Mastering the Weil Lesser Metatarsal Shortening Osteotomy: An Intraoperative Guide

Key Takeaway
This masterclass provides an exhaustive, real-time guide to the Weil lesser metatarsal shortening osteotomy. Fellows will learn intricate surgical anatomy, meticulous preoperative planning, and granular intraoperative execution from a master surgeon's perspective. We'll cover precise instrument handling, critical pearls and pitfalls, and comprehensive postoperative management, ensuring a deep understanding of this essential forefoot procedure for metatarsalgia and MTP joint instability.
Comprehensive Introduction and Patho-Epidemiology
Metatarsalgia stemming from metatarsophalangeal (MTP) joint subluxation or dislocation is a ubiquitous, yet highly complex, forefoot pathology that routinely challenges orthopedic surgeons. The Weil lesser metatarsal shortening osteotomy has firmly established itself as a cornerstone, joint-preserving, intra-articular procedure that effectively restores forefoot biomechanics. Originally conceptualized by L.S. Weil in 1992 and subsequently popularized in the peer-reviewed literature by Barouk in 1996, this technique provides a highly reliable method to address excessive metatarsal length and the resulting pressure imbalance that drives forefoot morbidity. Unlike historical alternatives—such as isolated dorsal soft tissue releases with K-wire fixation, silicone arthroplasties, or destabilizing excisional arthroplasties—the Weil osteotomy directly corrects the osseous architectural fault without sacrificing the critical plantar intrinsic musculature attachments.

The core pathophysiological driver of this condition is the progressive attenuation and ultimate failure of the plantar plate. The plantar plate is a robust, fibrocartilaginous structure that serves as the primary static restraint against MTP joint hyperextension. Functionally, it acts as a critical load-bearing cushion during the terminal stance phase of gait. When subjected to repetitive microtrauma, often exacerbated by an excessively long lesser metatarsal or a hypermobile first ray, the plantar plate undergoes degenerative tearing. As the plate fails, the delicate balance of the MTP joint is disrupted, initiating a predictable cascade of instability. The proximal phalanx begins to subluxate dorsally, driven by the now-unopposed pull of the extensor digitorum longus (EDL) and extensor digitorum brevis (EDB).
Epidemiologically, this pathology predominantly affects women in their fifth to seventh decades of life, often correlating with a history of wearing constrictive, high-heeled footwear that forces the MTP joints into non-physiologic extension. However, it is also frequently observed in patients with systemic inflammatory arthropathies, such as rheumatoid arthritis, or those with underlying neuromuscular imbalances. The condition is rarely isolated; it frequently presents concomitantly with hallux valgus. A severe hallux valgus deformity compromises the weight-bearing capacity of the first ray, leading to transfer metatarsalgia. Furthermore, the laterally deviating hallux physically abuts the second digit, mechanically forcing it into a crossover toe deformity and accelerating the rupture of the lateral collateral ligament and plantar plate of the second MTP joint.
Understanding this progressive patho-epidemiology is paramount. Once the plantar plate is compromised, the dorsal capsule and extensor tendons undergo adaptive shortening, creating a rigid, chronic dislocation. The intrinsic muscles (lumbricals and interossei), whose line of action normally passes plantar to the MTP joint axis of rotation to aid in plantarflexion, migrate dorsally. Once their line of pull shifts dorsal to the axis of rotation, they paradoxically become MTP joint extensors, further exacerbating the deformity. The Weil osteotomy, by shortening the metatarsal, effectively decompresses the joint, relaxes the contracted dorsal soft tissues, and realigns the intrinsic muscle vectors, thereby breaking this vicious cycle of instability.
Detailed Surgical Anatomy and Biomechanics
Mastery of the Weil osteotomy requires a profound, three-dimensional understanding of the surgical anatomy and the biomechanical consequences of altering the lesser ray architecture. The MTP joint is a condyloid joint formed by the convex metatarsal head and the shallow, concave articular surface of the proximal phalanx base. The stability of this joint relies heavily on its ligamentous and capsular envelope rather than bony congruency. The aforementioned plantar plate is the most critical structure, attaching firmly to the base of the proximal phalanx and blending proximally with the plantar fascia. Crucially, the plantar plate has no substantial, direct fibrous attachment to the plantar aspect of the metatarsal neck or head; its connection is mediated primarily through the collateral ligaments.

This specific anatomical arrangement is the precise reason why the Weil osteotomy is so biomechanically sound. By performing an extra-articular cut through the metatarsal neck and shifting the capital fragment proximally, the surgeon shortens the bone without stripping the plantar soft tissue attachments from the metatarsal head. The plantar plate, intrinsic tendons, and plantar vascular supply remain tethered to the capital fragment. As the head translates proximally, it effectively shifts the weight-bearing epicenter to a more compliant, proximal region of the plantar fat pad, relieving the focal pressure beneath the original metatarsal head location.
The extensor mechanism must be meticulously managed during this procedure. The Extensor Digitorum Longus (EDL) tendon is the primary dorsal structure encountered. It courses over the MTP joint to insert on the middle and distal phalanges. In chronic subluxation, the EDL is severely contracted and acts as a deforming force, necessitating formal lengthening. Lateral to the EDL lies the Extensor Digitorum Brevis (EDB) tendon, which inserts into the lateral aspect of the EDL tendon hood. The EDB often contributes to lateral deviation and dorsal contracture and is typically resected or tenotomized to facilitate joint reduction. Deep to these tendons lies the dorsal joint capsule, which will be thick and contracted.
Neurovascular preservation is a critical component of the surgical approach. The dorsal digital nerves, terminal branches of the superficial fibular nerve, course longitudinally in the subcutaneous tissues and are highly susceptible to iatrogenic transection or traction neuropraxia during retraction. Similarly, the dorsal metatarsal arteries and the robust dorsal venous plexus lie within the intermetatarsal spaces. The plantar blood supply to the metatarsal head is derived from branches of the plantar metatarsal arteries that enter the capsule plantarly and laterally. Excessive stripping of the plantar capsule during the osteotomy can disrupt this tenuous blood supply, leading to avascular necrosis (Freiberg's infraction iatrogenica). Therefore, the saw cut must be precise, and plantar soft tissue dissection must be strictly avoided.
Exhaustive Indications and Contraindications
Patient selection is the primary determinant of success in forefoot reconstruction. The Weil osteotomy is a powerful tool, but its application must be strictly governed by clinical and radiographic criteria. The decision to proceed with surgery should only follow a comprehensive trial of conservative management, including custom orthotics with metatarsal offloading pads, shoe modifications (rocker-bottom soles, wide toe boxes), non-steroidal anti-inflammatory drugs, and targeted corticosteroid injections (used judiciously to avoid accelerating plantar plate rupture).
| Category | Specific Conditions | Rationale / Clinical Context |
|---|---|---|
| Indications | Metatarsalgia with MTP Joint Subluxation/Dislocation | The classic indication. Shortening decompresses the joint and allows reduction of the proximal phalanx. |
| Disproportionately Long Lesser Metatarsal | Corrects the underlying architectural fault causing focal plantar overload and keratosis. | |
| Crossover Toe Deformity | Used in conjunction with soft tissue balancing (collateral ligament repair/plantar plate repair) to restore alignment. | |
| Freiberg's Infraction (Late Stage) | Decompresses the joint; the osteotomy can be angled to rotate healthy plantar cartilage dorsally into the articulation. | |
| Severe Multi-Ray Rheumatoid Deformity | Allows for joint preservation in select RA patients, avoiding the traditional pan-metatarsal head resection. | |
| Contraindications | Active Local or Systemic Infection | Absolute contraindication. Risk of deep space osteomyelitis. |
| Severe Peripheral Arterial Disease (PAD) | Relative to Absolute. Poor vascularity precludes osseous healing and soft tissue recovery. | |
| Charcot Neuroarthropathy (Active) | High risk of nonunion, hardware failure, and exacerbation of the neuroarthropathic process. | |
| Isolated Plantar Keratosis without MTP Instability | A distal metatarsal elevation osteotomy (e.g., BRT or DMMO) may be more appropriate than a Weil shortening. | |
| Inadequate Bone Stock / Severe Osteoporosis | Relative contraindication. May lead to hardware pull-out, cut-out, or intraoperative fracturing of the capital fragment. |
Differentiating mechanical metatarsalgia from a Morton's neuroma is a critical preoperative diagnostic step. While both present with forefoot pain, neuroma pain is typically neuralgic (burning, electric), radiates into the toes, and is exacerbated by lateral compression of the forefoot (Mulder's sign). Conversely, mechanical metatarsalgia presents with localized pain directly beneath the metatarsal head, often accompanied by a palpable plantar keratosis and pain upon dorsal translation of the proximal phalanx (the Drawer test). It is not uncommon for a patient to have both; however, addressing a neuroma without correcting the underlying mechanical overload will inevitably lead to persistent symptoms.
Furthermore, the surgeon must evaluate the entire forefoot as a functional unit. Performing an isolated lesser metatarsal osteotomy in the presence of an untreated, hemodynamically significant hallux valgus or first ray hypermobility is a recipe for failure. The unstable first ray will continue to transfer loads laterally, leading to recurrent subluxation of the operated toe or the development of transfer metatarsalgia to an adjacent, previously asymptomatic lesser metatarsal. Therefore, concurrent first ray stabilization (e.g., Lapidus arthrodesis or Scarf osteotomy) is frequently mandated.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning forms the blueprint for a successful Weil osteotomy. The clinical examination provides the functional context, while radiographic analysis yields the quantitative data required for precise surgical execution. The physical examination must meticulously document the presence and location of plantar keratoses, the reducibility of hammer toe deformities, and the integrity of the MTP joint using the dorsal Drawer test.

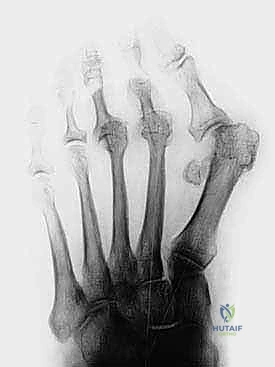
Standard weight-bearing dorsoplantar (AP) and lateral radiographs of the foot are mandatory. On the AP view, the surgeon must assess joint congruency. A dorsally dislocated proximal phalanx will project directly over the metatarsal head, creating the classic "gun barrel" sign. The clear space of the MTP joint should be evaluated; diminution of this space suggests chronic hyperextension and cartilage wear. The most critical measurement, however, is the relative metatarsal length. The Maestro curve, or a simple comparative measurement utilizing the first metatarsal as a reference, is employed. The ideal cascade dictates that the second metatarsal should be equal in length to, or slightly shorter than, the first metatarsal, with a progressive shortening of the third, fourth, and fifth metatarsals.
Templating the osteotomy is a quantitative exercise. Using digital templating software or a physical ruler on the radiographs, the surgeon calculates the exact millimeter discrepancy. For instance, if the second metatarsal projects 4mm distal to the ideal Maestro line, a 4mm to 5mm shortening is planned. It is crucial to understand the trigonometry of the Weil cut: because the osteotomy is angled (typically 10 to 15 degrees relative to the longitudinal axis of the metatarsal, aiming to be parallel to the plantar aspect of the foot), the amount of proximal translation required to achieve a specific longitudinal shortening is greater than the shortening itself.
Patient positioning and operating room setup must be optimized for efficiency and visualization. The patient is positioned supine on the operating table. It is highly advantageous to position the patient's foot at the extreme distal edge of the table. A small bump or rolled blanket is placed beneath the ankle. This specific positioning allows the surgeon to maximally plantarflex the MTP joint during the procedure, which is absolutely critical for exposing the metatarsal head and achieving the correct trajectory for the saw blade.
An Esmarch bandage is utilized to exsanguinate the limb, and a pneumatic ankle tourniquet is inflated (typically to 250 mmHg) to ensure a pristine, bloodless surgical field. This is vital for identifying the delicate dorsal digital nerves and achieving meticulous hemostasis. The fluoroscopy unit (C-arm) is positioned on the contralateral side of the table, draped sterilely, and oriented to allow rapid acquisition of both AP and lateral views of the forefoot without compromising the sterile field or requiring awkward repositioning of the limb.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the Weil osteotomy demands precision, respect for soft tissue envelopes, and an acute awareness of spatial geometry. We typically begin with a 3-cm longitudinal incision centered directly over the dorsal aspect of the affected metatarsal, extending from the distal metatarsal diaphysis to the proximal interphalangeal (PIP) joint.

Careful superficial dissection is performed using blunt retractors to sweep the dorsal venous plexus and the dorsal digital nerves medially and laterally, protecting them from the operative field.
Once the extensor hood is exposed, the Extensor Digitorum Longus (EDL) tendon is identified. In cases of chronic deformity, this tendon is invariably contracted and requires a formal Z-plasty lengthening.

A longitudinal incision is made down the midline of the EDL, followed by opposing transverse hemi-transections at the proximal and distal extents of the longitudinal cut. The tendon flaps are retracted, providing direct access to the underlying MTP joint capsule.

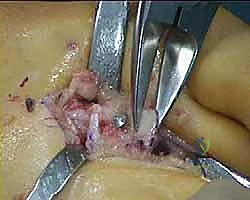
A longitudinal dorsal capsulotomy is then performed. To fully mobilize the joint and allow for exposure of the metatarsal head, the collateral ligaments must be released from their metatarsal epicondylar attachments.

Using a McGlamry elevator or a Freer elevator, the plantar capsule is gently swept off the plantar aspect of the metatarsal head, but strictly limited to the intra-articular space to avoid damaging the plantar blood supply. The toe is then acutely plantarflexed to 90 degrees, delivering the metatarsal head fully into the dorsal wound.

The osteotomy is the most critical phase. Using a fine-toothed sagittal saw, the cut is initiated at the dorsal edge of the articular cartilage.

The trajectory of the saw blade is paramount. It must be oriented parallel to the plantar weight-bearing surface of the foot, which typically corresponds to an angle of 10 to 15 degrees plantar to the longitudinal axis of the metatarsal shaft.
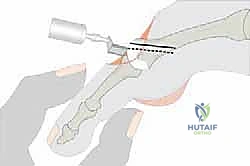
If the cut is made too steep (too plantarflexed), shifting the head proximally will simultaneously drive it plantarly, exacerbating the plantar keratosis. If the cut is too dorsal, the head elevates, leading to transfer metatarsalgia.
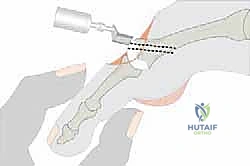
The saw is advanced smoothly through the metatarsal neck and shaft, ensuring a single, planar cut to maximize bony contact for healing.

Once the osteotomy is complete, a specialized Weil retractor or a towel clip is used to grasp the capital fragment.

The head is then translated proximally by the pre-calculated amount determined during templating (e.g., 4mm).

Because of the angle of the cut, the proximal translation results in a small dorsal overhang of the proximal diaphyseal bone.

While maintaining the reduction, temporary fixation is achieved with a 1.2mm or 1.6mm Kirschner wire driven from dorsal-proximal to plantar-distal, capturing the capital fragment.
Fluoroscopy is utilized at this stage to confirm the amount of shortening, the trajectory of the K-wire, and the realignment of the MTP joint.

Definitive fixation is typically achieved with one or two twist-off (snap-off) screws or standard cortical screws (2.0mm or 2.5mm).

The screw is inserted over the K-wire (if cannulated) or adjacent to it, ensuring bicortical purchase without violating the plantar articular surface.

Following secure fixation, the overhanging dorsal lip of the proximal diaphyseal fragment is meticulously resected with a rongeur or the sagittal saw to prevent dorsal impingement and mechanical irritation of the extensor tendons.

The final steps involve soft tissue balancing. The EDL tendon, previously Z-cut, is repaired in its newly lengthened position using a 3-0 or 4-0 non-absorbable suture.

The tension should be set such that the toe rests in neutral alignment with the ankle at 90 degrees.

If a concurrent plantar plate repair is indicated, it is performed prior to the final fixation of the osteotomy, utilizing the exposure provided by the mobile capital fragment. The skin is closed with a running or interrupted non-absorbable suture, and a compressive forefoot dressing is applied.
Complications, Incidence Rates, and Salvage Management
Despite its biomechanical elegance, the Weil osteotomy is not without complications. The surgeon must be acutely aware of these potential pitfalls, their incidence, and the appropriate salvage strategies. The most notorious and frequently discussed complication is the "floating toe" deformity.
| Complication | Estimated Incidence | Etiology & Prevention | Salvage Management |
|---|---|---|---|
| Floating Toe | 15% - 30% | Etiology: Proximal translation of the head moves the axis of rotation proximally, slackening the intrinsic muscles (lumbricals/interossei) which lose their plantarflexion moment. Prevention: Limit shortening (<5mm if possible), concurrent flexor-to-extensor transfer (Girdlestone-Taylor), aggressive post-op plantarflexion taping. | Flexor digitorum longus (FDL) to extensor tendon transfer; PIP joint arthrodesis to convert the toe into a rigid lever. |
| Transfer Metatarsalgia | 5% - 15% | Etiology: Over-shortening of the operated metatarsal, or failure to address a hypermobile first ray, shifting load to adjacent rays. Prevention: Meticulous pre-op templating; concurrent first ray stabilization. | Orthotic offloading; subsequent Weil osteotomy of the newly symptomatic adjacent metatarsal. |
| Nonunion / Delayed Union | 1% - 3% | Etiology: Poor bone stock, thermal necrosis from the saw blade, inadequate fixation, smoking. Prevention: Copious irrigation during saw use, rigid bi-cortical screw fixation. | Prolonged immobilization, bone stimulator, revision with bone grafting and plate fixation. |
| Avascular Necrosis (AVN) | < 2% | Etiology: Excessive stripping of the plantar and lateral capsular attachments, destroying the vascular supply to the metatarsal head. Prevention: Strict adherence to dorsal dissection only. | Conservative management (often asymptomatic); late-stage collapse may require excisional arthroplasty or interpositional grafting. |
| Hardware Irritation | 5% - 10% | Etiology: Prominent screw heads, especially if the dorsal overhanging bone was not adequately resected. Prevention: Countersinking screws, thorough resection of the dorsal bony lip. | Simple hardware removal under local anesthesia once radiographic union is confirmed (typically > 3 months). |
The floating toe warrants deeper discussion. When the metatarsal head is shifted proximally, the distance between the origin and insertion of the intrinsic muscles decreases. Because these muscles normally pass plantar to the MTP joint axis to flex the toe, this slackening reduces their mechanical advantage. Furthermore, the proximal shift of the bony architecture effectively moves the center of rotation proximally. If the intrinsic tendons do not adapt, their line of pull can migrate dorsal to the new axis of rotation, turning them into paradoxical extensors. To mitigate this, many surgeons routinely perform a concurrent Flexor Digitorum Longus (FDL) to extensor hood transfer to actively pull the toe plantarly, or they utilize a modified Weil technique (taking a parallel slice of bone to shorten without translating the axis).
Stiffness of the MTP joint is another nearly universal, though often mild, complication. Some degree of restricted
