Interfascicular Nerve Grafting: Surgical Techniques and Protocols

Key Takeaway
Interfascicular nerve grafting is the gold standard for bridging peripheral nerve defects where tension-free primary repair is impossible. Pioneered by Millesi, this microsurgical technique relies on precise fascicular alignment and tensionless coaptation using autologous donor grafts, most commonly the sural nerve. Success demands meticulous intraneural dissection, accurate fascicular mapping, and rigorous postoperative rehabilitation to optimize axonal regeneration and functional recovery.
Comprehensive Introduction and Patho-Epidemiology
The fundamental principle of peripheral nerve surgery dictates that a primary repair or graft coaptation must be entirely free of tension. Biomechanical and microvascular studies have conclusively demonstrated that tension across a nerve repair site exceeding 8% to 10% of the nerve's resting length induces a critical reduction in intraneural blood flow. When tension exceeds 15%, the result is complete ischemia of the nerve ends, leading to profound intraneural fibrosis, dense scarring at the coaptation site, and the ultimate failure of axonal regeneration. In the context of significant peripheral nerve trauma, tumor resection, or delayed presentations where gap formation is inevitable, bridging the defect without tension is paramount to restoring functional continuity.
When a peripheral nerve defect is too large to permit a tension-free primary end-to-end neurorrhaphy, interfascicular nerve grafting becomes the definitive gold standard of treatment. Pioneered and popularized by Hanno Millesi in the 1970s, the interfascicular grafting technique represents a paradigm shift in peripheral nerve microsurgery. It abandons the historically flawed concept of bulk epineurial approximation under tension in favor of precise, tensionless coaptation of individual fascicles or fascicular groups using autologous nerve grafts. This meticulous technique maximizes the cross-sectional area of precise axonal alignment, minimizes the misdirection of regenerating motor and sensory fibers, and significantly mitigates the fibrotic response by excising redundant, scar-producing epineurial tissue.
The patho-epidemiology of peripheral nerve gaps requiring interfascicular grafting is broad and encompasses high-energy trauma, blast injuries, extensive crush injuries, and iatrogenic transections. High-velocity gunshot wounds and severe traction injuries (such as those seen in brachial plexus avulsions) frequently result in extensive zones of injury that undergo Wallerian degeneration and subsequent fibrotic replacement. Delayed presentations of nerve injuries often reveal a neuroma-in-continuity or a massive terminal neuroma, necessitating extensive resection back to healthy, viable fascicular tissue. The resulting gap, which may span several centimeters, cannot be overcome by joint positioning or nerve mobilization alone without compromising the microvascular integrity of the nerve. Consequently, the surgeon must rely on interfascicular autografting to provide a biologically viable, structurally sound conduit for advancing axonal growth cones.
Understanding the temporal dynamics of nerve injury is equally critical. Following transection, the distal nerve segment undergoes Wallerian degeneration, characterized by the breakdown of axons and myelin sheaths, while Schwann cells proliferate to form the bands of Büngner. Simultaneously, the target end-organs (motor endplates and sensory receptors) begin to atrophy. Motor endplates typically become irreversibly fibrotic and refractory to reinnervation after 18 to 24 months of denervation. Therefore, interfascicular grafting must be performed within an optimal therapeutic window—ideally between 3 weeks and 3 months post-injury, once the zone of injury has declared itself, but well before irreversible target organ atrophy ensues.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of intraneural topography and biomechanics is mandatory before undertaking interfascicular grafting. The internal architecture of a peripheral nerve is not a static bundle of cables; rather, it is a highly dynamic, undulating plexus of fascicles that divide, anastomose, and migrate as they traverse the extremity. The connective tissue framework of the nerve consists of the mesoneurium (allowing longitudinal excursion), the external epineurium (providing structural integrity), the internal or interfascicular epineurium (cushioning the fascicles), the perineurium (the critical blood-nerve barrier providing tensile strength), and the endoneurium (surrounding individual axons).
Millesi stressed the critical importance of recognizing that most cross-sections of peripheral nerves exhibit one of four distinct fascicular patterns. Identifying these patterns at the proximal and distal stumps under high-power microscopic magnification is the foundational first step in successful graft mapping and execution.
Monofascicular Nerves
These nerves consist of a single, large fascicle enveloped by a robust layer of epineurium. They are typically found in the distal terminal branches of peripheral nerves, such as the digital nerves in the hand or the terminal motor branches entering a muscle belly. Grafting these nerves is straightforward, requiring a single graft of appropriate caliber.

Oligofascicular Nerves
These nerves contain a small number of relatively large, distinct fascicles. Dissection, identification, and group matching in oligofascicular nerves are generally straightforward, making them highly amenable to precise interfascicular grafting with minimal mismatch.

Polyfascicular Nerves with Group Arrangements
In this pattern, numerous smaller fascicles are clustered into distinct, identifiable groups separated by robust interfascicular epineurium. This is the most common pattern encountered in major mixed motor-sensory nerves (e.g., the median, ulnar, or radial nerves in the proximal forearm) and is highly amenable to group interfascicular grafting, where each graft bridges a specific functional group.

Polyfascicular Nerves without Group Arrangements
This is the most complex and surgically demanding pattern, characterized by numerous small fascicles scattered diffusely throughout the cross-section without distinct grouping or functional segregation. Matching these fascicles requires meticulous clinical estimation, intraoperative electrical stimulation (if performed acutely), and often necessitates grouping them artificially based on regional quadrants to facilitate grafting.

Biomechanically, peripheral nerves exhibit complex viscoelastic properties, including creep and stress relaxation, which allow them to accommodate joint motion. However, a free nerve graft lacks the intrinsic vascularized mesoneurium of a native nerve. It relies entirely on plasmatic imbibition from the surrounding soft tissue bed for the first 72 to 96 hours before neovascularization occurs. If a graft is placed under any tension, the delicate fibrin clot at the coaptation site will fail, the graft will undergo ischemic necrosis, and the resulting scar tissue will form an impenetrable barrier to the regenerating growth cones. Thus, the biomechanical imperative of interfascicular grafting is absolute redundancy; the graft must be long enough to lie sinuously within the nerve bed, accommodating full joint excursion without transmitting any tensile load to the micro-sutures.
Exhaustive Indications and Contraindications
The decision to proceed with interfascicular nerve grafting requires a comprehensive evaluation of the patient's injury pattern, the physiological state of the denervated targets, and the availability of suitable donor tissue. The primary indication for this procedure is a peripheral nerve defect that cannot be closed primarily without exceeding the critical tension threshold. Attempting to force a primary repair through extreme joint flexion or aggressive, extensive nerve mobilization is widely condemned in modern microsurgery, as it invariably leads to joint contractures, ischemic nerve failure, and devastating functional outcomes.
Interfascicular grafting is indicated in both acute and delayed settings. In acute high-energy trauma with segmental nerve loss, grafting is often delayed for 3 to 6 weeks. This delay allows the true extent of the intraneural injury (the zone of trauma) to declare itself, ensuring that the surgeon resects back to unequivocally healthy fascicles. In delayed presentations, such as a symptomatic neuroma-in-continuity that fails to demonstrate action potentials across the lesion on intraoperative nerve monitoring, resection and interfascicular grafting are definitively indicated. Furthermore, grafting is the cornerstone of complex reconstructive procedures, including brachial plexus exploration and targeted muscle reinnervation (TMR), where specific fascicular groups must be redirected to distinct anatomical targets.
Contraindications to interfascicular nerve grafting must be strictly observed to prevent surgical failure and unnecessary donor site morbidity. Absolute contraindications include the presence of an active, untreated infection in the recipient bed, which will inevitably destroy the avascular graft. Similarly, attempting to graft a motor nerve when the target muscle has undergone irreversible fibrotic degeneration (typically >18 to 24 months post-injury) is futile; in such cases, tendon transfers or free functioning muscle transfers are the appropriate reconstructive options. A severely scarred, avascular recipient bed that cannot support plasmatic imbibition is also a contraindication, necessitating prior soft tissue reconstruction with a vascularized flap before nerve grafting can be considered.
| Category | Specific Indications / Contraindications | Clinical Rationale and Surgical Considerations |
|---|---|---|
| Absolute Indications | Nerve gaps > 2.0 - 2.5 cm | Primary repair impossible without ischemic tension; bridging required. |
| Absolute Indications | Failed primary neurorrhaphy | Dense scar formation requires wide resection and subsequent grafting. |
| Absolute Indications | Neuroma-in-continuity (non-conducting) | Resection of fibrotic segment is mandatory to restore axonal pathways. |
| Relative Indications | Gaps 1.0 - 2.0 cm in critical areas | If joint positioning causes tension, a short graft is preferred over a tight primary repair. |
| Absolute Contraindications | Active recipient bed infection | Purulent environments rapidly destroy avascular free nerve grafts. |
| Absolute Contraindications | Irreversible motor endplate atrophy | >18-24 months post-injury; axons will reach fibrotic muscle incapable of contraction. |
| Absolute Contraindications | Avascular soft tissue bed | Graft relies on plasmatic imbibition; requires preliminary flap coverage. |
| Relative Contraindications | Severe patient comorbidities | Poor microvascular flow (e.g., severe uncontrolled diabetes, heavy smoking) impairs graft survival. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the bedrock of successful interfascicular nerve grafting. The clinical evaluation must precisely map the sensory and motor deficits to localize the lesion and estimate the functional groups involved. Electrodiagnostic studies (EMG and NCS) are indispensable; baseline studies are typically obtained at 3 to 4 weeks post-injury to confirm the presence of Wallerian degeneration and rule out neurapraxia. Serial EMGs help monitor for any spontaneous reinnervation, which might alter the surgical plan. Advanced imaging modalities, particularly high-resolution ultrasound and Magnetic Resonance Neurography (MRN), have revolutionized preoperative templating. These tools allow the surgeon to visualize the neuroma, measure the anatomical gap, assess the quality of the proximal and distal nerve segments, and accurately plan the required length of donor nerve harvest.
The selection of the ideal donor nerve is a critical component of preoperative planning. The donor must provide sufficient length, possess a favorable fascicular architecture (preferably oligofascicular or polyfascicular with minimal connective tissue), and result in a predictable, well-tolerated donor site morbidity. While the medial antebrachial cutaneous nerve, lateral antebrachial cutaneous nerve, and superficial branch of the radial nerve are viable options for upper extremity defects, the sural nerve remains the undisputed workhorse for interfascicular grafting.
The sural nerve provides up to 30 to 40 cm of high-quality graft material, boasts an excellent ratio of axonal tissue to epineurial connective tissue, and its harvest results in a clinically insignificant area of numbness over the lateral aspect of the foot. The nerve is located posterolateral to the lateral malleolus, running in close proximity to the lesser saphenous vein. Preoperative marking of the sural nerve course and the planned incisions is essential.

Patient positioning is dictated by the location of both the recipient site and the donor site. For upper extremity reconstructions utilizing sural nerve autografts, the patient is typically placed supine. The ipsilateral or contralateral lower extremity is prepped and draped freely to allow access to the posterior calf. A bump may be placed under the hip to internally rotate the leg, facilitating exposure of the posterolateral ankle and calf. The use of dual surgical teams—one preparing the recipient bed and the other harvesting the graft—significantly reduces operative time and tourniquet ischemia. The operating microscope must be positioned ergonomically to allow the primary surgeon and assistant unhindered access to the operative field, as the interfascicular coaptation phase requires intense concentration and absolute immobility.
Step-by-Step Surgical Approach and Fixation Technique
1. Preparation and Neuroma Excision
The surgical approach begins with the exposure and dissection of the injured nerve in a completely bloodless field, utilizing a well-padded pneumatic tourniquet. Dissection must strictly proceed from healthy, unscarred tissue proximally and distally, converging toward the central zone of injury. This "outside-in" approach prevents inadvertent iatrogenic injury to the nerve embedded in dense scar tissue.
Once the neuroma at the proximal stump and the glioma at the distal stump are isolated, they must be meticulously excised. Using a fresh diamond knife, a specialized nerve-cutting instrument, or a sterile wooden tongue depressor as a cutting block, the surgeon sequentially sections the nerve ends in a process known as "bread-loafing." This continues until healthy, pouting fascicles are visualized, completely free of interfascicular fibrosis and exhibiting a characteristic "mushrooming" appearance from the epineurial sleeve.
Following complete resection, the tourniquet must be deflated. Achieving absolute hemostasis in the recipient bed is critical; any postoperative hematoma will organize into a fibrotic scar, creating an impenetrable mechanical barrier to regenerating axons and potentially causing compressive ischemia of the free graft.
2. Fascicular Mapping and Graft Harvest
With the healthy nerve stumps exposed, the surgeon creates a detailed intraoperative sketch of the cross-sectional ends. Fascicular mapping involves identifying corresponding groups in the distal stump by evaluating the size, number, and spatial arrangement of fascicles within the proximal stump. While reliable over short defects, mapping over long gaps requires profound anatomical knowledge and clinical estimation due to the complex internal plexus formation.
Simultaneously, the sural nerve is harvested. While minimally invasive nerve strippers are available, harvesting the nerve through a single, continuous longitudinal incision (or a series of stepped incisions) is strongly recommended by purists. This open technique facilitates the removal of the nerve with minimal trauma, preventing the traction injuries, intraneural hemorrhage, and inadvertent transection of branches that frequently occur with blind stripping.

3. Graft Preparation and Sizing
Once harvested, the nerve graft must be kept continuously moist with Ringer's solution or saline to prevent desiccation, which rapidly destroys the delicate Schwann cells. A critical surgical pitfall is cutting the graft too short. The nerve graft must be cut into sections that are 10% to 15% longer than the measured defect, measured with the adjacent joints fully extended. This redundancy compensates for the natural shrinkage of the free graft and accommodates the normal excursion of the nerve bed during postoperative joint movement.
Using a diamond knife under the microscope, the graft is gently transected. It is imperative to meticulously excise any redundant epineurial and areolar connective tissue from the ends of the graft. If this tissue drapes over the fascicles, it will physically block axonal crossing and promote scar formation.
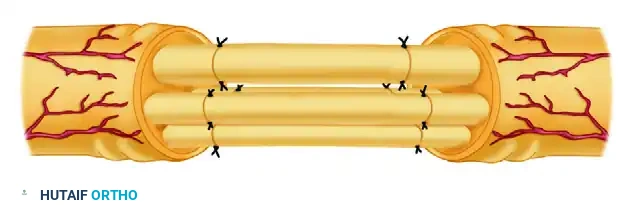
4. Interfascicular Coaptation
The prepared nerve grafts are then interposed between the proximal and distal nerve stumps. Referring to the intraoperative sketch, the surgeon determines the precise spatial orientation for each graft segment to bridge specific functional groups.

The goal is exact, tensionless coaptation. The surgeon utilizes a single 10-0 or 11-0 monofilament nylon suture on a micro-spatula needle for each end of the graft. The needle passes through the epineurium of the graft and anchors deeply into the perineurium of the host fascicle, or into the robust interfascicular connective tissue of the host group.
Because the repair is entirely tension-free, multiple sutures are contraindicated. Excessive suturing introduces foreign body material, inciting a profound inflammatory response and subsequent fibrosis. The natural fibrin clot that forms within minutes provides significant adhesive stability. If alignment is imperfect, the graft is rotated around the axis of the primary suture, and a maximum of one or two additional micro-sutures are placed. Fibrin tissue adhesive may be applied as an adjunct to seal the coaptation site and provide additional mechanical stability without the inflammatory burden of sutures.
5. Wound Closure and Drainage
Wound closure must be executed with extreme care to ensure the grafts are not displaced by shearing forces from the overlying soft tissues. The soft tissue bed must be highly vascularized to support the graft. If skin closure is tight, particularly in the distal forearm or ankle, shearing forces will easily disrupt the delicate 10-0 repairs. In such scenarios, relaxing incisions or the application of a split-thickness skin graft over a secondary defect is mandated to ensure zero pressure on the primary graft site. Active suction drainage is strictly avoided, as the negative pressure will disrupt the interfascicular coaptations and aspirate the stabilizing fibrin clot; passive Silastic drains are utilized if necessary.
Complications, Incidence Rates, and Salvage Management
Despite flawless microsurgical technique, interfascicular nerve grafting carries inherent risks, primarily due to the complex biology of axonal regeneration and the reliance on a free, avascular graft. Complications can arise at the donor site, within the recipient bed, or at the micro-coaptation interfaces. Recognizing these complications early and understanding the algorithms for salvage management are critical competencies for the peripheral nerve surgeon.
The most devastating complication is graft necrosis, which typically results from a highly scarred, avascular recipient bed, postoperative hematoma formation, or placing the graft under tension. This leads to complete failure of axonal transit. Another significant challenge is the "Distal Block," a phenomenon where regenerating axons successfully traverse the proximal coaptation and the length of the graft, but are halted by dense fibrosis at the distal suture line. This is often detected clinically when the advancing Tinel's sign arrests at the distal end of the graft for several months without further progression.
Donor site morbidity, while generally well-tolerated, can include painful neuromas at the transection site of the sural nerve, delayed wound healing, or hyperesthesia in the distribution of the harvested nerve. Meticulous handling of the proximal donor stump—burying it deep within a muscle belly or capping it—is essential to minimize symptomatic neuroma formation.
| Complication | Estimated Incidence | Etiology and Clinical Presentation | Salvage Strategy and Management |
|---|---|---|---|
| Graft Necrosis / Failure | 5% - 10% | Avascular bed, tension, or hematoma. Presents as complete absence of advancing Tinel's sign. | Re-exploration, excision of necrotic graft, soft tissue coverage (flap), and re-grafting. |
| The "Distal Block" | 10% - 15% | Fibrosis at the distal coaptation site. Tinel's sign arrests distally for >3-4 months. | Surgical re-exploration, resection of the fibrotic distal suture line, and secondary end-to-end repair. |
| Painful Donor Site Neuroma | 5% - 8% | Unprotected proximal stump of the harvested nerve (e.g., sural). | Resection of the neuroma, burying the stump deep into adjacent muscle (e.g., gastrocnemius), or TMR. |
| Postoperative Hematoma | 2% - 5% | Inadequate hemostasis post-tourniquet deflation. Causes compressive ischemia. | Immediate surgical evacuation, meticulous hemostasis, and re-evaluation of graft integrity. |
| Joint Contracture | 5% - 12% | Prolonged immobilization or failure to initiate early gliding exercises. | Aggressive physical therapy, dynamic splinting, and rarely, surgical capsular release. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following interfascicular nerve grafting is a delicate balance between protecting the fragile micro-coaptations during the initial healing phase and initiating early motion to prevent restrictive perineurial adhesions and joint contractures. A highly structured, phased protocol managed by a specialized hand or occupational therapist is mandatory for optimal functional recovery.
Phase I: Immobilization and Stabilization (Days 1 to 10)
The immediate postoperative phase is critical for the survival and stabilization of the avascular nerve graft. The extremity is immobilized in a well-padded, custom-molded plaster or fiberglass splint in the exact position that was maintained throughout the surgical procedure. The part is strictly immobilized for 8 to 10 days. This crucial period allows the initial fibrin clot at the coaptation sites to organize into early, stable collagenous tissue, and permits the onset of plasmatic imbibition from the surrounding wound bed. Strict elevation is enforced to minimize edema, and any signs of excessive pain must prompt an evaluation for hematoma formation, which requires immediate evacuation to prevent compressive ischemia.
Phase II: Early Mobilization and Nerve Gliding (Weeks 2 to 4)
After 8 to 10 days, the static splint is removed, and a carefully monitored program of free motion of the adjacent joints is permitted. Formal physical therapy, consisting of active and active-assisted range-of-motion exercises, is instituted. The primary goal during this phase is to encourage the longitudinal gliding of the nerve bed. Controlled excursion of the nerve prevents the formation of dense, restrictive adhesions between the graft and the surrounding soft tissues, which could tether the nerve and induce chronic traction injuries during normal limb use. If a skin graft or local flap was utilized for closure, its viability must be meticulously monitored during mobilization.
Phase III: Axonal Tracking and Sensory/Motor Re-education (Months 1 to 24)
The progress of axonal regeneration is monitored clinically by observing the advancing Tinel sign, which is elicited by gently tapping along the course of the grafted nerve. Regenerating axons typically advance at a rate of approximately 1 mm per day (or 1 inch per month), though this rate is highly variable and influenced by the patient's age, metabolic status, the specific nerve involved, and the distance from the neuronal cell body.
As axons reach their target receptors, sensory re-education programs are initiated to help the cerebral cortex interpret the altered afferent signals. This involves structured stimulation using various textures, temperatures, and pressures. Concurrently, motor retraining utilizing biofeedback and targeted electrical muscle stimulation (EMS) is employed to maintain the viability of the muscle fibers and re-establish neuromuscular control as motor axons reinnervate the endplates. The patient must be educated that maximal functional recovery is a protracted process, often taking up to two years, and requires unwavering compliance with the rehabilitation protocol.
Summary of Landmark Literature and Clinical Guidelines
The modern practice of interfascicular nerve grafting is built upon decades of rigorous anatomical, biomechanical, and clinical research. The foundational principles were established by Hanno Millesi in the 1970s and 1980s. Millesi's landmark publications challenged the prevailing dogma of bulk epineurial repair under tension, definitively proving that tension is the primary enemy of nerve regeneration. His work on fascicular topography and the necessity of tension-free group fascicular grafting remains the cornerstone of peripheral nerve microsurgery today.
Sunderland's classification of nerve injury and his exhaustive anatomical studies on the internal topography of peripheral nerves provided the necessary mapping required for surgeons to align corresponding fascicular groups accurately. The understanding that the internal plexus is dynamic, changing its architectural arrangement every few millimeters, dictates the surgical reality that perfect fascicular matching over long gaps is an anatomical impossibility, reinforcing the need for group matching based on functional quadrants.
Contemporary clinical guidelines strongly endorse the use of autologous nerve grafts for critical gaps exceeding 2 to 3 centimeters. While recent advancements in bioengineering have introduced synthetic nerve conduits (e.g., polyglycolic acid, collagen tubes) and processed nerve allografts (which eliminate donor site morbidity), robust clinical evidence restricts their reliable use to non-critical sensory nerves or mixed nerve gaps shorter than 2 to 3 centimeters. For massive defects, high-energy trauma, and critical motor nerve reconstructions, the autologous interfascicular nerve graft, meticulously harvested and precisely coapted under microscopic magnification, remains the undisputed gold standard, offering the highest probability of restoring meaningful function to the devastated extremity.
📚 Medical References
- Interfascicular nerve grafting, Clin Orthop Relat Res 163:65, 1982.
- Pringle RM, Protheroe K, Mukherjee SK: Entrapment neuropathy of the sural nerve, J Bone Joint Surg 56B:465, 1974.
- [Riley DA, Lang DH: Carbonic anhydrase activity of human peripheral nerves: a possible histochemical aid to nerve repair, J Hand Surg 9A:112, 1984.](https://pubmed.ncbi.nlm.nih.gov/?term=Riley%20DA%2C%20Lang%20DH%3A%20Carbonic%20anhydrase%20activity%20of%20human%20peripheral%20nerves%3A%20a%20possible%20histochemical%20aid%20to%20nerve%20repair%2C%20J%20Hand%2
