Management of Digital Nerve Injuries and Interfascicular Grafting
Key Takeaway
Digital nerve injuries require meticulous microsurgical repair to restore hand sensation and function. Critical repairs include the thumb ulnar digital nerve and index radial digital nerve. When primary tension-free coaptation is impossible, interfascicular nerve grafting using the Millesi step-cut technique is indicated. Successful outcomes depend on precise fascicular mapping, tension-free coaptation in a well-vascularized bed, and a structured postoperative rehabilitation protocol monitoring the advancing Tinel sign.
Comprehensive Introduction and Patho-Epidemiology
Distal to the radiocarpal joint, the digital nerves represent the most frequently lacerated, crushed, or avulsed peripheral nervous structures within the upper extremity. The restoration of protective and tactile sensation is absolutely paramount for optimal hand function, fine motor dexterity, and the prevention of inadvertent thermal, chemical, or mechanical injury. A completely insensate digit is often functionally bypassed by the patient, rendering even a biomechanically intact finger virtually useless in complex prehensile tasks. While the prevailing microsurgical dogma dictates that all digital nerve lacerations warrant rigorous evaluation for primary or secondary repair, it is critically important for the operating surgeon to prioritize the repair of specific nerves that govern primary pinch, power grip, and spatial proprioception.
The epidemiological profile of digital nerve injuries skews heavily toward young, active, and working-age populations, predominantly males between the ages of 18 and 40. Industrial accidents involving table saws, high-pressure injection equipment, and heavy crush machinery account for a significant proportion of complex, multi-tissue injuries. Conversely, domestic incidents—such as kitchen knife slips or broken glass lacerations—typically present as sharp, clean transections. The mechanism of injury directly dictates the zone of trauma; a sharp glass laceration may result in a sub-millimeter zone of injury, whereas an avulsion or severe crush injury can induce intraneural fibrosis and Wallerian degeneration extending several centimeters proximal and distal to the visible macroscopic lesion.
From a pathophysiological standpoint, the moment a digital nerve is transected, a highly orchestrated cascade of cellular events is initiated. Distal to the laceration, the axon and its myelin sheath undergo Wallerian degeneration, a process characterized by axonal fragmentation and subsequent phagocytosis by invading macrophages and resident Schwann cells. These proliferating Schwann cells then align longitudinally to form the bands of Büngner, which serve as the biological conduits for future regenerating axonal sprouts. Proximal to the injury, the neuron's cell body undergoes chromatolysis, upregulating the synthesis of structural proteins required for axonal elongation. If the gap between the proximal and distal stumps is too large, or if the local environment is intensely fibrotic, the advancing axonal cone will fail to cross the defect, resulting in a disorganized, painful tangle of axons and connective tissue known as a terminal neuroma.
Given the finite regenerative capacity of peripheral nerves, prioritization of repair is essential in multi-level or devastating hand injuries. The most functionally vital digital nerves include the ulnar digital nerve of the thumb (essential for key pinch and opposition), the radial digital nerve to the index finger (critical for pulp-to-pulp pinch and fine manipulation), the radial digital nerves to the long and ring fingers (important for power grip and spatial orientation), and the ulnar digital nerve to the little finger (crucial for the ulnar border of the hand during power grip and resting on surfaces). Furthermore, a comprehensive knowledge of the anatomy of the cutaneous sensory branches of the nerves on the dorsum of the hand allows for the meticulous repair of these dorsal branches, which, while often overlooked historically, contribute significantly to overall hand proprioception and sensory feedback.
Detailed Surgical Anatomy and Biomechanics
The topographical and micro-surgical anatomy of the digital nerves must be intimately understood to facilitate successful exploration, mobilization, and interfascicular grafting. Digital nerves can be reliably repaired distal to the distal volar flexion crease of the fingers, extending well into the region of the terminal arborizations. As the common digital nerves bifurcate in the distal palm, they travel distally as proper digital nerves, situated volar to the digital arteries within the neurovascular bundle. This bundle is securely tethered and protected by a complex fascial network, notably Cleland’s ligaments (situated dorsal to the neurovascular bundle) and Grayson’s ligaments (situated volar to the bundle). These fascial septa not only stabilize the skin during prehension but also dictate the extent of nerve retraction following a complete transection.
On a microscopic level, the peripheral nerve is a highly organized, hierarchical structure. The outermost layer, the epineurium, provides mechanical support and houses the vital longitudinal vascular plexus (vasa nervorum). Beneath the epineurium lies the perineurium, a dense, metabolically active layer of specialized cells that maintains the blood-nerve barrier and encases individual fascicles. Finally, the endoneurium surrounds individual axons within the fascicle. As the digital nerves progress distally from the palm to the fingertip, their internal architecture transitions from a polyfascicular arrangement (multiple small fascicles) to an oligofascicular or even monofascicular pattern. Recognizing this topographical shift is critical when performing a repair, as a polyfascicular proximal stump may need to be coapted to a monofascicular distal stump, requiring meticulous group fascicular matching.
Biomechanically, peripheral nerves are not static cables; they possess an inherent elasticity and tensile strength primarily derived from the undulating, accordion-like arrangement of the endoneurial tubes and axons, known as the bands of Fontana. This elasticity allows the nerve to accommodate the extreme ranges of motion of the metacarpophalangeal and interphalangeal joints without sustaining traction injuries. However, this same biomechanical property becomes a formidable obstacle following transection. When a nerve is severed, the proximal and distal stumps immediately retract due to this inherent elasticity, compounded by surrounding tissue edema and muscle contraction (if proximal to the motor branches).
Tension at the repair site is universally recognized as the primary enemy of nerve regeneration. Tension mechanically compromises the delicate microvascular supply within the mesoneurium and epineurium, leading to profound ischemia at the coaptation site. This ischemic environment stimulates excessive fibroblast proliferation, resulting in a dense, impermeable scar that mechanically blocks axonal sprouting. If a primary repair cannot be achieved without tension—typically defined as requiring larger than an 8-0 suture to hold the stumps together, or any tension that causes the fascicles to buckle—an interfascicular nerve graft is strictly and unequivocally indicated to bridge the defect.
Exhaustive Indications and Contraindications
The decision-making algorithm for the management of digital nerve injuries hinges on the timing of presentation, the mechanism of injury, the condition of the soft tissue envelope, and the overall physiological status of the patient. Primary repair, performed within the first 48 to 72 hours, remains the gold standard for sharp, clean lacerations with minimal crush component. In this acute window, the nerve ends have not yet undergone maximal retraction, and the intraneural architecture remains clearly identifiable, facilitating anatomical fascicular alignment. However, in cases of severe crush injuries, extensive avulsions, or highly contaminated agricultural or industrial wounds, a delayed primary (within 2 weeks) or secondary repair (after 2 weeks) is strictly indicated to allow for tissue demarcation and aggressive serial debridement.
If digital nerves are to be repaired secondarily or via interfascicular grafting, the surgical environment must be meticulously optimized. The proposed suture line must lie in a well-vascularized bed completely free of fibrotic scar tissue. Placing a delicate nerve repair or a non-vascularized autograft into a scarred, avascular bed will inevitably result in catastrophic failure due to ischemic necrosis of the advancing axonal sprouts. In such complex reconstructive scenarios, the surgeon must first address the soft tissue deficit, often requiring local rotational flaps, regional flaps (e.g., cross-finger flaps), or even free tissue transfer to provide a robust, nutrient-rich envelope for the subsequent nerve graft.
Contraindications to digital nerve repair or grafting must be carefully weighed against the functional demands of the patient. Absolute contraindications include life-threatening polytrauma where prolonged microscopic upper extremity surgery would compromise patient survival, severe active purulent infection at the injury site, and a completely avascular digit requiring amputation. Relative contraindications encompass severe physiological non-compliance, profound cognitive impairment precluding participation in mandatory post-operative sensory re-education, and advanced peripheral microvascular disease (such as severe diabetic neuropathy or end-stage Buerger's disease) where the regenerative capacity of the peripheral nervous system is fundamentally extinguished.
| Parameter | Indications for Repair/Grafting | Contraindications (Absolute/Relative) |
|---|---|---|
| Timing & Mechanism | Sharp lacerations (Primary); Demarcated crush/avulsion (Delayed/Secondary); Gap > 1cm (Grafting). | Un-demarcated severe crush (Relative); Active purulent infection (Absolute). |
| Soft Tissue Envelope | Well-vascularized bed; Adequate skin coverage available (local or flap). | Dense avascular scar bed without flap option (Absolute); Exposed bone/tendon without coverage (Absolute). |
| Patient Factors | High functional demand; Intact cognitive status; Compliant with rehab. | Severe advanced diabetic neuropathy (Relative); Non-compliant/psychiatric instability (Relative). |
| Anatomical Level | Proximal to distal interphalangeal joint; Critical pinch/grip digits. | Distal to the nail matrix where arborization precludes technical repair (Relative). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of successful microsurgical nerve reconstruction. In the acute setting, the diagnosis of a digital nerve laceration is clinical, relying heavily on static and moving two-point discrimination testing, as well as Semmes-Weinstein monofilament evaluation. However, in the delayed or secondary setting, the proximal nerve stump will have inevitably formed a terminal neuroma. Locating this stump amidst dense, unyielding scar tissue intraoperatively can be a frustrating and tissue-destructive endeavor if not planned appropriately.
Before secondary repair or grafting, the proximal end of the nerve can often be localized clinically in the outpatient setting. By passing a firm, blunt object—such as a paper clip or the wooden end of a cotton swab—gently and distally along the anatomical course of the nerve, the surgeon can map the nerve's progression. Upon reaching the terminal neuroma, the patient will indicate exquisite, electrifying tenderness, representing a localized Tinel's sign. This precise mapping guides the proximal extent of the surgical incision and dictates the anticipated length of the nerve graft required, allowing the surgeon to select the most appropriate donor site (e.g., medial antebrachial cutaneous nerve, lateral antebrachial cutaneous nerve, or sural nerve) well before the patient enters the operating theater.
Patient positioning and operating room ergonomics are critical for minimizing surgeon fatigue and maximizing microsurgical precision. The patient is positioned supine with the operative arm extended on a rigid, radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mmHg (or 100 mmHg above systolic pressure) after exsanguination to provide a bloodless surgical field. The surgeon and assistant should be seated comfortably opposite each other, with the operating microscope (or high-powered 4.5x to 6.0x loupes) positioned directly over the surgical field. Forearm support for the surgeon is non-negotiable to eliminate physiologic tremor during the placement of 10-0 or 11-0 sutures.
The microsurgical armamentarium must be prepared and inspected prior to the first incision. This includes jeweler's forceps (typically #5), non-toothed micro-adson forceps, curved and straight microscissors (such as Westcott or Vannas scissors), and specialized nerve-holding clamps. A sterile background material—often a small piece of blue or green silicone—is essential to place behind the nerve stumps, enhancing visual contrast and preventing the delicate translucent fascicles from blending into the underlying hemorrhagic soft tissue. Fibrin glue may also be prepared on the back table as an adjunct to suture coaptation, particularly in multi-cable interfascicular grafting where minimizing the volume of foreign body (suture material) is desired.
Step-by-Step Surgical Approach and Fixation Technique
Exposure and Neuroma Resection
The surgical approach to the injured digital nerve must provide extensile exposure while respecting the biomechanics of the digit. The surgeon should utilize a Bruner zig-zag volar incision or a mid-axial incision to expose the neurovascular bundle. It is a cardinal rule of hand surgery to never cross volar flexion creases perpendicularly, as this will inevitably lead to devastating longitudinal scar contractures and secondary joint stiffness. The incision should be generous, allowing the surgeon to identify the nerve in pristine, virgin tissue both proximal and distal to the central zone of injury. Once identified in healthy tissue, the nerve ends are meticulously traced toward the central zone of scarring, utilizing loop magnification.
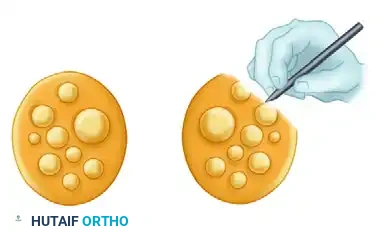
Upon reaching the zone of injury, the terminal neuroma on the proximal stump and the corresponding glioma on the distal stump must be radically resected back to healthy, viable fascicles. This is arguably the most critical step of the procedure; inadequate resection is the leading cause of graft failure.

The image above illustrates the classic appearance of a neuroma-in-continuity or a severely scarred nerve segment prior to resection. The thickened, fibrotic epineurium and disorganized internal architecture must be completely excised. Using a fresh, ultra-sharp surgical blade (such as a #11 or a specialized diamond micro-knife) against a sterile wooden tongue depressor, the surgeon must "bread-loaf" the nerve ends. This involves making sequential 1-mm transverse cuts until healthy, glistening fascicles "mushroom" or pout out of the epineurium. This pouting indicates normal endoneurial pressure and viable, healthy tissue capable of supporting axonal regeneration.
Fascicular Mapping and Preparation
In polyfascicular nerves, such as the median and ulnar nerves at the wrist, or even the more proximal common digital nerves in the palm, appropriate alignment of sensory and motor fascicles (or specific sensory territories) is critical to prevent axonal misdirection. If a sensory axon regenerates down a motor endoneurial tube, that axon is functionally lost.
As shown in the illustration above, it is highly helpful to physically sketch the ends of the two nerve stumps with their respective fascicular patterns. The surgeon should use a sterile surgical marker and a piece of the sterile glove wrapper to draw the cross-section of the proximal and distal stumps. Map the fascicles based on their size, the number of fascicles, and their spatial arrangement within the stumps. Furthermore, utilize longitudinal epineurial blood vessels as critical landmarks to ensure rotational alignment. Clinical estimation of fascicular alignment is relatively straightforward over short distances but becomes exponentially more difficult over longer defects where the internal topography of the nerve naturally rotates and branches. Relying on intraoperative sketches allows for precise matching of the respective fascicles and appropriate placement of the graft cables.
The Millesi Step-Cut Interfascicular Technique
When a significant gap exists after adequate, aggressive debridement of the proximal and distal stumps, interfascicular nerve grafting is absolutely required. The step-cut technique, pioneered and popularized by Hanno Millesi, is highly recommended for polyfascicular nerves to maximize the surface area for coaptation and, crucially, to prevent the confluence of scar tissue across a single transverse plane.
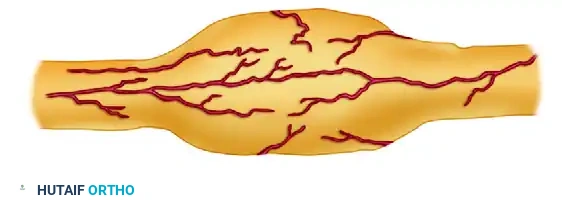
As demonstrated in the step-cut technique of Millesi (Figures A to C above):
* Step A: The epineurium is longitudinally incised and resected over a short distance (typically 5 to 10 mm) to expose the underlying fascicular groups.
* Step B: The fascicular groups are meticulously separated using interfascicular dissection with micro-scissors and jeweler's forceps, taking immense care not to disrupt the delicate perineurium.
* Step C: The fascicles are transected at different levels (staggered or "step-cut"). This ensures that the individual nerve grafts will protrude from the nerve stump at varying lengths after the completion of the interfascicular dissection.
The surgeon must carry out this similar staggered dissection on both the proximal and distal stumps. This staggering prevents a single, circumferential ring of restrictive scar tissue from forming at the coaptation site, which could otherwise constrict regenerating axons and lead to a mechanical block to recovery.
Nerve Grafting Principles and Coaptation
Donor site selection is dictated by the caliber of the injured nerve and the total length of the gap to be filled. For common and proper digital nerves, the medial or lateral antebrachial cutaneous nerves are highly satisfactory. They offer an excellent caliber match for digital nerves and result in a relatively inconspicuous area of donor site numbness that patients tolerate well. If a massive amount of nerve tissue is required (e.g., multiple digital nerves or a large gap in a major mixed nerve), the sural nerve remains the undisputed gold standard. It provides up to 30-40 cm of robust graft material and can be cut into multiple cables to match the cross-sectional area of the recipient nerve.
After the nerve graft has been harvested, it is imperative to reverse its orientation (i.e., suturing the distal end of the graft to the proximal nerve stump). This reversed orientation minimizes axonal loss through any small, unnoticed cutaneous branches within the graft; if placed in the native orientation, regenerating axons could migrate down these dead-end branches and be lost to the distal target. The graft is then placed gently between the proximal and distal nerve stumps. In polyfascicular nerves, the surgeon uses the intraoperative sketch to allow appropriate, topographically matched placement of the graft cables.
When coaptation of the graft is initiated, the surgeon utilizes 10-0 or 11-0 monofilament nylon on a micro-spatula needle. The needle should pass superficially through the epineurium of the graft and the perineurium of one of the fascicles in the group, or into the interfascicular connective tissue of the host stump. A strict "minimal suture technique" should be employed. Multiple sutures are rarely required and are often detrimental. If the bed is well-prepared, the graft is perfectly sized, and there is zero tension, 2 to 3 sutures per coaptation site are entirely sufficient. Excessive suturing introduces unnecessary foreign body reactions, localized inflammation, and scarring. The natural fibrin clot that forms within the surgical field will provide significant adhesive tensile strength within minutes of tourniquet deflation.
Wound Closure and Drainage
Meticulous hemostasis is mandatory before closure to prevent hematoma formation. A hematoma acts as a physical barrier to axonal regeneration, a potent stimulator of fibrosis, and a rich nidus for deep space infection. The tourniquet must be deflated, and all pinpoint bleeding controlled with bipolar micro-cautery, taking extreme care to keep the thermal energy far away from the newly coapted nerve grafts.
If dead space is a concern, small passive Silastic drains may be inserted to prevent fluid accumulation. However, there is a strict warning in microsurgical nerve repair: Avoid the use of active suction drainage. Active suction can easily displace the delicate nerve grafts, suck the graft into the drain fenestrations, or violently disrupt the tenuous 10-0 nylon coaptations. The skin is closed carefully with non-absorbable monofilament sutures. The surgeon must visually confirm that the graft is not displaced, kinked, or subjected to shearing forces during wound closure. If skin closure causes any tension over the graft, a local rotational flap or a full-thickness skin graft must be utilized immediately to ensure a tension-free, well-vascularized envelope.
Complications, Incidence Rates, and Salvage Management
Despite meticulous microsurgical technique, digital nerve repair and interfascicular grafting are fraught with potential complications. The most dreaded complication is the failure of axonal regeneration, leading to a persistent insensate digit and the formation of a painful terminal neuroma. Neuroma formation occurs in approximately 3% to 5% of primary repairs but can skyrocket to over 15% in secondary grafting procedures placed in sub-optimal, scarred beds. A symptomatic neuroma presents as exquisite point tenderness, a strongly positive Tinel's sign at the site of arrest, and severe cold intolerance.
Graft failure can occur due to tension, ischemia, infection, or inadequate resection of the initial zone of injury. Monitoring the advancing Tinel's sign is the clinical barometer of success. If the Tinel's sign arrests at the distal coaptation site for more than 3 to 4 months, graft failure must be suspected. Another profound complication is Complex Regional Pain Syndrome (CRPS), which can occur in up to 10% of peripheral nerve injuries of the upper extremity. CRPS is characterized by severe hyperalgesia, allodynia, sudomotor changes, and trophic skin alterations.
Salvage management requires a highly customized approach. For painful neuromas that have failed conservative management (desensitization therapy, gabapentinoids, targeted steroid injections), surgical excision is mandated. The neuroma is resected, and the nerve end can be managed via several techniques: burying the stump deep into healthy muscle or bone, capping the nerve end with a synthetic conduit, or utilizing Targeted Muscle Reinnervation (TMR) to provide the regenerating axons with a physiological target. For graft failures, re-exploration, excision of the fibrotic coaptation, and revision grafting with a fresh autograft or a processed nerve allograft is required.
| Complication | Estimated Incidence | Clinical Presentation | Salvage / Management Strategy |
|---|---|---|---|
| Symptomatic Neuroma | 5% - 15% | Exquisite point tenderness, positive Tinel's at arrest site, hyperalgesia. | Excision and burying into muscle/bone; Targeted Muscle Reinnervation (TMR); Capping. |
| Graft Failure / Non-union | 10% - 20% | Arrested Tinel's sign > 3-4 months at distal coaptation; persistent numbness. | Re-exploration, aggressive resection of scar, revision interfascicular grafting. |
| Complex Regional Pain Syndrome | 5% - 10% | Allodynia, sudomotor changes, trophic skin changes, joint stiffness. | Aggressive multidisciplinary therapy, Gabapentinoids, Sympathetic nerve blocks, Vitamin C prophylaxis. |
| Post-operative Hematoma | 2% - 4% | Acute swelling, throbbing pain, ecchymosis, wound dehiscence. | Immediate surgical evacuation, bipolar hemostasis, copious irrigation. |
Phased Post-Operative Rehabilitation Protocols
The success of a microsurgical nerve repair or graft relies just as heavily on strict adherence to a phased, scientifically grounded post-operative rehabilitation protocol as it does on the intraoperative technique. The rehabilitation is heavily dependent on the specialized skills of a certified hand therapist.
Phase I: Immobilization and Protection (Days 0 to 14)
Immediately post-operatively, the extremity is immobilized in a well-padded, custom-molded dorsal blocking splint. The primary goal of this phase is absolute protection of the tenuous micro-coaptations. The splint should hold the hand in as near an anatomical, tension-free position as possible. Typically, this involves slight wrist flexion (10-20 degrees), metacarpophalangeal (MCP) joints flexed to 30-45 degrees, and interphalangeal (IP) joints gently extended, depending entirely on the exact site of the graft and the joints it crosses. The part is strictly immobilized for about 10 to 14 days to allow the initial fibrin clot to organize into a robust cellular matrix and for early tensile strength to develop at the coaptation sites. During this phase, strict elevation is maintained to minimize edema. Hematomas that develop early in the post-operative period must be surgically evacuated immediately to prevent fibrotic scarring.
Phase II: Early Mobilization and Cortical Plasticity (Weeks 2 to 6)
At approximately 10 to 14 days, the splint is removed, sutures are extracted, and free movement of the joints is carefully initiated to prevent flexor tendon adhesions and joint capsular stiffness. Physical therapy is formally begun with supervised active and active-assisted range-of-motion exercises. It is critical to balance the need for tendon gliding with the protection of the nerve graft; extreme composite extension of the digit and wrist is avoided to prevent traction on the graft. Sensory re-education programs are initiated even before protective sensation returns. This early phase of sensory re-education focuses on maintaining cortical representation in the somatosensory cortex through visual-tactile integration, utilizing mirrors and contralateral hand stimulation to prevent cortical mapping degradation.
Phase III: Advanced Sensory Re-education and Monitoring (Weeks 6 and Beyond)
The progress of axonal regeneration is meticulously followed clinically using the advancing Tinel's sign. Axons typically regenerate at a rate of 1 mm per day (or roughly 1 inch per month) after an initial latency period of 3 to 4 weeks required for the axons to cross the proximal coaptation site. The surgeon must measure and document the most distal point of the Tinel's sign at each follow-up visit. Once protective sensation (typically perceived as a 30 Hz vibration or deep pressure) reaches the fingertip, Phase 2 sensory re-education begins. This involves moving touch, constant touch, and eventually complex object identification and stereognosis training. If the Tinel's sign stops advancing and shows no further progression for 3 to 4 months at the distal end of the graft, this indicates a failure of axons to cross the distal suture line, mandating surgical re-exploration.
Summary of Landmark Literature and Clinical Guidelines
The evolution of digital nerve repair and interfascicular grafting is deeply rooted in the landmark anatomical and clinical studies of the 20th century. Sir Sydney Sunderland’s exhaustive mapping of the internal topography of peripheral nerves laid the foundational understanding that nerves are not homogenous cables, but highly organized fascicular structures that require precise anatomical realignment. His classification of nerve injuries remains the definitive standard for understanding the pathophysiology of nerve trauma.
Hanno Millesi revolutionized the field of peripheral nerve reconstruction in the 1970s by challenging the then-prevailing dogma of repairing nerves under tension. Millesi’s landmark papers demonstrated unequivocally that tension at the repair site induces ischemia and massive intraneural fibrosis. He introduced the concept of the tension-free interfascicular nerve graft and the step-cut technique, proving that axons could more easily traverse two tension-free coaptation sites (a graft) than a single coaptation site under tension. This paradigm shift remains the bedrock of modern microsurgical nerve repair.
Contemporary clinical guidelines, supported by the American Society for Surgery of the Hand (ASSH) and recent meta-analyses, have further refined the indications for grafting versus alternative conduits. Current evidence suggests that for digital nerve gaps of less than 1.0 to 1.5 cm, synthetic nerve conduits (such as polyglycolic acid or collagen tubes) or processed nerve allografts yield sensory recovery rates comparable to autografts, while sparing the patient donor site morbidity. However, for critical nerve gaps exceeding 2.0 cm, or in heavily scarred and avascular beds, the non-vascularized autograft (sural or antebrachial
