Wrist Denervation: An Intraoperative Masterclass for Chronic Wrist Pain Relief

Key Takeaway
Join us in the OR for a comprehensive wrist denervation masterclass. This guide covers patient selection, detailed anatomy, precise intraoperative techniques for partial and full denervation, critical pearls to avoid pitfalls, and essential postoperative management strategies for effective chronic wrist pain relief.
Comprehensive Introduction and Patho-Epidemiology
Wrist denervation is a highly nuanced, joint-preserving surgical intervention designed to palliate chronic wrist pain while meticulously maintaining the patient's existing range of motion and grip strength. In the academic setting, we frequently encounter patients suffering from recalcitrant wrist arthrosis—often secondary to Scapholunate Advanced Collapse (SLAC), Scaphoid Nonunion Advanced Collapse (SNAC), Kienböck's disease, or primary radiocarpal osteoarthritis. These patients typically present with substantial pain-related disability, yet they possess a functional, albeit degenerative, arc of motion that they are desperate to preserve.
The fundamental philosophy of wrist denervation rests on the targeted interruption of the afferent nociceptive pathways originating from the radiocarpal, midcarpal, and distal radioulnar joints. Historically pioneered by Wilhelm in the 1960s as a complete denervation involving extensive dissection, the procedure has evolved significantly. Modern orthopedic practice heavily favors a more focused, partial denervation—most commonly targeting the Posterior Interosseous Nerve (PIN) and the Anterior Interosseous Nerve (AIN). This evolution reflects a deeper understanding of carpal innervation patterns and a desire to minimize surgical morbidity while maximizing analgesic efficacy.
It is imperative to understand that denervation does not alter the underlying structural pathology or halt the progression of arthrosis. Instead, it acts as a highly effective palliative measure. By surgically dividing the specific articular nerve branches transmitting noxious signals, we effectively disconnect the "alarm system" of the degenerating joint. This allows patients to utilize their remaining mechanical function without the profound inhibition of pain. When executed with precision, wrist denervation serves as a critical bridge or an alternative to motion-sacrificing salvage procedures such as proximal row carpectomy (PRC) or partial/total wrist arthrodesis.
Epidemiologically, the ideal candidate is typically a middle-aged, high-demand patient—often a manual laborer or active individual—who cannot afford the functional limitations imposed by a wrist fusion. The success of this procedure is highly dependent on meticulous patient selection, comprehensive preoperative diagnostic blockades, and a profound, three-dimensional understanding of the neurovascular anatomy of the forearm and wrist.
Detailed Surgical Anatomy and Biomechanics
The wrist joint is innervated by a complex, redundant network of articular branches derived from the major peripheral nerves of the upper extremity. A masterful execution of wrist denervation requires an intimate knowledge of these pathways, their anatomical landmarks, and their relationships to adjacent neurovascular and tendinous structures.
The Posterior Interosseous Nerve (PIN)
The PIN is arguably the most significant contributor to nociception in the dorsal wrist capsule. As the terminal motor branch of the radial nerve, it courses through the supinator muscle, emerging into the posterior compartment of the forearm. It travels distally along the interosseous membrane, accompanied by the posterior interosseous artery and veins.

At the level of the distal radioulnar joint (DRUJ), the PIN lies strictly on the radial floor of the fourth extensor compartment, deep to the extensor digitorum communis (EDC) and extensor indicis proprius (EIP) tendons. Its terminal branches arborize extensively to innervate the dorsal radiocarpal and intercarpal ligaments. Recognizing its precise location on the interosseous membrane is critical for isolation and excision.
The Anterior Interosseous Nerve (AIN)
The AIN, the terminal motor branch of the median nerve, is the primary sensory supply to the volar wrist capsule. It descends along the anterior surface of the interosseous membrane, situated between the flexor pollicis longus (FPL) and the flexor digitorum profundus (FDP). Distally, it passes deep to the pronator quadratus muscle. Its terminal articular branches innervate the volar radiocarpal ligaments, the scaphoid, and the lunate. The AIN can be accessed either via a dedicated volar approach or, more elegantly in a partial denervation, through a window in the interosseous membrane from a dorsal approach.
Superficial Radial and Ulnar Articular Branches
Beyond the deep interosseous nerves, the superficial sensory nerves also contribute articular branches. The dorsal articular branches of the radial nerve provide sensation to the dorsoradial aspect of the wrist, particularly around the radial styloid and scaphoid.

Conversely, the dorsal cutaneous branch of the ulnar nerve courses dorsally to supply the dorsal-ulnar wrist capsule and the DRUJ.

Additionally, the palmar branch of the median nerve and the recurrent intermetacarpal nerve branches provide supplementary innervation to the volar wrist and carpometacarpal joints, respectively. Total wrist denervation necessitates the systematic identification and transection of all these accessory branches, whereas partial denervation focuses strictly on the PIN and AIN.
Exhaustive Indications and Contraindications
Patient selection is the absolute cornerstone of a successful wrist denervation. The procedure is not a panacea for all wrist pain; rather, it is a highly specific tool for a specific clinical scenario. The ideal patient demonstrates significant pain due to structural arthrosis but retains a functional, albeit potentially limited, range of motion that they wish to preserve.
Patient Selection Criteria
We meticulously evaluate patients presenting with SLAC or SNAC wrists (typically stages I or II, and carefully selected stage III), localized radiocarpal arthrosis, or isolated DRUJ arthritis. Crucially, the wrist must be mechanically stable. Denervation in the presence of frank carpal instability will fail, as the abnormal kinematics will continue to generate pain and accelerate catastrophic joint destruction. Furthermore, diagnostic local anesthetic blocks must yield a profound reduction in pain (typically >75-80% relief) and a measurable increase in grip strength to justify surgical intervention.
Table of Indications and Contraindications
| Category | Specific Conditions | Clinical Rationale |
|---|---|---|
| Primary Indications | SLAC/SNAC Wrist (Stages I-II), Kienböck's Disease, Primary Radiocarpal OA | Pain relief desired while preserving functional motion; failure of conservative management. |
| Secondary Indications | Post-traumatic wrist pain, isolated DRUJ arthrosis | Targeted denervation (e.g., PIN only) can provide excellent localized relief. |
| Absolute Contraindications | Active joint infection, Frank carpal instability (e.g., dynamic SL dissociation) | Denervation masks progressive destruction; instability requires structural stabilization. |
| Relative Contraindications | Inflammatory Arthritis (Rheumatoid), Chronic Regional Pain Syndrome (CRPS) | Pain is systemic/neuropathic rather than purely mechanical/articular; poor surgical outcomes. |
| Clinical Prerequisites | Negative response to diagnostic blocks | If blocks do not relieve pain, surgical denervation will not be effective. |
Pre-Operative Planning, Templating, and Patient Positioning
Comprehensive preoperative planning transforms a technically sound surgery into a clinically successful outcome. This phase relies heavily on advanced physical examination and the strategic use of diagnostic local anesthetic blocks.
Diagnostic Local Anesthetic Blocks
The diagnostic block is not merely an assessment tool; it is a predictive therapeutic trial. We utilize 0.5% bupivacaine without epinephrine to selectively numb the articular branches.

The protocol is executed systematically:
1. PIN Block: 1 mL injected 1 cm ulnar and 3 cm proximal to Lister's tubercle, deep to the extensor fascia.
2. AIN Block: Advancing the needle through the interosseous membrane from the PIN site, injecting 1 mL volarly.
3. Radial/Ulnar Branches: Subcutaneous injections targeting the dorsal radial and dorsal ulnar sensory branches.
Following the injections, the patient is observed for 20 to 30 minutes. We require objective data: a visual analog scale (VAS) pain reduction of at least 80% and a demonstrable improvement in grip strength using a Jamar dynamometer. A positive block confirms that the patient's pain is mediated by these specific neural pathways, making them an excellent candidate for surgical neurectomy.
Intraoperative Setup and Equipment
The patient is positioned supine with the operative extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mmHg (or 100 mmHg above systolic pressure) following exsanguination with an Esmarch bandage. A bloodless field is non-negotiable, as the articular nerve branches are minute and easily obscured by minor hemorrhage.
Loupe magnification is absolutely mandatory. We strongly recommend 2.5x to 4.5x magnification combined with a high-intensity fiber-optic headlight. The surgical tray must include fine plastic surgery instruments: tenotomy scissors, delicate mosquito hemostats, fine-toothed forceps, and nerve hooks. Bipolar electrocautery is utilized exclusively to prevent collateral thermal injury to adjacent tendons and major nerve trunks.
Step-by-Step Surgical Approach and Denervation Technique
The surgical execution demands meticulous dissection. We will detail both the partial denervation (targeting the PIN and AIN) and the comprehensive total wrist denervation. The fundamental principle for every nerve branch encountered is to identify it, isolate it, resect a minimum 1-centimeter segment, and bury or coagulate the proximal stump to prevent painful neuroma formation.
Partial Denervation Targeting the PIN and AIN
Step 1: The Dorsal Approach
A 3-cm longitudinal or transverse incision is made over the dorsal aspect of the distal forearm, centered approximately 3 to 4 cm proximal to the radiocarpal joint line. This proximal placement ensures the PIN is captured before it arborizes into multiple terminal filaments.
Blunt dissection is carried through the subcutaneous tissues, carefully retracting any superficial sensory branches of the radial nerve. The extensor retinaculum is identified, and the fourth extensor compartment is opened longitudinally.
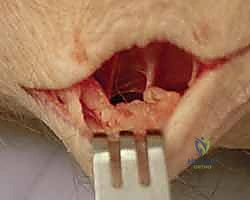
Step 2: Isolation of the PIN
The tendons of the EDC and EIP are retracted ulnarward. The radial floor of the fourth compartment is now exposed. The PIN is identified lying directly on the interosseous membrane, invariably accompanied by the posterior interosseous artery.

Using a fine nerve hook, the PIN is gently separated from the vascular bundle. It appears as a distinct, white, thread-like structure. A 1-cm to 1.5-cm segment of the nerve is sharply excised. The proximal stump is gently cauterized with bipolar forceps and allowed to retract proximally into the deep muscular fascia to minimize neuroma risk.
Step 3: Trans-osseous Approach to the AIN
While the AIN can be accessed volarly, an elegant technique involves accessing it through the dorsal incision. A small, 1-cm longitudinal window is sharply created in the interosseous membrane, taking extreme care not to plunge and injure the volar structures.
By gently retracting the volar musculature (pronator quadratus) through this window, the AIN can be visualized resting on the volar aspect of the interosseous membrane. It is isolated, and a 1-cm segment is resected in the same manner as the PIN.
Comprehensive Total Wrist Denervation
For patients requiring total denervation, the procedure is expanded to include multiple supplementary incisions to capture the remaining articular branches.
Step 4: Radial and Ulnar Articular Branches
To address the superficial radial nerve articular branches, a separate incision is made over the first and second extensor compartments.

The sensory branches are carefully preserved, but the deep articular twigs diving toward the scaphoid and radial styloid are identified and transected. Similarly, an incision over the distal ulna allows for the identification of the dorsal cutaneous branch of the ulnar nerve.

The articular branches diving into the DRUJ and ulnocarpal joint are meticulously isolated and resected.
Step 5: Palmar and Intermetacarpal Branches
Volar innervation is addressed via a palmar incision proximal to the wrist crease, identifying the palmar cutaneous branch of the median nerve. Its deep articular branches are sacrificed while preserving the main sensory trunk.

Finally, small incisions over the bases of the second and third metacarpals allow for the identification and excision of the recurrent intermetacarpal nerve branches. Once all targeted nerves are resected, the tourniquet is deflated, meticulous hemostasis is achieved, and the wounds are closed in layers.
Complications, Incidence Rates, and Salvage Management
While wrist denervation is generally considered a low-morbidity, joint-preserving procedure, it is not without potential complications. The surgeon must be acutely aware of these risks and possess the armamentarium to manage them effectively.
Neuroma and Incomplete Denervation
The most common cause of surgical failure is incomplete denervation, resulting from missed anomalous branches or failure to resect a sufficient length of the nerve. Patients will present with persistent pain identical to their preoperative state. Conversely, symptomatic neuroma formation at the transection site presents as a new, sharp, neuropathic pain with a positive Tinel's sign over the surgical incision.
Another theoretical complication often discussed in the literature is Charcot arthropathy (neuropathic joint destruction) due to the loss of proprioception. However, extensive long-term follow-up studies have demonstrated that clinically significant Charcot arthropathy following wrist denervation is exceedingly rare, likely due to the preservation of profound capsular and ligamentous mechanoreceptors not addressed by the targeted neurectomies.
Table of Complications and Management Strategies
| Complication | Estimated Incidence | Etiology / Pathophysiology | Salvage Management / Prevention |
|---|---|---|---|
| Incomplete Pain Relief | 15% - 25% | Missed articular branches, advanced unaddressed arthrosis, misdiagnosis. | Re-evaluation; progression to salvage procedures (PRC, Arthrodesis). |
| Symptomatic Neuroma | 2% - 5% | Failure to bury proximal nerve stump; superficial nerve injury during approach. | Surgical exploration, neuroma excision, and burying the stump into deep muscle belly. |
| Superficial Dysesthesia | 5% - 10% | Iatrogenic traction or thermal injury to superficial radial/ulnar sensory nerves. | Usually transient; managed with gabapentinoids, desensitization therapy. |
| Wound Healing Issues | < 2% | Standard surgical site infection, hematoma formation. | Meticulous hemostasis post-tourniquet deflation; standard antibiotic protocols. |
| Charcot Arthropathy | < 1% | Theoretical loss of joint proprioception leading to accelerated destruction. | Extremely rare in practice; requires conversion to total wrist arthrodesis if it occurs. |
Phased Post-Operative Rehabilitation Protocols
Because wrist denervation does not alter the structural integrity of the carpus, divide ligaments, or require osseous healing, the postoperative rehabilitation protocol is remarkably accelerated compared to other wrist reconstructive procedures. The primary goals are edema control, prevention of stiffness, and rapid restoration of preoperative function.
Immediate Post-Operative Phase (Days 1-14)
The patient is placed in a bulky, soft compressive dressing with a volar plaster splint for comfort immediately post-surgery. The splint is typically removed within 3 to 5 days. We strongly encourage immediate, active range of motion (ROM) of the digits, elbow, and shoulder to prevent generalized upper extremity stiffness and promote venous return. Once the splint is removed, gentle active and active-assisted ROM of the wrist is initiated. Pain is usually well-controlled with oral analgesics, and patients often note an immediate absence of their deep, preoperative arthritic pain.
Intermediate and Advanced Rehabilitation (Weeks 2-6)
Sutures are removed at 10 to 14 days. At this stage, patients are transitioned to a removable thermoplastic wrist splint, worn primarily for heavy activities or sleep. Formal occupational therapy is highly beneficial. Therapists focus on scar massage and desensitization techniques to prevent superficial dysesthesias. Progressive strengthening exercises, focusing on grip and pinch strength, are introduced at week 3. Because the mechanical block of pain has been removed, patients often achieve grip strengths that significantly exceed their preoperative baselines. Unrestricted activity and return to manual labor are typically permitted by 6 to 8 weeks postoperatively, guided by the patient's comfort and functional recovery.
Summary of Landmark Literature and Clinical Guidelines
The academic foundation of wrist denervation is built upon decades of anatomical and clinical research. Wilhelm's landmark 1966 publication introduced the concept of total wrist denervation, mapping the complex articular branches. However, the extensive dissection required often led to unacceptable rates of scar formation and superficial nerve injury.
Historical Context and Evolving Paradigms
The paradigm shifted significantly in the late 1990s and early 2000s. Berger (1998) and later Weinstein and colleagues demonstrated that partial denervation, specifically targeting the PIN and AIN, provided pain relief statistically comparable to total denervation but with a fraction of the surgical morbidity.
Modern systematic reviews and meta-analyses consistently report that 70% to 85% of properly selected patients achieve satisfactory pain relief following partial wrist denervation. Furthermore, long-term studies indicate that the analgesic effect is durable, often lasting 5 to 10 years, thereby significantly delaying or entirely avoiding the need for salvage procedures like complete wrist arthrodesis. Clinical guidelines now firmly establish partial wrist denervation as a first-line surgical option for mechanically stable, painful wrist arthrosis that has failed conservative management, provided the patient demonstrates a positive response to preoperative diagnostic blocks.
