Ulnar Nerve Reconstruction and Cubital Tunnel Syndrome: Advanced Surgical Management
Key Takeaway
Ulnar nerve reconstruction utilizing the anterior interosseous nerve (AIN) to ulnar motor branch transfer provides a reliable method for restoring intrinsic hand function. Concurrently, the management of cubital tunnel syndrome has evolved, favoring in situ decompression for primary cases, reserving anterior transposition for nerve subluxation or revision surgery. This guide details the surgical techniques, biomechanical principles, and postoperative protocols for optimizing ulnar nerve outcomes.
Comprehensive Introduction and Patho-Epidemiology
The ulnar nerve is structurally and functionally critical for the fine motor dexterity, grip strength, and intrinsic power of the human hand. It provides the terminal innervation to the hypothenar musculature, the interossei, the medial two lumbricals, and the adductor pollicis, thereby governing the complex biomechanics of pinch, grasp, and digital abduction/adduction. Injuries or chronic compressive neuropathies of the ulnar nerve present significant reconstructive challenges for the orthopedic surgeon. High ulnar nerve injuries—defined as those occurring proximal to the mid-forearm—are notorious for poor intrinsic muscle recovery. This is primarily due to the prolonged distance regenerating axons must travel. Growing at a rate of approximately 1 mm per day, regenerating axons often arrive at the distal targets only to find that irreversible motor endplate degradation, muscle fibrosis, and profound atrophy have occurred, precluding any meaningful functional recovery.
To address the dismal outcomes associated with proximal ulnar nerve neurotmesis, the paradigm of ulnar nerve reconstruction has experienced a monumental shift toward distal nerve transfers. These advanced microsurgical techniques bypass the proximal zone of injury entirely, providing a local, expendable source of high-density motor axons to reinnervate the intrinsic musculature before irreversible endplate collapse occurs. The transfer of the distal anterior interosseous nerve (AIN) to the deep motor branch of the ulnar nerve has become the gold standard in this reconstructive algorithm, fundamentally altering the prognostic landscape for severe upper extremity nerve trauma.
Concurrently, the management of chronic compressive neuropathies, predominantly cubital tunnel syndrome (CuTS) and tardy ulnar nerve palsy, has evolved significantly. Cubital tunnel syndrome represents the second most common compression neuropathy in the upper extremity, superseded only by carpal tunnel syndrome. Epidemiological data suggest an incidence of 25 to 30 cases per 100,000 person-years, with a higher prevalence in males and individuals engaged in occupations requiring repetitive elbow flexion or sustained direct pressure on the medial elbow. Tardy ulnar nerve palsy, a historical term often associated with delayed neuropathy following childhood lateral condyle fractures or progressive cubitus valgus deformities, shares a similar pathophysiological endpoint requiring meticulous evaluation.
The contemporary approach to these compressive pathologies places a growing emphasis on evidence-based, minimally invasive, and anatomically respectful surgical interventions. The historical reliance on routine anterior transposition has been challenged by robust prospective data supporting simple, in situ decompression for primary, uncomplicated cases. This evolution reflects a deeper understanding of intraneural microvascular hemodynamics, the deleterious effects of aggressive circumferential neurolysis, and the critical importance of preserving the extrinsic vascular supply to the nerve.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy and biomechanics of the ulnar nerve is the absolute prerequisite for both decompression and reconstructive procedures. The ulnar nerve originates from the medial cord of the brachial plexus, carrying fibers predominantly from the C8 and T1 nerve roots. It descends through the medial compartment of the arm, initially running medial to the brachial artery. At the level of the arcade of Struthers—a fascial hiatus in the medial intermuscular septum located approximately 8 cm proximal to the medial epicondyle—the nerve pierces the septum to enter the posterior compartment of the arm. This arcade is the most proximal potential site of compression and must be meticulously evaluated during any anterior transposition procedure to prevent secondary kinking of the nerve.
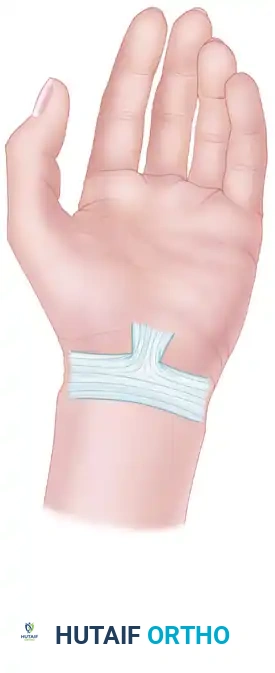
As the nerve progresses distally, it enters the retroepicondylar groove, bordered anteriorly by the medial epicondyle and laterally by the olecranon. The roof of this groove is formed by the cubital tunnel retinaculum, or Osborne’s ligament, which spans from the medial epicondyle to the tip of the olecranon. Distal to this, the nerve enters the true cubital tunnel, passing between the humeral and ulnar heads of the flexor carpi ulnaris (FCU). The deep flexor-pronator aponeurosis represents the most distal potential compression point in the elbow region. Further distally, the nerve travels through the forearm between the FCU and the flexor digitorum profundus (FDP), giving off motor branches to the FCU and the ulnar half of the FDP, before entering Guyon's canal at the wrist.
Biomechanically, the ulnar nerve is subjected to significant dynamic stresses during normal upper extremity function. Elbow flexion profoundly alters the spatial and volumetric parameters of the cubital tunnel. Studies utilizing advanced imaging and cadaveric models have demonstrated that full elbow flexion decreases the cross-sectional area of the cubital tunnel by up to 55%. Simultaneously, the cubital tunnel retinaculum becomes taut, and the medial head of the triceps pushes the nerve medially, increasing intraneural pressure from a resting baseline of approximately 7 mm Hg to over 20 mm Hg. When combined with contraction of the FCU, this pressure can exceed 200 mm Hg.
Furthermore, elbow flexion places substantial longitudinal traction on the nerve, elongating it by 4.7 to 8.0 mm. This elongation compromises the intraneural microcirculation. The vasa nervorum are uniquely susceptible to stretch; elongation of merely 8% can impede venous outflow, while 15% elongation results in complete arterial ischemia. Prolonged or repetitive flexion, therefore, induces transient ischemia, which triggers a cascade of intraneural edema, localized demyelination, impaired axonal transport, and eventual Wallerian degeneration of the affected fascicles. This ischemia-edema cycle is the fundamental pathophysiological driver of cubital tunnel syndrome.
Exhaustive Indications and Contraindications
The decision-making process for ulnar nerve interventions requires a nuanced synthesis of clinical severity, electrodiagnostic findings, anatomical variations, and patient-specific functional demands. The severity of cubital tunnel syndrome dictates the treatment algorithm, generally guided by the McGowan-Dellon classification system. Conservative management is uniformly indicated as the first-line treatment for Grade I (mild) and early Grade II (moderate) dysfunction, provided there is no evidence of rapid progressive motor loss. Surgical intervention is indicated upon the failure of a rigorous 3-to-6-month trial of non-operative management, or immediately upon presentation with Grade III (severe) dysfunction characterized by profound intrinsic atrophy, clawing, or a positive Wartenberg's sign.
When surgical decompression is indicated, the choice between in situ decompression and anterior transposition is dictated by specific anatomical and clinical criteria. Simple in situ decompression is the procedure of choice for primary, uncomplicated cubital tunnel syndrome. It preserves the segmental blood supply, minimizes surgical trauma, and allows for rapid rehabilitation. Conversely, anterior transposition (subcutaneous, intramuscular, or submuscular) is specifically indicated for patients with a hypermobile or subluxating ulnar nerve, significant cubitus valgus deformity, severe osteoarthritis with osteophyte impingement in the retroepicondylar groove, or in the revision setting where extensive perineural fibrosis mandates moving the nerve to an unscarred, well-vascularized bed.
For severe, high ulnar nerve injuries (e.g., proximal lacerations, severe crush injuries, or delayed presentations of proximal neurotmesis), primary repair or nerve grafting alone is often insufficient for intrinsic hand recovery. In these scenarios, the AIN to deep motor branch of the ulnar nerve transfer is strongly indicated. The ideal window for this nerve transfer is within 6 to 9 months post-injury, before irreversible motor endplate fibrosis occurs. It is also indicated in severe, end-stage cubital tunnel syndrome where profound intrinsic atrophy is present and proximal decompression alone is unlikely to reverse the distal motor deficit in a timely manner (a "supercharge" end-to-side or end-to-end transfer).
Absolute contraindications to nerve transfer include a concomitant high median nerve injury or a brachial plexus lesion that compromises the donor AIN. Relative contraindications include prolonged delay from injury (typically >12-18 months), severe pre-existing intrinsic muscle fibrosis, or significant generalized polyneuropathy that impairs nerve regeneration.
Table of Indications and Contraindications
| Procedure | Primary Indications | Contraindications (Absolute & Relative) |
|---|---|---|
| Conservative Management | McGowan Grade I/II CuTS; Intermittent paresthesias; Normal or mildly abnormal EMG/NCS. | Absolute: Progressive motor deficit; Profound intrinsic atrophy (Grade III). |
| In Situ Decompression | Primary, uncomplicated CuTS failing conservative care; Stable ulnar nerve in flexion. | Absolute: Subluxating nerve; Valgus deformity; Severe bony impingement. Relative: Revision surgery. |
| Anterior Transposition | Subluxating ulnar nerve; Cubitus valgus; Osteophyte formation; Revision decompression. | Absolute: None. Relative: High risk of poor wound healing (for submuscular); Medial epicondylitis. |
| AIN to Ulnar Nerve Transfer | High ulnar nerve injury (<9 months old); Severe intrinsic atrophy; "Supercharge" for severe CuTS. | Absolute: Concomitant high median nerve injury; Donor AIN dysfunction. Relative: Injury >12-18 months old. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of successful ulnar nerve surgery. The clinical evaluation must systematically differentiate ulnar neuropathy at the elbow from cervical radiculopathy (C8-T1), thoracic outlet syndrome, or distal compression at Guyon's canal. Provocative testing, including a positive Tinel's sign at the cubital tunnel and the elbow flexion test (sustained flexion with wrist extension for 60 seconds), are highly sensitive. Motor evaluation must quantify grip and pinch strength, and specifically assess for a positive Froment's sign (compensatory thumb interphalangeal joint flexion due to adductor pollicis weakness) and Wartenberg's sign (abducted posture of the small finger due to unopposed extensor digiti minimi action and weak third palmar interosseous).
Electrodiagnostic studies (EMG and NCS) are mandatory. They confirm the diagnosis, localize the lesion, assess the severity of axonal loss, and rule out double-crush syndromes. In cubital tunnel syndrome, a focal slowing of motor conduction velocity across the elbow to less than 50 m/s, or a drop of >10 m/s compared to the forearm segment, is diagnostic. Electromyography provides critical prognostic information; the presence of fibrillation potentials and positive sharp waves in the intrinsic muscles indicates active denervation and Wallerian degeneration, elevating the urgency of surgical intervention. Advanced imaging, specifically high-resolution ultrasound, is increasingly utilized to measure the cross-sectional area (CSA) of the nerve; a CSA greater than 10 mm² at the medial epicondyle is highly specific for compression.
Patient positioning and operating room setup vary depending on the planned procedure. For cubital tunnel decompression, the patient is positioned supine with the arm abducted, externally rotated, and supported on a radiolucent hand table. A non-sterile tourniquet is applied high on the brachium. The surgeon typically sits on the axillary side of the arm. For the AIN to ulnar nerve transfer, the setup is similar, but the focus is on the distal forearm and wrist. An operating microscope with a dual-head setup is essential for the intraneural dissection and coaptation, and microsurgical instruments (jeweler's forceps, microscissors, micro-needle holders) must be meticulously prepared.
Careful marking of anatomical landmarks is critical. For the elbow, the medial epicondyle, olecranon, and the course of the medial antebrachial cutaneous (MABC) nerve are marked. The MABC nerve typically crosses the surgical field 2 to 3 cm distal to the medial epicondyle and is highly susceptible to iatrogenic injury, which can result in a painful neuroma. For the distal forearm, the course of the ulnar artery and the FCU tendon are delineated to guide the approach to Guyon's canal and the distal ulnar nerve.
Step-by-Step Surgical Approach and Fixation Technique
In Situ Ulnar Nerve Decompression at the Cubital Tunnel
The in situ decompression is performed through a 4 to 6 cm longitudinal incision centered over the retroepicondylar groove, slightly posterior to the medial epicondyle to avoid the anterior branches of the MABC nerve. The subcutaneous tissues are sharply divided. The MABC nerve branches are identified, carefully mobilized, and protected with vessel loops. The common fascia overlying the cubital tunnel is incised.
The decompression begins proximally by identifying the ulnar nerve proximal to the medial epicondyle. The arcade of Struthers and the medial intermuscular septum are palpated and, if tight, released. The dissection then proceeds distally, dividing the cubital tunnel retinaculum (Osborne's ligament). The surgeon must then follow the nerve into the forearm, releasing the fascial band between the two heads of the FCU and the deep flexor-pronator aponeurosis.
Crucially, the nerve must not be circumferentially dissected or aggressively mobilized from its bed. The extrinsic blood supply, entering via the mesoneurium, must be preserved to prevent ischemic fibrosis. Once the decompression is complete from 8 cm proximal to 6 cm distal to the medial epicondyle, the elbow is taken through a full range of motion. The nerve is directly visualized to ensure it does not subluxate anterior to the medial epicondyle. If subluxation occurs, the procedure must be converted to an anterior transposition.
AIN to Deep Motor Branch of Ulnar Nerve Transfer
For high ulnar nerve injuries with absent intrinsic function, the distal nerve transfer is executed.
Step 1: Positioning and Incision
The patient is positioned supine with the arm extended on a hand table. A tourniquet is applied to the proximal arm. A longitudinal incision is made over the ulnar neurovascular bundle in the distal third of the forearm, extending distally across the wrist crease into the Guyon canal.
Step 2: Exposure of the Ulnar Nerve and Guyon's Canal
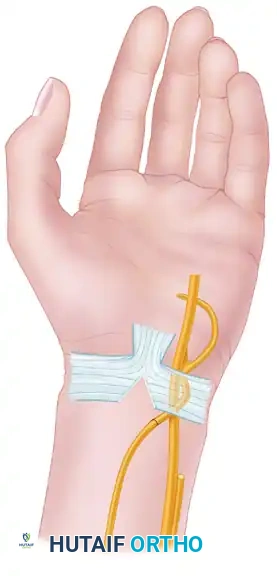
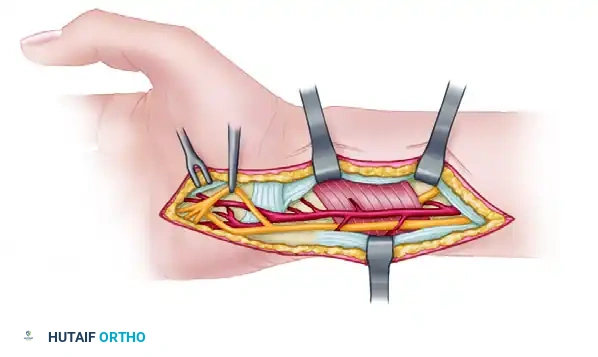
The incision is deepened through the subcutaneous tissue. The volar carpal ligament is incised to decompress Guyon's canal fully. The ulnar neurovascular bundle is identified. The ulnar artery is carefully retracted radially to expose the underlying ulnar nerve.
Step 3: Intraneural Dissection of the Ulnar Nerve
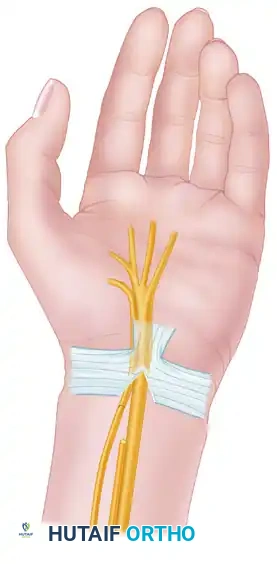
The bifurcation of the ulnar nerve into its superficial sensory branch and deep motor branch is identified within the palm, as it curves around the pisiform and hook of the hamate. Using the operating microscope, a meticulous intraneural neurolysis is performed. The epineurium is opened, and the motor fascicles are separated from the sensory fascicles proximally into the distal forearm, up to the level of the proximal border of the pronator quadratus. The topography of the ulnar nerve in the distal forearm is highly predictable; the motor fascicles are typically located in the ulnar-dorsal quadrant.
Step 4: Identification and Harvest of the AIN
The flexor tendons (FDP and FDS) are retracted radially to expose the pronator quadratus muscle. The terminal motor branch of the AIN is identified coursing along the interosseous membrane and entering the undersurface of the pronator quadratus. It is dissected distally into the muscle belly to maximize length, and then transected at its terminal branching point.
Step 5: Nerve Coaptation
The isolated ulnar motor fascicles are transected proximally, ensuring enough length on the distal stump to allow for a tension-free swing toward the AIN. The distal stump of the ulnar motor branch and the proximal stump of the AIN are brought together. Under operating microscope guidance, an epineurial/perineurial repair is performed using 9-0 or 10-0 nylon sutures. Fibrin glue is frequently applied to augment the repair, reducing the number of sutures required and minimizing foreign body reaction.
The tourniquet is deflated, meticulous hemostasis is achieved, and the wound is closed in layers without tension.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following ulnar nerve surgery can occur and require prompt recognition and management. The most common complication following any open elbow procedure is injury to the medial antebrachial cutaneous (MABC) nerve. Neuromas of the MABC are notoriously painful, often presenting with severe hyperalgesia over the medial proximal forearm that is exacerbated by elbow extension.
Persistent or recurrent symptoms following cubital tunnel decompression occur in 10% to 15% of patients. This may be due to incomplete initial release (most commonly at the deep flexor-pronator aponeurosis or the arcade of Struthers), iatrogenic subluxation of the nerve leading to friction neuritis, or extensive perineural scarring resulting from aggressive devascularization during the primary surgery. In cases of failed primary in situ decompression, revision surgery typically involves an anterior submuscular transposition to place the nerve in a pristine, vascularized bed.
For nerve transfers, the primary complication is failure of reinnervation. If intrinsic function does not return within 12 to 18 months following an AIN to ulnar nerve transfer, the procedure is considered a failure. This may be due to tension at the coaptation site, poor fascicular matching, or irreversible endplate degradation prior to axonal arrival. In these scenarios, salvage management relies on palliative tendon transfers to restore pinch strength and correct clawing.
Table of Complications and Salvage Management
| Complication | Estimated Incidence | Etiology/Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| MABC Nerve Neuroma | 5% - 10% | Iatrogenic transection or traction during elbow exposure. | Excision of neuroma and burying the proximal stump into the triceps or brachialis muscle. |
| Recurrent CuTS Symptoms | 10% - 15% | Incomplete release; Iatrogenic subluxation; Perineural fibrosis. | Revision surgery with anterior submuscular transposition; Neurolysis. |
| Nerve Transfer Failure | 10% - 20% | Tension at repair; Delayed surgery (>12 mos); Severe pre-existing atrophy. | Tendon transfers (e.g., Zancolli lasso for clawing; ECRB to adductor pollicis for pinch). |
| Medial Epicondyle Pain | 5% - 30% (Post-Epicondylectomy) | Over-resection of epicondyle; MCL complex destabilization. | Conservative management (NSAIDs, PT); Rarely requires ligamentous reconstruction. |
| Hematoma / Infection | < 2% | Inadequate hemostasis post-tourniquet deflation; Poor wound care. | Evacuation of hematoma; Intravenous antibiotics; Surgical debridement if deep. |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation trajectory is highly dependent on the specific surgical procedure performed. A tailored, phased approach is critical to optimize nerve gliding, prevent restrictive adhesions, and facilitate motor re-education.
Rehabilitation Post-Cubital Tunnel Decompression
For patients undergoing simple in situ decompression, the rehabilitation protocol is accelerated. The surgical dressing is removed after 3 to 5 days, and immediate active and passive range of motion of the elbow, wrist, and hand is initiated. No splinting is required. Patients are instructed in nerve gliding exercises to prevent adherence of the ulnar nerve to the surgical bed. Heavy lifting and forceful gripping are restricted for 4 weeks to allow the soft tissues to heal.
If an anterior transposition (particularly submuscular) is performed, a brief period of immobilization is necessary to protect the flexor-pronator mass repair. The elbow is placed in a posterior splint at 90 degrees of flexion with the forearm in neutral for 10 to 14 days. Following splint removal, a graduated range of motion program is initiated, avoiding aggressive terminal extension and combined wrist/finger extension that places tension on the flexor-pronator origin. Strengthening begins at 6 weeks post-operatively.
Rehabilitation Post-AIN to Ulnar Nerve Transfer
The post-operative protocol for distal nerve transfers deviates significantly from traditional nerve repair paradigms. Because the nerve coaptation is performed in a tension-free manner within the well-vascularized bed of the distal forearm, immobilization is strictly avoided. Post-operatively, no splinting is utilized. The patient is encouraged to begin immediate active and passive range of motion of the wrist and fingers. Immediate motion prevents the formation of restrictive perineural adhesions at the coaptation site and facilitates necessary intrinsic stretching.
Motor re-education is the most critical component of the rehabilitation phase following a nerve transfer. Patients work closely with a specialized hand therapist to perform "donor activation" exercises. Because the AIN originally powered the pronator quadratus, the patient must initially activate the donor nerve by attempting to pronate the forearm. They are instructed to actively forcefully pronate against resistance while simultaneously attempting to abduct and adduct the fingers (ulnar intrinsic function). Initially, the patient will only achieve intrinsic contraction when actively pronating. Over a period of months, through targeted therapy and cortical plasticity, the brain remaps the motor pathways. The patient eventually learns to dissociate these movements, resulting in seamless, independent intrinsic hand function without the need for conscious forearm pronation.
Summary of Landmark Literature and Clinical Guidelines
The evolution of ulnar nerve surgery is heavily grounded in landmark clinical literature and rigorous randomized controlled trials. For cubital tunnel syndrome, the shift away from routine transposition was solidified by several key studies. A landmark meta-analysis by Macadam et al. (2008) reviewed randomized controlled trials comparing simple decompression to anterior transposition. The study concluded that there was no statistically significant difference in motor or sensory outcomes between the two techniques for primary CuTS, but simple decompression was associated with fewer complications and a faster return to work. Similarly, prospective randomized studies by Bartels et al. and Nabhan et al. reinforced that in situ decompression yields equivalent long-term clinical outcomes with reduced surgical morbidity, establishing it as the current gold standard for uncomplicated cases.
In the realm of reconstructive microsurgery, the AIN to ulnar motor nerve transfer is a relatively modern triumph. Mackinnon and Novak (1999) first described the anatomical feasibility and early clinical success of transferring the terminal AIN to the deep motor branch of the ulnar nerve. Their work demonstrated that bypassing the proximal zone of injury could salvage intrinsic hand function that was previously considered lost. In 2002, Haase and Chung corroborated the efficacy of this technique in a broader clinical series, reporting excellent return of intrinsic function and pinch strength with negligible donor site morbidity.
Current clinical guidelines from the American Society for Surgery of the Hand (ASSH) and the American Association of Neuromuscular & Electrodiagnostic Medicine (AANEM) emphasize the critical role of pre-operative electrodiagnostic testing in guiding surgical decision-making. Future directions in ulnar nerve management are exploring the use of bioabsorbable nerve conduits, processed nerve allografts for short-gap reconstructions, and the localized application of neurotrophic factors and immunosuppressants (such as topical tacrolimus) to accelerate axonal regeneration and improve functional outcomes in severe neuropathies.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is designed to assist ortho ---
