar digital neurovascular bundles. Using fine tenotomy scissors or a mosquito hemostat, the bundles are dissected free from the surrounding fascial bands (Cleland's and Grayson's ligaments) and gently mobilized laterally. Retraction must be gentle to avoid traction neuritis.

Flexor Sheath Management and Joint Exposure
With the neurovascular bundles safely retracted, the flexor tendon sheath is exposed. The surgeon must identify the A2, C1, A3, C2, and A4 pulleys. To access the volar plate, the sheath is typically opened by incising the C1, A3, and C2 pulleys, while strictly preserving the critical A2 and A4 pulleys to prevent subsequent flexor tendon bowstringing. The flexor digitorum superficialis and profundus tendons are then gently retracted laterally, revealing the underlying volar plate and the PIP joint capsule.


To gain comprehensive access to the articular surfaces, a "shotgun" exposure is frequently employed. This involves incising the accessory collateral ligaments bilaterally where they insert into the volar plate. If the joint remains tight, particularly in chronic cases, a sequential release of the proper collateral ligaments from their proximal phalangeal origins may be required. The PIP joint is then forcefully hyperextended, opening the joint space like a shotgun breech. This maneuver provides unparalleled visualization of the proximal phalanx condyles and the fractured base of the middle phalanx.
Joint Preparation and Volar Plate Advancement
Once exposed, the joint is thoroughly irrigated and debrided. All fracture hematoma, fibrous scar tissue, and loose, non-viable osteochondral fragments are meticulously excised using a fine rongeur or curette. The volar base of the middle phalanx is then prepared to receive the volar plate. A small, high-speed burr or curette is used to create a transverse bony trough at the base of the middle phalanx, exposing bleeding cancellous bone to promote robust soft-tissue-to-bone healing.
Attention is then turned to the volar plate itself. To allow sufficient distal advancement, the proximal checkrein ligaments must be identified and sharply released from the proximal phalanx. The distal, cartilaginous margin of the volar plate is then debrided to a fresh, healthy edge. A robust, non-absorbable suture (e.g., 2-0 or 3-0 braided polyester or FiberWire) is woven through the distal margin of the volar plate. A modified Kessler, Krackow, or multiple horizontal mattress suture configuration can be utilized to ensure a secure, tear-resistant grasp of the fibrocartilaginous tissue.

Suture Fixation and Dynamic Assessment
The final, critical step is securing the advanced volar plate into the prepared bony trough. Using a 0.035-inch or 0.045-inch Kirschner wire or a specialized micro-drill, two parallel drill holes are created, starting from the volar bony trough and exiting dorsally through the middle phalanx. It is absolutely imperative that these drill holes exit dorsal to the mid-axial line; if they are placed too volarly, the advanced plate will not provide a sufficient volar buttress, and the joint will re-subluxate. Furthermore, the surgeon must ensure the drill bit does not compromise the central slip insertion on the dorsal cortex.
The two tails of the suture previously woven into the volar plate are then passed through these intraosseous tunnels using a suture passer or straight Keith needles.

As the sutures are tensioned dorsally, the volar plate is drawn deeply into the cancellous trough, effectively resurfacing the volar articular defect. The joint is reduced, and the sutures are tied firmly over the dorsal cortex. To prevent the sutures from cutting through the dorsal skin or bone, they are typically tied over a sterile padded button.

Before closing, the stability of the reconstruction must be dynamically assessed. The tourniquet is deflated, and hemostasis is achieved. Under live fluoroscopy, the PIP joint is taken through a full range of motion. The surgeon must confirm that the joint remains concentrically reduced without any dorsal subluxation, particularly in full extension.

If the joint hinges or subluxates, the tension on the volar plate must be adjusted, or supplemental temporary transarticular K-wire fixation (typically holding the joint in 20-30 degrees of flexion for 2-3 weeks) may be required. Once stability is confirmed, the skin is loosely approximated with non-absorbable sutures to accommodate postoperative swelling.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, volar plate arthroplasty is associated with a distinct complication profile. The delicate balance between achieving joint stability and maintaining functional mobility makes the postoperative course challenging. Surgeons must be prepared to identify and manage these complications aggressively.
Intraoperative and Early Postoperative Complications
Intraoperatively, the most devastating complication is iatrogenic injury to the digital neurovascular bundles. This typically occurs during the "shotgun" exposure if the bundles have not been adequately mobilized and protected. Early postoperative complications include superficial skin necrosis or infection, particularly under the dorsal button. The button must be padded adequately and monitored closely; if skin breakdown is imminent, the button may need to be removed prematurely, relying on scar tissue for residual stability.
Loss of reduction in the early postoperative phase is a catastrophic failure, usually resulting from technical errors such as inadequate volar plate advancement, drill holes placed too volarly, or failure to recognize an articular defect exceeding 60%. If early recurrent dorsal subluxation occurs, immediate revision surgery is mandated, often requiring conversion to a salvage procedure.
Late Complications and Degenerative Changes
The most ubiquitous late complication following VPA is PIP joint stiffness. A flexion contracture of 10 to 20 degrees is exceedingly common and is often considered an acceptable trade-off for a stable, pain-free joint. However, severe stiffness severely limits digital function. This underscores the critical importance of early, supervised active range of motion protocols.
| Complication | Estimated Incidence | Prevention and Salvage Management |
|---|---|---|
| PIP Joint Stiffness / Flexion Contracture | 40% - 60% | Prevention: Meticulous hemostasis, early active ROM in dorsal block splint. Management: Dynamic extension splinting; late surgical tenolysis/capsulotomy if refractory. |
| Recurrent Dorsal Subluxation | 5% - 15% | Prevention: Strict adherence to <50% articular defect indication; proper dorsal drill hole placement. Management: Revision to Hemi-Hamate arthroplasty or PIP Arthrodesis. |
| Dorsal Skin Necrosis (Button) | 2% - 5% | Prevention: Adequate padding beneath the button; avoiding excessive suture tension. Management: Local wound care; early button removal; local rotational flaps if severe. |
| Post-Traumatic Osteoarthritis | 20% - 30% (Long-term) | Prevention: Achieving perfect concentric reduction; avoiding VPA in severely damaged proximal phalanges. Management: NSAIDs, injections; ultimate salvage via Arthrodesis or Silicone Arthroplasty. |
Long-term follow-up studies indicate that mild to moderate radiographic osteoarthritis is common, though it does not always correlate with clinical symptoms. If painful, end-stage arthritis develops years later, salvage options include PIP joint arthrodesis (typically fused in 40-50 degrees of flexion for the index/long fingers, and more flexion for the ring/small fingers) or, in select low-demand patients, silicone implant arthroplasty.
Phased Post-Operative Rehabilitation Protocols
The success of a volar plate arthroplasty is as dependent on the postoperative rehabilitation protocol as it is on the surgical execution. The rehabilitation strategy must delicately balance the protection of the healing volar plate reconstruction with the imperative need to prevent debilitating joint stiffness. Collaboration with a skilled Certified Hand Therapist (CHT) is essential.
Early Protective Phase
Immediately postoperatively, the digit is immobilized in a bulky compressive dressing with a dorsal plaster splint holding the PIP joint in approximately 20 to 30 degrees of flexion, and the metacarpophalangeal (MCP) joint in 70 degrees of flexion. At 3 to 5 days post-surgery, the bulky dressing is removed, and a custom thermoplastic dorsal block splint is fabricated. This splint maintains the PIP joint in 20-30 degrees of flexion to prevent tension on the advanced volar plate.
Crucially, early active range of motion (AROM) is initiated within the constraints of this dorsal block splint. The patient is instructed to perform active flexion exercises, pulling the digit away from the dorsal block, followed by active extension up to the limit of the splint. This controlled motion prevents tendon adhesions and promotes organized collagen deposition in the healing volar plate, without risking hyperextension and recurrent subluxation.
Intermediate and Late Strengthening Phases
At approximately 3 to 4 weeks postoperatively, the dorsal pull-out button and sutures are removed in the clinic. The dorsal block splint is gradually extended by 10 degrees each week, progressively challenging the healing reconstruction. By 6 weeks, the splint is typically discontinued during the day, though it may be worn at night for an additional 2 weeks.
If a residual flexion contracture persists beyond 6 to 8 weeks, dynamic or static progressive extension splinting may be initiated, provided radiographic healing is confirmed and the joint remains concentrically reduced. Strengthening exercises, including putty and grip strengthening, are generally introduced at 8 weeks. Patients must be counseled that maximal medical improvement may take up to 6 to 12 months, and a slight residual flexion contracture is a normal and acceptable outcome.
Summary of Landmark Literature and Clinical Guidelines
The conceptual foundation of the volar plate arthroplasty was pioneered by Eaton and Malerich in their landmark 1980 publication. They were the first to systematically describe the advancement of the volar plate into the middle phalanx defect, fundamentally changing the management of chronic PIP fracture-dislocations. Their initial series demonstrated a reliable restoration of stability and a functional, albeit slightly restricted, arc of motion.
Subsequent long-term outcome studies, such as those by Dionysian and Eaton, have validated the durability of this procedure. While acknowledging the high incidence of mild flexion contractures (averaging 15 degrees) and radiographic degenerative changes over a 10-year follow-up, these studies confirm that the vast majority of patients maintain a stable, pain-free joint with a functional arc of motion averaging 70 to 80 degrees.
Current clinical guidelines emphasize that while newer techniques, such as hemi-hamate autografting, have gained popularity for massive articular defects (>50%), the classic volar plate arthroplasty remains the gold standard for defects comprising 30% to 50% of the articular surface. Mastery of this technique provides the orthopedic hand surgeon with a powerful, reliable tool to salvage one of the most challenging injuries in the upper extremity, restoring function to the critical PIP joint.
